
Autoimmune diseases are not always recognized as urgent health issues, despite a worldwide prevalence of 4%–5%. Most estimates come from high-income countries, as low- and middle-income countries face more issues of under-reporting. Despite this and the lack of recognition under current reporting practices, the role these diseases play in mortality must be acknowledged. In particular, considering multiple causes of death as opposed to a single cause of death results in a 1.5–4.2-fold increase in deaths classified as relating to autoimmune diseases, evidence of their share in overall mortality burden, a factor important for patient care and healthcare policy decision making. However, formulating such policies and programs for timely, appropriate diagnoses and care is stymied in low- and middle-income countries by the shortage of methodologically sound studies on mor tality from systemic autoimmune diseases. This limitation exacerbates inequalities and health gaps among patients in different countries and localities. Multiple cause-of-death methodology has been validated for research on other diseases and demonstrates the mortality burden of these illnesses in countries where traditional methodological approaches, primarily based on prospective cohort studies, are not feasible. Studying mortality from systemic autoimmune diseases by analyzing multiple causes of death with data from national mortality registries is a low-cost alternative to traditional mortality analysis. The objective of this paper is to demonstrate and defend the usefulness of this approach to estimate mortality burden.
KEYWORDS Autoimmune diseases, mortality, cause of death, Cuba

INTRODUCTION Hypoxic ischemic encephalopathy is a neurological condition occurring immediately after birth following a perinatal asphytic episode. Therapeutic hypothermia is a safe and effective intervention to reduce mortality and major disability in survivors. In Latin America, perinatal asphyxia is a major problem, but no data are available characterizing its current situation in the region or the impact of hypoxic ischemic encephalopathy on its management.
OBJECTIVE Understand the prevalence, mortality and use of therapeutic hypothermia in newborns at ≥36 weeks gestational age with hypoxic ischemic encephalopathy admitted to neonatal units reporting to the Ibero-American Society of Neonatology Network.
METHODS The Ibero-American Society of Neonatology Network groups various neonatology centers in Latin America that share information and collaborate on research and medical care. We evaluated data on newborns with ≥36 weeks gestational age reported during 2019. Each unit received a guide with definitions and questions based on the Society’s 7th Clinical Consensus. Evaluated were encephalopathy frequency and severity, Apgar score, need for resuscitation at birth, use of therapeutic hypothermia and clinical evolution at discharge. Our analysis includes descriptive statistics and comparisons made using the chi-square test.
RESULTS We examined reports of 2876 newborns from 33 units and 6 countries. In 2849 newborns with available data, hypoxic encephalopathy prevalence was 5.1% (146 newborns): 27 (19%) mild, 36 (25%) moderate, 43 (29%) severe, and 40 (27%) of unknown intensity. In those with moderate and severe encephalopathy, frequencies of Apgar scores ≤3 at the first minute (p = 0.001), Apgar scores ≤3 at the fifth minute (p <0.001) and advanced resuscitation (p = 0.007) were higher. Therapeutic hypothermia was performed in only 13% of newborns (19). Neonatal mortality from encephalopathy was 42% (61).
CONCLUSION Hypoxic ischemic encephalopathy is a neonatal condition that results in high mortality and severe neurological sequelae. In this study, the overall prevalence was 5.1% with a mortality rate of 42%. Although encephalopathy was moderate or severe in 54% of reported cases, treatment with hypothermia was not performed in 87% of newborns. These data reflect a regional situation that requires urgent action.
KEYWORDS Hypoxia ischemia, brain; encephalopathy, neonatal; mortality; hypothermia, induced; neonatology; Latin America
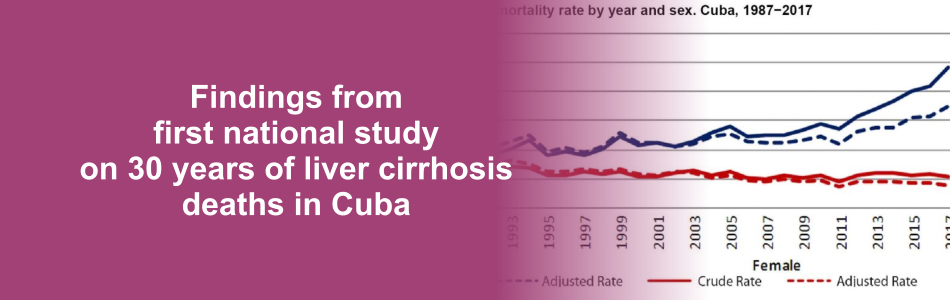
INTRODUCTION Cirrhosis of the liver is a chronic disease that is widespread and irreversible. It represents the final stage of numerous diseases that affect the liver. By the end of 2017, it was the 11th most common cause of death, with a loss of 41.4 million years of disability-adjusted life years, which represent 2.1% of the total years of life lost in the global mortality burden. In Cuba, cirrhosis and other chronic liver diseases have been among the top 10 causes of death for several decades, their rates consistently increasing, from 576 deaths in 1970 (6.7 per 100,000 population) to 1738 in 2017 (15.5 per 100,000 population), with a risk of death that is 4.6 times higher in men.
OBJECTIVE Characterize deaths from cirrhosis of the liver in Cuba from 1987 to 2017.
METHODS An ecological time-series study was conducted for 1987 to 2017 using information obtained from the mortality database of the Medical Records and Health Statistics Bureau of Cuba’s Ministry of Public Health. The study universe consisted of all deceased persons in the country whose underlying cause of death was cirrhosis of the liver. Both general mortality rates and specific mortality were calculated by age group, sex and etiological classification using adjusted and crude rates. Rates were age-adjusted using the direct method, and the population from the 2002 Census of Population and Housing was considered as the standard population. Percentages and means were also calculated according to selected variables and the relative risk of death due to the disease according to sex, age group and etiological classification. The trend and forecast for mortality rates were estimated for this disease.
RESULTS The crude mortality rate from cirrhosis of the liver was 9.0 per 100,000 population for the period. Those aged ≥75 years had the highest risk of death (48.3 per 100,000 population). The crude and adjusted mortality rates were almost double for men (12.4 vs. 5.6 and 11.7 vs. 5.6 per 100,000 population, respectively), as was the total relative risk of death, which was 2.2 times higher. Nonalcoholic cirrhosis accounted for 71.6% of deaths. By the end of 2017, risk of death from cirrhosis had climbed to 14.8 per 100,000 population (adjusted rate: 10.6 per 100,000 population), a signal that mortality had progressively increased over the 31 years analyzed. In addition, forecasts predict that death rates will continue their gradual increase, reaching 19.2 per 100,000 population in 2025.
CONCLUSIONS Deaths from cirrhosis of the liver constitute a substantial health burden in Cuba. The upward trend and forecast, in addition to increased risk of mortality in men and older adults, are similar to those reported internationally. The finding that most of these deaths result from nonalcoholic cirrhosis should be further studied, as formulation of effective public health strategies depends largely on attaining a better understanding of the etiology, progression and social determinants of the disease.
KEYWORDS Liver cirrhosis, alcoholic liver cirrhosis, fatty liver, mortality, Cuba
INTRODUCTION On March 11, 2020, WHO declared COVID-19 a pandemic and called on governments to impose drastic measures to fight it. It is vitally important for government health authorities and leaders to have reliable estimates of infected cases and deaths in order to apply the necessary measures with the resources at their disposal.
OBJECTIVE Test the validity of the logistic regression and Gompertz curve to forecast peaks of confirmed cases and deaths in Cuba, as well as total number of cases.
METHODS An inferential, predictive study was conducted using logistic and Gompertz growth curves, adjusted with the least squares method and informatics tools for analysis and prediction of growth in COVID-19 cases and deaths. Italy and Spain—countries that have passed the initial peak of infection rates—were studied, and it was inferred from the results of these countries that their models were applicable to Cuba. This hypothesis was tested by applying goodness-of-fit and significance tests on its parameters.
RESULTS Both models showed good fit, low mean square errors, and all parameters were highly significant.
CONCLUSIONS The validity of models was confirmed based on logistic regression and the Gompertz curve to forecast the dates of peak infections and deaths, as well as total number of cases in Cuba.
KEYWORDS COVID-19, SARS-CoV-2, logistic models, pandemic, mortality, Cuba
INTRODUCTION The scales available to predict death and complications after acute coronary syndrome include angiographic studies and serum biomarkers that are not within reach of services with limited resources. Such services need specific and sensitive instruments to evaluate risk using accessible resources and information.
OBJECTIVE Develop a scale to estimate and stratify the risk of intrahospital death in patients with acute ST-segment elevation myocardial infarction.
METHODS An analytical observational study was conducted in a universe of 769 patients with acute ST-segment elevation myocardial infarction who were admitted consecutively to the Camilo Cienfuegos Provincial Hospital in Sancti Spíritus Province, Cuba, from January 2013 to March 2018. The fi nal study cohort included 667 patients, excluding 102 due to branch blocks, atrial fibrillation, drugs that prolong the QT interval, low life expectancy or history of myocardial infarction. The demographic variables of age, sex, skin color, classic cardiovascular risk factors, blood pressure, heart rate, blood glucose level, in addition to duration and dispersion of the QT interval with and without correction, left ventricular ejection fraction, and glomerular filtration rate were included in the analysis. Patients were categorized according to the Killip-Kimball Classification for degree of heart failure. A risk scale was constructed, the predictive ability of which was evaluated using the detectability index associated with an receiver-operator curve.
RESULTS Seventy-seven patients died (11.5%). Mean blood glucose levels were higher among the deceased, while their systolic and diastolic blood pressure, left ventricular ejection fraction, and glomerular filtration rate were lower than those participants discharged alive. Relevant variables included in the scale were systolic blood pressure, Killip-Kimball class, cardiorespiratory arrest, glomerular filtration rate, corrected QT interval dispersion rate, left ventricular ejection fraction, and blood glucose levels. The variable with the best predictive ability was cardiorespiratory arrest, followed by a blood glucose level higher than 11.1 mmol/L. The scale demonstrated a great predictive ability with a detectability index of 0.92.
CONCLUSIONS The numeric scale we designed estimates and stratifies risk of death during hospitalization for patients with ST-segment elevation myocardial infarction and has good metric properties for predictive ability and calibration.
KEYWORDS ST-segment elevation myocardial infarction, mortality, risk assessment, Cuba
INTRODUCTION Mortality analysis based on a single cause of death is not, in most cases, fully informative. There are several more illuminating procedures using a multiple cause of death approach; these are little known and rarely used in Cuba. The simplest of these methods, while methodologically limited, consists of summing all deaths from a specific cause mentioned on death certificates, regardless of whether the cause is listed as underlying or contributing.
OBJECTIVE Using Cuban data, critically assess and implement two of the most recognized approaches to analyzing multiple causes of death.
METHODS Multiple causes of death in Cuba were assessed for the years 2005, 2010 and 2015, employing death records from the National Medical Records and Health Statistics Bureau of Cuba’s Ministry of Public Health. With the example of diabetes mellitus as underlying cause, we explored connections between underlying and associated (antecedent and contributing) causes on death certificates using two approaches from the international literature: the simple method and the cause-of-death association indicator.
RESULTS The study identified main trends in multiple causes of death identified in 2005, 2010 and 2015, overall and by age group and sex. We observed a trend to increasing mean number of causes of death per death certificate between 2005 and 2015. The number of causes reported showed no substantial differences by age group or sex. Diseases of the arteries, arterioles and capillaries were by far the most frequently associated with diabetes mellitus as underlying cause.
CONCLUSIONS The multiple causes of death approach affords more nuanced understanding of patterns of disease, comorbidity and death in the Cuban population. The indicators used fulfill different roles: the simple method brings to light the full range of ways in which a given cause contributes to mortality, and the cause-of-death association indicator enables exploration of links between different causes of death, not possible with the simple method.
KEYWORDS Mortality, multifactorial causality, causes of death, diabetes mellitus, Cuba
INTRODUCTION Early assessment of prognosis following major abdominal surgery is associated with decreased risk of complications and death. While scoring systems are useful in this regard, there is no index that enables comprehensive individual patient assessment and is also applicable in ICUs with limited resources.
OBJECTIVES Demonstrate that a model based on intra-abdominal pressure is effective in predicting death after major abdominal surgery.
METHODS A prospective observational study was done of 300 post–abdominal-surgery patients admitted to the ICU of a university hospital affiliated with the General Calixto García Medical Faculty, in January 2008 through January 2010. Patients were randomly assigned (2:1) to two groups: test and validation. The independent variable was vital status at discharge (alive or deceased); independent variables were age, sex, malignancy, APACHE II score and intra-abdominal pressure. In the test group, three mathematical models were fit to predict death (APACHE II, intra-abdominal pressure, and APACHE II plus intra-abdominal pressure), which were later validated in the second group. Each model’s capacity to discriminate between living and deceased was evaluated according to sensitivity and specificity of receiver operating characteristic curves. Calibration was assessed with the Hosmer–Lemeshow goodness-of-fit test and comparison of receiver operating characteristic curves by chi-square test of homogeneity. Each patient was followed until hospital discharge or death.
RESULTS The three mortality prediction models displayed excellent calibration and discrimination, very similar predictive power, and no differences among their respective areas under the curve (chi square 2.802, p = 0.094). Variables with the most influence on probability of death were age, APACHE II score and intra-abdominal pressure.
CONCLUSIONS The three models show good capacity and similar effectiveness to predict death after major abdominal surgery. The model based on intra-abdominal pressure is the most feasible in limited-resource settings.
KEYWORDS Abdominal surgery, APACHE II, intra-abdominal pressure, mortality, prediction model, evidence-based medicine, decision modeling, decision support techniques, Cuba
INTRODUCTION Newborns in need of surgery are a challenge to manage and require highly specialized centers with multidisciplinary surgical teams. Since the 1980s, neonatal surgical survival has increased by up to 70% in some countries, mainly due to advances in neonatal intensive care, anesthesia and surgical technique.
OBJECTIVE Describe surgical case fatality and survival in a neonatal reference hospital in Cuba, estimate risk of death, and identify potential risk predictors among neonatal characteristics.
METHODS A retrospective cohort study was conducted based on hospital administrative data and clinical records for a series of surgical cases in the neonatal intensive care unit of Havana’s William Soler University Children’s Hospital from January 2005 to December 2015. All neonates who underwent surgery during the study period were included. The dependent variable was discharge status (alive, deceased); independent variables were: sex, age (in days) at time of surgery, gestational age, birth weight, indication for surgery, surgical order (first, repeat), and presence of sepsis or other postoperative complications. The study used contingency tables to analyze associations between neonatal characteristics and discharge status. A classification tree was used to obtain simple estimates of surgical risk.
RESULTS Survival was 91.3% (675/739) among 739 neonates who underwent surgery. The majority were male (58.7%, 434/739), full term (84.2%, 622/739), and of normal birth weight (80.6%, 596/739). Most surgeries were performed in the first 10 days of life. Digestive system anomalies constituted the most common surgical indication (57.6%, 426/739); among these anorectal malformations (26.8%, 114/426) and esophageal atresia (17.4%, 74/426) predominated. Survival rates were lower for digestive perforation (57.7%, 15/26), gastroschisis (57.1%, 4/7) and intestinal atresia (73%, 27/37). Neonates in the youngest and oldest age groups at time of surgery faced highest risk of death, especially those in the older group. Term infants with normal birth weight operated on for the first time had survival rates >95%.
CONCLUSIONS Survival was high and low birth weight conferred the worst prognosis. Infants with normal birth weight operated on for the first time had the greatest probability of survival.
KEYWORDS Neonatal surgery, intensive care, neonatal; congenital disorders, birth defects, congenital abnormalities, surgery, surgery, mortality, case fatality, Cuba
INTRODUCTION Tuberculosis is the second leading cause of infectious-disease death worldwide, after AIDS. Most tuberculosis patients in Cuba have pulmonary TB and recovery rates are high. When TB chemotherapy fails, the most common adverse outcome is death.
OBJECTIVE Determine survival patterns in a cohort of pulmonary TB patients in Cuba.
METHODS A retrospective cohort study was conducted of pulmonary TB patients who were notified and treated in Cuba in 2009 and 2010. Time elapsed between diagnosis and death was examined. Patient survival was analyzed with the Kaplan–Meier method and comparisons were made with the log-rank estimator; an adjusted Cox model was used to analyze risk of death.
RESULTS The study included 1339 patients, of whom 71.7% were aged 25–64 years and 77.4% were men. Infectious pulmonary tuberculosis was the most common form (75.6%). Only a small number of patients (5.7%) presented TB/HIV coinfection. Ninety-four deaths were reported, 55% during the first 60 days of treatment. Lower survival rates were observed among men (HR 1.87, 95% CI 1.02–3.45), patients coinfected with HIV/AIDS (HR 6.25, 95% CI 3.46–11.31), and patients aged ≥48 years (HR 3.93, 95% CI 2.41–6.40).
CONCLUSION The preponderance of deaths early in TB treatment course may be related to diagnostic and/or treatment delays. Older age at diagnosis, male sex and TB/HIV coinfection increase risk of death.
KEYWORDS Pulmonary tuberculosis, HIV/AIDS, mortality, survival, case fatality, Cuba
INTRODUCTION Population aging translates into more people with chronic non-communicable diseases, disability, frailty and dependency. The study of frailty—a clinical syndrome associated with an increased risk of falls, disability, hospitalization, institutionalization and death—is important to improve clinical practice and population health indicators. OBJECTIVES In a cohort of older adults in Havana and Matanzas provinces, Cuba, estimate prevalence of frailty and its risk factors; determine incidence of dependency; estimate mortality risk and identify mortality predictors. METHODS A prospective longitudinal study was conducted door to door, from June 2003 through July 2011, in a cohort of 2813 adults aged ≥65 years living in selected municipalities of Havana and Matanzas provinces; mean followup time was 4.1 years. Independent variables included demographics, behavioral risk factors and socioeconomic indicators, chronic non-communicable diseases (hypertension, stroke, dementia, depression, diabetes, anemia), number of comorbidities, and APOE ε4 genotype. Dependent variables were frailty, dependency and mortality. Criteria for frailty were slow walking speed, exhaustion, weight loss, low physical activity and cognitive decline. Prevalence and frailty risk were estimated by Poisson regression, while dependency and mortality risks and their predictors were determined using Cox regression. RESULTS Frailty syndrome prevalence was 21.6% (CI 17.9%–23.8%) at baseline; it was positively associated with advanced age, anemia and presence of comorbidities (stroke, dementia, depression, three or more physically debilitating diseases). Male sex, higher educational level, married or partnered status, and more household amenities were inversely associated with frailty prevalence. In followup, dependency incidence was 33.1 per 1000 person-years (CI 29.1–37.6) and mortality was 55.1 per 1000 person-years. Advanced age, male sex, lower occupational status during productive years, dependency, frailty, dementia, depression, cerebrovascular disease and diabetes were all associated with higher risk of death. CONCLUSIONS Given the challenge for developing countries presented by demographic and epidemiologic transition; the high prevalence in older adults of frailty syndrome, dependency and chronic non-communicable diseases; and the association of all these with higher mortality, attention should be targeted to older adults as a risk group. This should include greater social protection, age-appropriate health services, and modification and control of cardiovascular risk factors.
KEYWORDS Frail elderly, frail older adults, aged, elderly, dependency, mortality, chronic disease, dementia, Alzheimer disease, risk factors, Cuba
The following error has been corrected in all online versions of this article.
Page 24, Introduction, first paragraph, line 2, “600,000 to 2 billion” should read “600 million to 2 billion.”
INTRODUCTION Acute myocardial infarction is one of the leading causes of death in the world. This is also true in Cuba, where no national-level epidemiologic studies of related mortality have been published in recent years.
OBJECTIVE Describe acute myocardial infarction mortality in Cuba from 1999 through 2008.
METHODS A descriptive study was conducted of persons aged ≥25 years with a diagnosis of acute myocardial infarction from 1999 through 2008. Data were obtained from the Ministry of Public Health’s National Statistics Division database for variables: age; sex; site (out of hospital, in hospital or in hospital emergency room) and location (jurisdiction) of death. Proportions, age- and sex-specific rates and age-standardized overall rates per 100,000 population were calculated and compared over time, using the two five-year time frames within the study period.
RESULTS A total of 145,808 persons who had suffered acute myocardial infarction were recorded, 75,512 of whom died, for a case-fatality rate of 51.8% (55.1% in 1999–2003 and 49.7% in 2004–2008). In the first five-year period, mortality was 98.9 per 100,000 population, falling to 81.8 per 100,000 in the second; most affected were people aged ≥75 years and men. Of Cuba’s 14 provinces and special municipality, Havana, Havana City and Camagüey provinces, and the Isle of Youth Special Municipality showed the highest mortality; Holguín, Ciego de Ávila and Granma provinces the lowest.
Out-of-hospital deaths accounted for the greatest proportion of deaths in both five-year periods (54.8% and 59.2% in 1999–2003 and 2004–2008, respectively).
CONCLUSIONS Although risk of death from acute myocardial infarction decreased through the study period, it remains a major health problem in Cuba. A national acute myocardial infarction case registry is needed. Also required is further research to help elucidate possible causes of Cuba’s high acute myocardial infarction mortality: cardiovascular risk studies, studies of out-of-hospital mortality and quality of care assessments for these patients.
KEYWORDS Acute myocardial infarction, ischemic heart disease, cardiovascular diseases, chronic disease, mortality, case-fatality, epidemiology, surveillance, registries, Cuba
Introduction Cancer has been the second cause of death in Cuba since 1958. The National Cancer Registry (NCR) and the National Statistics Division of the Ministry of Public Health provide incidence, mortality and other relevant epidemiological data on the disease, as a basis for analysis and decision-making in public health planning for cancer control.
Objectives Describe trends in incidence and mortality of cancer in Cuba overall and by sex since 1990, and analyze the most current 3-year data for frequent types and risk of developing and dying from cancer, by age group, sex, site, and province.
Methods Cancer incidence and mortality were described using age-adjusted rates based on standard world population for 1990–2003 and 1990–2007, respectively. Crude and age-adjusted rates were calculated for the most common sites (excluding nonmelanoma skin cancer) by sex using the latest 3-year incidence data available (2001–2003) from the National Cancer Registry and mortality data (2005–2007) from the National Statistics Division of the Ministry of Public Health. To compare risk of developing and dying from cancer among Cuban provinces, age-adjusted rates were distributed in quartiles.
Results Cancer incidence and mortality have increased in both sexes since 1990. In 2001–2003, an average of 23,710 new cancer cases were diagnosed annually (excluding nonmelanoma skin cancer), and the average annual risk of developing cancer was 216.5 per 100,000 population for men and 204.0 per 100,000 population for women. Between 2005 and 2007, there were 19,671 average annual deaths from cancer in Cuba. The risk of developing and dying from cancer varies by age group and by geographic location but was highest in Havana City province. The sites with highest incidence and mortality were lung, female breast, prostate, colon, and uterine cervix.
Conclusions Cancer incidence and mortality are increasing in Cuba, and the differences by site, age, sex and geographical distribution analyzed in this article, as well as recommended further research, should serve to inform adoption and implementation of more effective strategies for the Ministry of Public Health’s national Comprehensive Cancer Control Program.
Keywords: Cancer, epidemiology, incidence, mortality, death rate, age distribution, sex distribution, registries, Cuba
Introduction Tuberculosis (TB) is a major cause of illness and death throughout the world. The World Health Organization’s Global Plan to Stop TB 2006-2015 proposes that countries cut TB mortality by half compared to 1990 rates. In Cuba, TB mortality declined steadily throughout the 20th century, particularly after 1960.
Objective Describe TB mortality distribution and trends in Cuba from January 1998 to December 2007 by infection site, sex, age and province, and determine progress towards the WHO’s 2015 target for TB mortality reduction.
Methods A time series ecological study was conducted. Death certificates stating TB as cause of death were obtained from the Ministry of Public Health’s National Statistics Division, and population data by age group, sex, and province were obtained from the National Statistics Bureau. Crude and specific death rate trends and variation were analyzed.
Results TB mortality declined from 0.4 per 100,000 population in 1998 to 0.2 (under half the 1990 rate) in 2007. Clinical forms of the disease, both pulmonary and extrapulmonary, also declined. The highest mortality rates were found in males and in the group aged ≥ 65 years. Rates were also highest in the capital, Havana, with extreme values of 0.73 and 0.39 per 100,000 population at the beginning and end of the period, respectively. Conclusions Deaths from TB declined steadily compared to total deaths and deaths caused by infectious diseases. The Global Plan to Stop TB target was met well ahead of 2015. If this trend continues, TB is likely to become an exceptional cause of death in Cuba.
Keywords Lung diseases, tuberculosis, mortality, communicable diseases, trends, Cuba
Introduction Asthma affects some 300 million people worldwide and causes over 250,000 deaths each year. It is considered a global health problem due to associated high morbidity and mortality rates; disability in inadequately treated patients; years of potential life lost (YPLL); social costs; and impact on the lives of patients, their families and society. Environmental factors, including climatic conditions, are triggers. The 2004 Cuban National Survey on Asthma found a national prevalence of 13% (CI 9.3-16.8).
Objective Describe the relationship between climatic factors andasthma mortality in Cuba from 1989 to 2003.
Methods Data on deaths from asthma in Cuba were obtained frommedical death certificates. Crude and adjusted mortality rates werecalculated using the 1981 Cuban population as the standard population;the two-parameter exponential smoothing method was used fortrend and prediction analyses, with 95% confidence intervals (CI) forestimating mortality rates by age, sex and YPLL. ArcView softwareversion 3.3 was used to obtain, adjust, and represent models of meteorologicalvariables, and a bioclimatic atlas was included.
Results Asthma mortality rates increased in Cuba in the early 90sand then decreased and stabilized in recent years; a rate of 2 per100,000 population was predicted for 2008. For the period understudy, 61% of asthma-related deaths occurred in Cuba’s dry wintermonths (November-April). The meteorological variables related to riskof asthma mortality were: atmospheric pressure (997.7-1024.3 hPa),temperature (21.3-24.3oC), number of rainy days in the dry season(15.5-45.2 days), and cloudiness (2.99-5.51%). The provinces withthe highest risk of asthma mortality were: Havana City, Havana, Ciegode Ávila, and Camagüey.
Conclusions In Cuba, unfavorable weather conditions in some geographicareas can cause the death of asthmatic patients, althoughthese are not the only factors determining asthma mortality. Theasthma mortality rate is not alarmingly high and is expected to remainstable. Nevertheless, preventive measures must be maintained,particularly for women, who suffer excess mortality from the disease.Implementation of prevention strategies that take into considerationthe seasonal nature of asthma mortality is recommended.
Keywords Epidemiology, asthma, mortality, climate, asthma in women, respiratory tract diseases, bronchial diseases
