INTRODUCTION Immunity in cancer patients is modified both by the cancer itself and by oncospecific treatments. Whether a patient’s adaptive immunity is impaired depends on their levels of naive lymphocytes and other cell populations. During the COVID-19 pandemic, cancer patients are at greater risk of progressing to severe forms of the disease and have higher mortality rates than individuals without cancer, particularly while they are receiving cancer-specific therapies. An individual’s protection against infection, their response to vaccines, and even the tests that determine the humoral immune response to SARS-CoV-2, depend on lymphocyte populations, meriting their study.
OBJECTIVE Estimate blood concentrations of lymphocytes involved in the immune response to new pathogens in cancer patients.
METHODS We carried out an analytical study of 218 cancer patients; 124 women and 94 men, 26–93 years of age, who were treated at the National Oncology and Radiobiology Institute in Havana, Cuba, March–June, 2020. Patients were divided into five groups: (1) those with controlled disease who were not undergoing cancer-specific treatment; (2) those undergoing debulking surgery; (3) patients undergoing chemotherapy; (4) patients undergoing radiation therapy and (5) patients currently battling infection. We evaluated the following peripheral blood lymphocyte subpopulations via flow cytometry: B lymphocytes (total, naive, transitional, memory, plasmablasts and plasma cells); T lymphocytes (total, helper, cytotoxic and their respective naive, activated, central memory and effector memory subsets); and total, secretory and cytotoxic natural killer cells and T natural killer cells. We also estimated neutrophil/lymphocyte ratios. Lymphocyte concentrations were associated with controlled disease and standard cancer therapy. For variables that did not fall within a normal distribution, ranges were set by medians and 2.5–97.5 percentiles. The two-tailed Mann–Whitney U test was used to measure the effect of sex and to compare lymphocyte subsets. We calculated odds ratios to estimate lymphopenia risk.
RESULTS All cancer patients had lower values of naive helper and cytotoxic T lymphocyte populations, naive B lymphocytes, and natural killer cells than normal reference medians. Naive helper T cells were the most affected subpopulation. Memory B cells, plasmablasts, plasma cells, activated T helper cells, and cytotoxic central memory T cells were increased. Patients undergoing treatment had lower levels of naive lymphocytes than untreated patients, particularly during radiation therapy. The risk of B lymphopenia was higher in patients in treatment. The odds ratio for B lymphopenia was 8.0 in patients who underwent surgery, 12.9 in those undergoing chemotherapy, and 13.9 in patients in radiotherapy.
CONCLUSIONS Cancer and conventional cancer therapies significantly affect peripheral blood B lymphocyte levels, particularly transitional T helper lymphocytes, reducing the immune system’s ability to trigger primary immune responses against new antigens.
KEYWORDS Cancer, lymphocyte subsets, flow cytometry, immunity, virus diseases, Cuba
ABSTRACT INTRODUCTION Immunity in cancer patients is modified both by the cancer itself and by oncospecific treatments. Whether a patient’s adaptive immunity is impaired depends on their levels of naive lymphocytes and other cell populations. During the COVID-19 pandemic, cancer patients are at greater risk of progressing to severe forms of the disease and have higher mortality rates than individuals without cancer, particularly while they are receiving cancer-specific therapies. An individual’s protection against infection, their response to vaccines, and even the tests that determine the humoral immune response to SARS-CoV-2, depend on lymphocyte populations, meriting their study.
OBJECTIVE Estimate blood concentrations of lymphocytes involved in the immune response to new pathogens in cancer patients.
METHODS We carried out an analytical study of 218 cancer patients; 124 women and 94 men, 26–93 years of age, who were treated at the National Oncology and Radiobiology Institute in Havana, Cuba, March–June, 2020. Patients were divided into five groups: (1) those with controlled disease who were not undergoing cancer-specific treatment; (2) those undergoing debulking surgery; (3) patients undergoing chemotherapy; (4) patients undergoing radiation therapy and (5) patients currently battling infection. We evaluated the following peripheral blood lymphocyte subsets via flow cytometry: B lymphocytes (total, naive, transitional, memory, plasmablasts and plasma cells); T lymphocytes (total, helper, cytotoxic and their respective naive, activated, central memory and effector memory subsets); and total, secretory and cytotoxic natural killer cells and T natural killer cells. We also estimated neutrophil/lymphocyte ratios. Lymphocyte concentrations were associated with controlled disease and standard cancer therapy. For variables that did not fall within a normal distribution, ranges were set by medians and 2.5–97.5 percentiles. The two-tailed Mann–Whitney U test was used to measure the effect of sex and to compare lymphocyte populations. We calculated odds ratios to estimate lymphopenia risk.
RESULTS All cancer patients had lower values of naive helper and cytotoxic T lymphocyte populations, naive B lymphocytes, and natural killer cells than normal reference medians. Naive helper T cells were the most affected subpopulation. Memory B cells, plasmablasts, plasma cells, activated T helper cells, and cytotoxic central memory T cells were increased. Patients undergoing treatment had lower levels of naive lymphocytes than untreated patients, particularly during radiation therapy. The risk of B lymphopenia was higher in patients in treatment. The odds ratio for B lymphopenia was 8.0 in patients who underwent surgery, 12.9 in those undergoing chemotherapy, and 13.9 in patients in radiotherapy.
CONCLUSIONS Cancer and conventional cancer therapies significantly affect peripheral blood B lymphocyte levels, particularly transitional T helper lymphocytes, reducing the immune system’s ability to trigger primary immune responses against new antigens.
KEYWORDS Cancer, lymphocyte subsets, flow cytometry, immunity, virus diseases, Cuba
INTRODUCTION In cancer patients, infections are a risk factor for morbidity and mortality, since these tend to be more severe due to secondary immunodeficiency that can develop during the course of the disease and its treatment. The adjusted death rate for infections in individuals with cancer may be three times higher than the general population.[1,2] Patients with hematologic malignancies are at increased risk of infection, compared with patients who have solid tumors, especially when undergoing hematopoietic cell transplantation.[2] Neutropenia, lymphopenia, alterations of anatomical barrier systems (rupture of epithelial surfaces and basement membranes, either due to tumor invasion or induced by therapies), splenic and humoral defects and therapeutic immunosuppression all play a role in immunopathogenesis and affect infection incidence and severity.[3]
IMPORTANCE Knowing lymphoid cell concentrations in cancer patients allows us to design better vaccination strategies for new pathogens like SARS-CoV-2 and avoid false negatives in antibody tests.
Cancer patients have shown greater susceptibility to COVID-19.[4,5] Those with active malignancy experience more severe disease, with COVID-19 mortality rates at 5%–61%, and mean estimated mortality at 25.6%.[2] Risk of dying from COVID-19 is increased (OR = 9.31) when patients have metastatic disease.[6] Compared to persons without cancer, these patients have a higher probability of SARS-CoV-2 infection, of severe manifestations of the disease and of fatal outcomes. These effects are mediated by tumor location, disease stage and treatment type.[3,5,7] Of all these factors, only treatment type can be modified.
The immune response (IR) to infection is complex and requires a functioning immune system (IS) to achieve effective antimicrobial response. Viral infections require special attention, since antiviral treatments are not as effective for them as antibiotics are for bacterial infections.[8,9] Viral infection control depends largely on balancing the innate and adaptive IS, which influence infection and recovery.[8]
The main cells in innate immunity for viral infection control are natural killer (NK) cells, plasmacytoid dendritic cells and neutrophils, which act immediately through extracellular traps.[10,11]
Specific adaptive immunity requires more time to develop than innate immunity, especially in the case of new pathogens like SARS-CoV-2, requiring establishment of a new primary IR. The mature cells involved in adaptive immunity are: helper T lymphocytes (Th), cytotoxic T lymphocytes (Tc) and B lymphocytes, in their varying stages of differentiation (naive, activated, memory, effector and terminally differentiated cell forms). B lymphocytes differentiate into plasma cells that produce antibodies or specific immunoglobulins.[12] Naive lymphocytes are mature T or B cells that reside in peripheral lymphatic organs and in circulating blood, which have never encountered their cognate antigen and are therefore charged with recognizing new pathogens. Their concentration in blood can be measured, as they recirculate in their role in immunosurveillance against new antigens.
IS alterations in cancer patients create challenges in diagnosing and treating emerging infections, as has been the case for COVID-19.[13] Quantitative and qualitative alterations have been noted in both innate and adaptive IS cells in these patients, thus considering cancer a secondary immunodeficiency. Naive T and B lymphocyte populations may be affected, which would compromise the primary immune response of Tc lymphocytes and immunoglobulin production in response to new pathogens such as SARS-CoV-2.[14–16] Patients with malignant hemopathies treated with stem cell therapy require special attention, due to the time required for IS reconstitution and the quality of IR after stem cell transplantation.[17]
Infection as a comorbidity in cancer patients is well-documented,[2,5,18] but few studies have investigated patient susceptibility to infection during epidemics based on alterations to immunopathogenic mechanisms. Changes to IS cells in cancer patients limit the use of treatment and screening strategies designed for the general population. Two of these limitations are of major concern: 1) serological screening tests for diagnosing infections that, due to their high sensitivity and feasibility of application, can result in false negatives due to the decreased function of B lymphocytes, resulting in fewer circulating antibodies produced in response to infection[15,16] and 2) prophylactic vaccination schedules that are not always as effective as in healthy people, due to IS alterations. This could necessitate modifications to the number and interval of vaccine doses, as well as deferring their application, in accordance with cancer stage and type.[19,20] Cancer patients are excluded from clinical trials testing new vaccines, but arguments can be made for their inclusion, because of their increased vulnerability to infection.[21]
Knowing the effect of standard cancer-specific treatments on IS cell proportions in cancer patients could help in designing strategies for controlling epidemics such as COVID-19, including vaccination schedules and detection strategies—and help adjust them to the needs of cancer patients. We carried out this study to evaluate the composition of lymphocytes in blood necessary to trigger a primary immune response against new antigens in Cuban cancer patients.
METHODS Design, participants and sampling We conducted a cross-sectional analytical study in 218 cancer patients with various tumor stages and locations, from March through June 2020. We included 124 women and 94 men 26–93 years of age who were treated in the National Oncology and Radiobiology Institute (INOR) in Havana, Cuba. Patients with malignant hemopathies were not included.
Patients were divided into five groups:
Patients with controlled cancer without oncospecific treatment (n = 39): followup patients with no evidence of active disease were considered ‘controlled’ after at least 12 weeks since the end of their primary/adjuvant treatment. Breast cancer patients who fulfilled this criteria and were on hormonal adjuvant therapy for 5 years or prophylactic treatment with zoledronic acid were also included.
Patients who had not started chemotherapy or radiotherapy, and underwent cytoreductive surgery as a therapeutic standard, 1–7 days post-surgery (n = 54).
Patients undergoing chemotherapy, regardless of the cycle and type of chemotherapy used, who did not undergo surgery or radiotherapy (n = 67).
Patients undergoing radiotherapy who had not received prior or concomitant chemotherapy or surgery (n = 44).
Patients diagnosed with acute infections confirmed via testing (related or unrelated to oncospecific therapies) (n = 14).
Peripheral blood samples were obtained by antecubital venipuncture, 4 mL of which were deposited in Vacutainer tubes (Becton Dickinson, USA) with ethylene aminotetraacetic acid added as an anticoagulant. Samples were processed within the first six hours after extraction.
Flow cytometry We designed a cytometry panel that allowed immunophenotyping of the following lymphocyte subsets (or subpopulations) in peripheral blood based on a CD45+++/SSlow window: Total B lymphocytes (CD19 + / CD20 +), naive (CD19 + / CD20 + / CD38 +/−), early activation (CD19 + / CD20 + / CD22 + / CD25 + / HLA-DR +), late activation (CD19 + / CD20 + / CD25 + / CD22 ++ / HLA-DR ++), transitional (CD19 + / CD20 + / CD22 +/− / CD38 ++), memory (CD19 + / CD20 + CD22 + / CD38 +/−); plasmablasts and plasma cells (CD19 + / CD20 − / CD22 − / CD38 +++); Total T (CD3 +), T helper (Th; CD3 + / CD4 +) and T-cytotoxic (Tc; CD3 + / CD8 +) lymphocytes; Th naive cells, activated, with central memory and effector memory; Naive Tc (CCR7 + / CD45RO −), activated (CD25 + / HLA-DR +), central memory (CCR7 + / CD45RO +) and effector memory (CCR7 − / CD45RO +); Total natural killer cells (NK; CD3 − / CD56 +) (secretory CD56 ++ and cytotoxic CD56 +); Natural killer T cells (NKT; CD3 + / CD56 +). We also estimated the neutrophil/lymphocyte ratio (NLR).
Samples were prepared according to manufacturer specifications for cell surface immunophenotyping, with an unwashed reed blood cell (RBC) lysis protocol (VeraLyse; Beckman-Coulter RBC Lysis Buffer, France). We used a 10-color cytometer (Beckman-Coulter, France). 100 μL of blood was dispensed for staining with fluorochrome-conjugated monoclonal antibodies (Beckman-Coulter, France): anti-CD45 AA750 (Clone J33), anti-CD19 PC7 (Clone J3-119), anti-CD3 FITC (Clone UCHT1), anti-CD4 PB (Clone 13B8.2), anti-CD8 AA700 (Clone B9.11), anti-CD56 PE (Clone N901) (NKH-1), anti-HLA-DR PE (Clone Immu-357), anti-CD45RO PC5 (Clone UCHL1), anti-CCR7 PC7 (Clone G043H7), anti-CD20 FITC (Clone B9E9), anti-CD38 PE (Clone LS198-4-3), anti-CD25 PC5 (Clone B1.49.9) and anti-CD22 PC7 (Clone SJ10.1H11).
We performed daily quality controls of the Flow-Check fluorosphere cytometer, aligning the lasers and checking the water system. Fluorescence intensity was monitored with Flow-Set fluorospheres from the same company.
Data was processed with Kaluza Analysis V1.5a software (Beckman-Coulter, France), with a minimum of 50,000 events acquired. We used a manual and logical-sequential window, and the guidelines recommended by the Human Immunology Project’s immunophenotype standardization.[22] We used published reference values.[23–25]
Statistical analysis To define value ranges, we evaluated normal distribution of variables via the Shapiro-Wilk test. Most variables did not follow a Gaussian distribution. Ranges were set through medians and 2.5–97.5 percentiles. We analyzed the effect of age on lymphocyte populations with a simple linear regression model, and applied the two-tailed Mann-Whitney U test to evaluate the effect of sex as well as the comparison between lymphocyte subpopulations. To evaluate association between variables, we calculated odds ratios. All tests were performed with an associated significance level of p <0.05.
Ethics The study was approved by the INOR ethics committee. Participants provided written informed consent and we followed the principles for human subject research established by the Declaration of Helsinki.[26] Identifying information was kept confidential. Diagnostic means were selected under the guiding principle of maximum beneficence, the ethical norm of ‘do no harm’, and material accessibility.
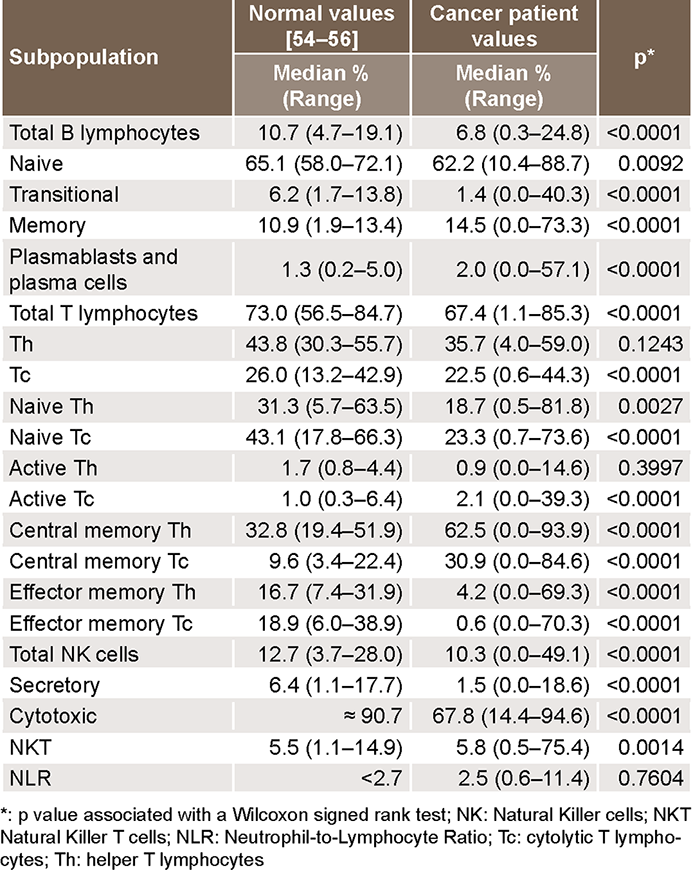
Table 1: Lymphocyte subpopulation percentage values and Neutrophil-to-Lymphocyte Ratios in cancer patient’s peripheral blood, as compared with normal reference values (N = 218)
RESULTS Age and sex did not significantly influence patient lymphocyte ratios.
Most naive T and B lymphocyte and NK cell populations were significantly lower in cancer patients than the normal reference median. However, memory lymphocytes and activated Tc were elevated. The neutrophil-to-lymphocyte ratio (NLR) was within normal range (Table 1).
Significant differences were observed in the estimated medians for all lymphocyte populations’ relative concentrations in the five groups (Table 2). We found a wide range inside the 2.5–97.5 percentiles for all lymphocyte subpopulations in the different groups, most notably in patients with untreated controlled disease and B lymphocyte subpopulations.
Patients with controlled disease had low total values of T lymphocytes and effector memory T lymphocytes (Th and Tc), but their naive T and B cells were not affected. Cytotoxic-type NK cells were lower than reference values.
Activated T lymphocytes, central memory, effector memory (Th and Tc) and transitional B lymphocytes were lower in patients who underwent cytoreductive surgeries. Cytotoxic-type NK cells were significantly lower. Neutrophil values were higher in patients with infection, with a mean of 10,025 cells/μL, increasing the NLR. However, neutrophil values were normal in other groups and the NLR did not rise (Table 2).
Patients undergoing chemotherapy had lower levels of naive Th and Tc cells, total and transitional B lymphocytes, and cytotoxic NK cells.
Patients with infections had lower levels of total T lymphocytes—at the expense of naive Tc—of total and naive B lymphocytes, and of cytotoxic-type NK cells. The NLR was higher, with increased neutrophils.
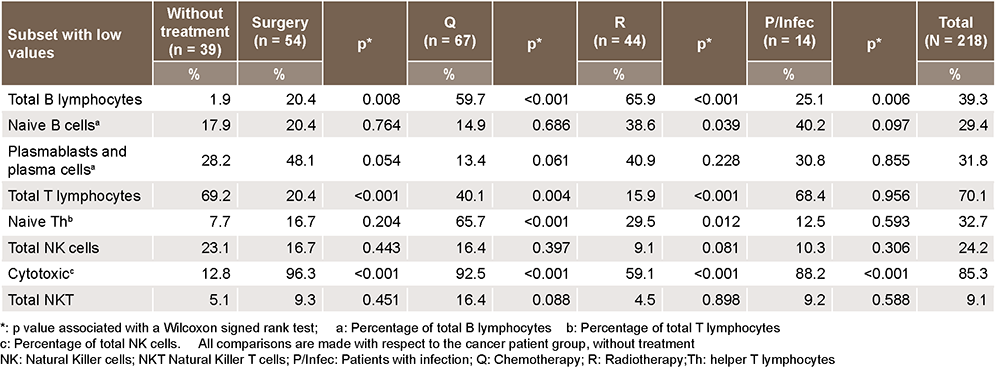
In the standard treatment and infection groups, proportions of patients with low total B lymphocyte values were higher than those in the untreated group (Table 3). Only the radiotherapy group showed a significant increase in patients with low levels of naive B lymphocytes compared to the untreated group. The proportion of patients with low naive Th and cytotoxic NK values was significantly higher in the treated and infection groups. In the treated groups, the proportion of patients with low levels of total T lymphocytes was lower compared to untreated patients (Table 3).
Table 2: Percentage values medians of lymphocyte subsets in cancer patients, by study group
Table 3: Proportion of patients with low lymphocyte subset levels, by study group
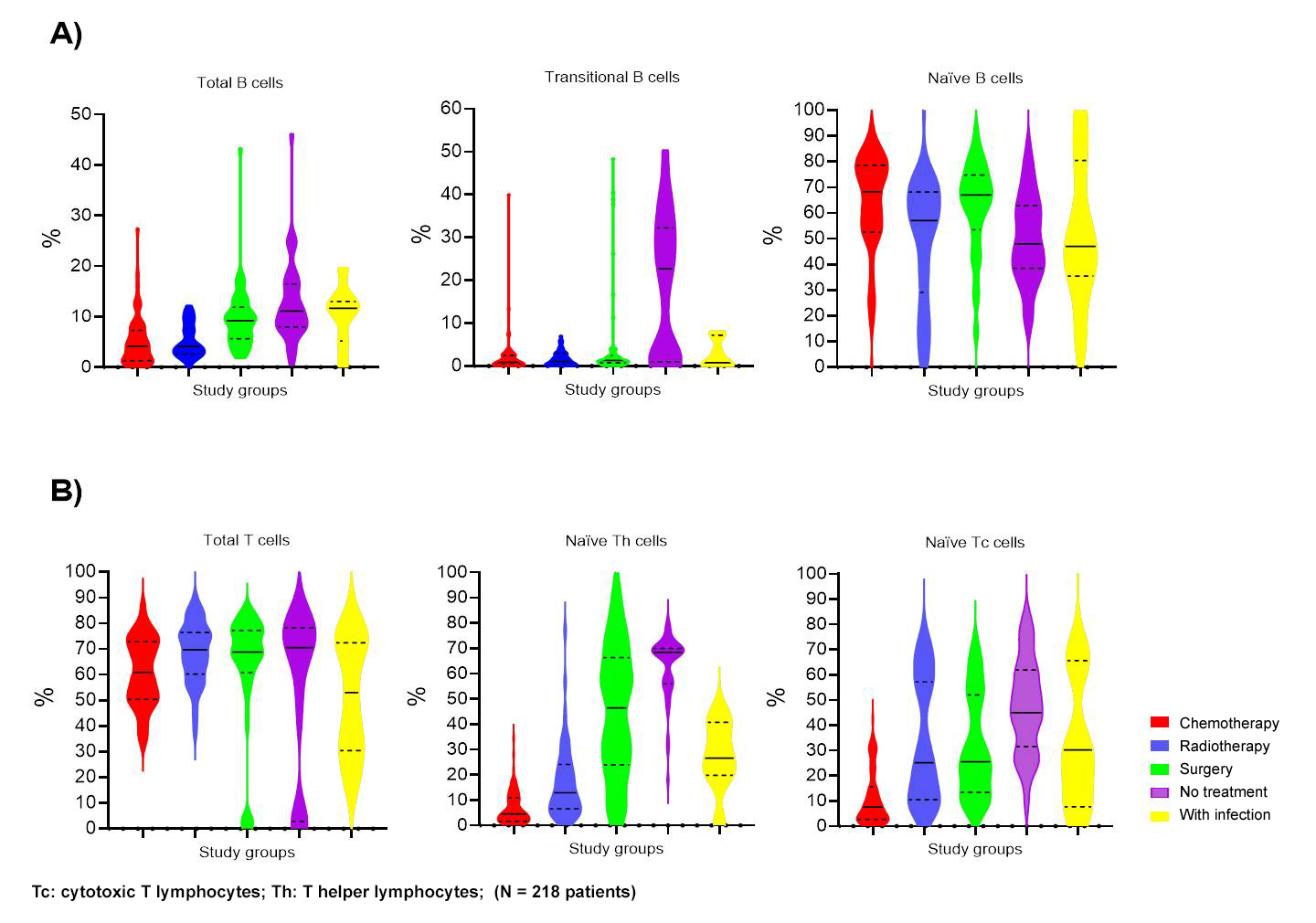
In all treatment groups, transitional B lymphocytes were low, but were high in patients with infections and in untreated patients (variability was high in the latter group). In all groups, naive B lymphocyte medians were normal but significantly lower in patients who had not undergone treatment and in patients with infections compared to treated patients (p = 0.001, Mann-Whitney U) (Figure 1A).
Figure 1: Main lymphocyte subpopulations involved in primary immune responses. A) Distribution of main B lymphocyte subpopulations according to the five study groups of cancer patients. B) Distribution of main T lymphocyte subpopulations according to the five study groups of cancer patients
Patients with infections had the lowest total lymphocyte medians and heterogenous values with bimodal distributions around the first and third quartiles. More than half of chemotherapy patients had decreased naive Th lymphocytes, and those who had undergone surgery had a high dispersion of percentage values for these lymphocytes with a bimodal distribution similar to that described for total T lymphocytes. Naive Th lymphocytes were higher than established reference values in the untreated group. Patients in chemotherapy had low Tc lymphocyte values.
Cancer patients undergoing surgery had an eight-fold higher risk of low transitional B lymphocytes than those who did not receive oncospecific treatments. Cancer patients who underwent surgery had a lower risk for low concentrations of memory B lymphocytes, Th and Tc, with risk reductions of 7.8, 5.5 and 8.3 times, respectively (Table 4).
Chemotherapy patients had a 12.9-fold greater risk than untreated patients for total B-cell lymphopenia and were 32.5 times more likely to have decreased naive Th lymphocyte levels. Risk of transitional B-cell lymphopenia was 2.5 times higher in chemotherapy patients. However, chemotherapy was associated with protection against total and memory T lymphocyte depletion. The risk of lymphopenia was reduced 3.8 times for Th, 9.1 times for Tc, and 33.3 and 11.1 times for central memory Tc and effector memory Th lymphocytes, respectively.
Radiation therapy was associated with a 13.9-fold increased risk of total B-cell lymphopenia. Additionally, it was associated with 10.1- and 7.5-times higher risks of transitional B-cell lymphopenias and naive Th lymphopenias respectively (Table 4), but was a protective factor against central memory and effector memory Th and Tc lymphocyte lymphopenias.
Table 4: Estimates and 95% confidence intervals of odds ratios for the subpopulation presence, by lymphocyte population and cancer therapy type
DISCUSSION Cancer patients suffer from IS dysfunction due to a failure in immune surveillance of malignant tumors. As the disease progresses, IS deficiency worsens, which explains immune tolerance of increasing tumor burdens. For this reason, cancer is considered a cause of secondary immunodeficiency.[27] When standard therapies are applied—chemotherapy,[28,29] radiotherapy[30] and cytoreductive surgery[31,32]—either alone or in combination, they lead to major immunodeficiency.[29] Chemo- and radiotherapy, which mainly affect proliferating cells, can destroy IS cells, especially those of developing leucocyte populations.[27,33] The selective cytotoxic effect on these cells could influence the fact that no significant decreases were found between men and women, or were associated with age.
In the case of lymphocytes, naive subpopulations require cycles of proliferation and differentiation to give rise to effector and memory cells, and are thus more affected than memory cells by chemotherapy and radiation.[3] Memory cells are mostly quiescent and are more abundant, as they have already undergone clonal expansion.[27,34] In our study, the decrease in naive lymphocytes was related to the effects of cancer and cancer-related therapies. These cells were affected by a double depletion mechanism, that of their precursors during maturation and that of naive clones when they are activated by cognate antigen recognition, as they undergo proliferation cycles in both conditions. This is why cancer patients have compromised defenses against infectious agents that are coming into contact with the body for the first time.[6,29,34]
The increase in memory B and T lymphocytes could be relative since their naive counterparts decreased in percentage. Memory Tc cells may increase, mainly in cancers that involve regional lymph nodes depending on disease stage, such as in breast cancer.[35,36] In these cases, tumor antigens arriving from IRs are systematically introduced to secondary lymphoid structures that generate memory clones that circulate in blood.
There is evidence that increases in memory B lymphocytes and Th lymphocytes are interrelated in some cancers, especially when there is a high density of B cells in tertiary lymphoid structures developed in the microenvironment. Increase of these populations is due mainly to clonal expansion, stemming from a great diversity of specificities, particularly in patients younger than 68 years.[37] Montfort concludes that the increase in memory B lymphocytes and antibody-producing plasma cells is due to antigenic diversity generated by the tumor, favored by chemotherapy.[38]
The risk cancer patients will suffer IR alterations is increased when they undergo oncospecific therapies, manifested by a decrease in leukocytes and an increased risk of infection. Our finding of a normal NLR median for all cancer patients was related to a decrease in neutrophils, which could be due to the influence of cytotoxic therapies, as they have a rapid turnover in circulation, with continuous replacement of new cells produced in bone marrow.[39] However, patients with infections had neutrophilia with high indices, contributing to the wide range we observed—up to 11.4.
NLR is an important biomarker for prognosis of these patients, since its increase is associated with poor outcomes.[40] This correlates with the literature, since patients undergoing treatment with chemo- and radiotherapy generally have lymphopenia and a low NLR, sometimes requiring treatment with granulocyte colony stimulating factor. In patients with infections, this index increased, which suggests poorer prognoses. In patients that recover, cell restoration kinetics are different for leukocytes and lymphocytes, as lymphocytes require more time to recover. Adaptive immunity takes anywhere from six months to a year to restore itself following chemotherapy. This delay can negatively impact patient prognosis after completion of cytotoxic therapies, as neutrophils normalize much faster than lymphocytes and thus NLR rises at the expense of persistent lymphopenia.[30,41]
Other research evaluating the impact of cancer and its treatments on IS cell ratios is based on lineage analysis, but few studies examine distribution of naive or memory populations. Our study shows that the cell population most affected by cancer treatment is B lymphocytes, which helps explain why the humoral response is also affected. This coincides with publications by other authors;[31,42–44] however, the main lymphocyte subpopulations involved in primary IR were also decreased in some study groups.
Recent research indicates that in chemotherapy patients, not only are naive cells lost, but memory cells (both B and T) are also diminished, manifested by a decrease of antibody titers against previously administered vaccines. This has been the case in antigen-dependent responses.[41,43] However, protection is preserved against latent viruses like cytomegalovirus, suggesting memory cytotoxic T cell preservation. This could be due to the fact that memory cells are mostly quiescent, and this type of therapy acts especially well on proliferating cells.[33,44] We observed the opposite in the defense against new infections produced by viruses like Zika, SARS-CoV-2 or West Nile, in which the naive cell repertoire is compromised and they are the ones generating the primary immune response.[30,43]
Our results coincide with these findings, as there was a significant decrease in naive populations, which resulted in a compromised primary response. In the case of total T lymphocytes, no risk of ymphopenia was found in the chemotherapy group, possibly due to the relative estimation of their subpopulations, and the decrease in naive cells did not cause a percentage decrease in T cells. These results are especially important during the COVID-19 pandemic, when cancer patients are more susceptible to severe forms of the disease and death.[2,5]
The tissues most affected by radiation are bone marrow and intestinal mucosa. Both are essential in the IS, since the first produces naive lymphocytes and the second is one of the largest secondary lymphoid organs. Radiation’s cytotoxic effects increase with dose and treatment time. The main mechanisms of radiation-induced death in lymphocyte populations are primary necrosis for T lymphocytes, secondary necrosis for B lymphocytes, and apoptosis for NK cells. NK lymphocytes are the most radiosensitive immune cells, followed by B lymphocytes and lastly, T cells.[38]
Within T cell and B cell subpopulations, naive cells are the most radiosensitive, because they proliferate when activated. Although radiation therapy is localized, its effects on lymphocytes are systemic.[44] Dovšak showed radiotherapy’s immunosuppressive effects in oral cancer patients and its negative impact on naive cells, even when irradiation was local. NK cells were also affected. This depression can persist longer than a year following treatment cessation.[31]
Transitional B lymphocytes come from bone marrow, are precursors of naive cells, and complete their maturation in other organs. Cells with the CD38hi subphenotype are known to be tolerant to circulating autoantigens, like tumor antigens, and the mechanism behind this tolerance is anergy, which often ends in apoptosis.[45] This could explain the depletion found in this lymphocyte subphenotype. In all groups studied, lymphopenia has multiple repercussions for patients (Figure 1A). On one hand, the repertoire of naive cells derived from transitional cells is reduced and the generation of humoral responses to new antigens is compromised—as is the case for new pathogens like SARS-CoV-2—but on the other hand this could lead to better cancer prognoses, as the cells that produce interleukin-10 are reduced at a systemic level, decreasing antitumor responses.
Cancer patients who underwent surgery had less risk of lower B lymphocyte, Th and total Tc lymphocyte values, which suggests tumor removal modifies inter-department lymphocyte distribution, although it does not necessarily favor production of naive lymphocytes. Cytoreductive cancer surgery improves patient immune status as it eliminates the tumor microenvironment that produces both local and systemic immunosuppressive effects, but it does so by reducing suppressive lymphocytes.[46,47] However, these surgeries are a stressor and they produce a decrease in certain lymphocyte populations, although this decrease is temporary.[47]
The decrease in transitional B lymphocytes after debulking surgeries could be related to inflammatory response and surgical healing processes. After the operation, bone marrow increases production of red blood cells, neutrophils and T lymphocytes related to homeostasis. B lymphocytes are perhaps less necessary to this process and transitional cells belong to the final stage of this lymphocytic lineage’s maturation. Naive Th cells had widely dispersed percentage values and exhibited a bimodal distribution similar to that described for total T lymphocytes. This could be due to heterogenicity in the tumor microenvironment’s cellular composition, which has a systemic impact and depends on tumor type and disease stage.[48]
The prognosis for an unfavorable NLR evolution is greater when dependent on a decrease in lymphocytes. NLR increase denotes dysfunctional and sometimes suppressive inflammation, which translates clinically into reduced patient survival and poor tumor cell response to therapies inhibiting PD1 receptors.[49] It is also associated with poor prognoses in infections with uncontrolled inflammatory reactions like those seen in COVID-19,[50] so this indicator should be measured in cancer patients, especially during oncospecific therapies. Absence of a high NLR in all study participants is because although patients with infections had neutrophilia and increased NLR, patients who received chemo- and radiotherapy had neutropenia and decreased NLR.
Antibody levels against pretreatment infections, including COVID-19, are lowered in cancer patients treated with chemotherapy.[15,16] In hematologic malignancies like leukemia, the antibody response to vaccines is also affected before starting chemotherapy, so the deficit caused by the disease is added to that caused by the therapy, implying that patients should be reimmunized three to six months after finishing treatment.[51–53] Antibody production is affected in cancer patients, so it would be advisable during new epidemics to carry out diagnostic tests that detect the causal agent—rather than estimating antibody presence in response to the causal agent—as this could be decreased or absent and result in false negatives, even if the patient has the infection.
Vaccination strategies in cancer patients should be based on sound scientific evidence, to not deprive them of vaccines or subject them to unnecessary risks. Indication for patient vaccination depends on vaccine design, cancer type, the state of the patient’s immune system, and treatment timing and type. In our experience with cancer patients, protective effects of immunization are obtained one month after immunosuppressive treatment cessation. However, in the case of malignant blood diseases like leukemia, vaccination is not always recommended, as treatments are usually prolonged. Malignant B cell neoplasms such as lymphoma, chronic lymphocyte leukemia and multiple myeloma will likely have different antibody responses to other cancer types in which the cells responsible for producing antibodies in response to infection are not affected by treatment. This is important when deciding whether to administer vaccines, where protection is related to antibody production, so indication for vaccination depends on vaccine design and expected response.
In addressing pandemics like COVID-19, vaccination strategies for cancer patients must be considered since high percentages of the population require vaccination and the decision whether to vaccinate patients or their cohabiting relatives should be prioritized. This decision must take into account cancer type, stage, the type of oncospecific treatment, the possible response of IS cells to these conditions and other preexisting comorbidities, as well as the type of vaccine to be administered.
Considering our results, it is recommended that vaccines—particularly those with attenuated live agents—not be administered during convalescence from major surgeries, in the first cycles of chemotherapy, or during full-dose total body irradiation. The proposal would be to vaccinate with a first dose two weeks before treatment or two weeks after treatment, at minimum, and finish the immunization schedule before starting another treatment cycle.[54,55]
Although this study was aimed at obtaining an overview of cancer as a group of diseases and establishing the effects of modifiable factors like therapeutic standards and infections, a stratified study examining age, sex, cancer type, disease stage and particularities within treatment groups is needed. Non-inclusion of these variables and stratification criteria constitute the main limitations of the present study.
CONCLUSIONS Cancer and its therapeutic standards significantly affect levels of NK cells and B lymphocytes in peripheral blood, particularly transitional B cells, and reduce percentages of naive T helper lymphocytes. The radiotherapy group was the most affected. These alterations reduce the IS’s ability to trigger effective immune responses to new antigenic challenges, including when a patient first encounters a new virus or a new vaccine. Due to IS effects in these patients, management of new infections and epidemics must differ from those established for the general population, including vaccination strategies and diagnostic methods that rely on detecting antibodies against specific pathogens.
Au L, Boos LA, Swerdlow A, Byrne F, Shepherd S, Fendler A, et al. Cancer, COVID-19, and antiviral immunity: The CAPTURE Study. Cell. 2020 Oct 1;183(1):4–10. https://doi.org/10.1016/j.cell.2020.09.005
Zheng Y, Chen Y, Yu K, Yang Y, Wang X, Yang X, et al. Fatal infections among cancer patients: a population based study in the United States. Infect Dis Ther. 2021 Jun;10(2):871–95. https://doi.org/10.1007/s40121-021-00433-7
Bakouny Z, Hawley JE, Choueiri TK, Peters S, Rini BI, Warner JL, et al. COVID-19 and cancer: current challenges and perspectives. Cancer Cell. 2020 Nov 9;38(5):629–46. https://doi.org/10.1016/j.ccell.2020.09.018
Li H, Baldwin E, Zhang X, Kenost C, Luo W, Calhoun EA, et al. Comparison and impact of COVID-19 for patients with cancer: a survival analysis of fatality rate controlling for age, sex and cancer type. BJM Health Care Inform. 2021 May;28(1):e100341. https://doi.org/10.1136/bmjhci-2021-100341
Lee LYW, Cazier JB, Starkey T, Briggs SE, Arnold R, Bisht V, et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study. Lancet Oncol. 2020 Oct;21(10):1309–16. https://doi.org/10.1016/S1470-2045(20)30442-3
Johannesen1 JB, Smeland S, Aaserud S, Buanes EA, Skog A, Ursin G, et al. COVID-19 in cancer patients, risk factors for diseases and adverse outcome, a population-based study from Norway. Front Oncol. 2021 Mar 25;11:652535. https://doi.org/10.3389/fonc.2021.652535
Zong Z, Wei Y, Ren J, Zhang L, Zhou F. The intersection of COVID-19 and cancer: signaling pathways and treatment implications. Mol Cancer. 2021 May 17;20(1):76. https://doi.org/10.1186/s12943-021-01363-1
Zheng H, Rao AM, Dermadi D, Toh T, Jones LM, Donato M, et al. Multi-cohort analysis of host immune response identifies conserved protective and detrimental modules associated with severity across viruses. Immunity. 2021 Apr 13;54(4):753–68. https://doi.org/10.1016/j.immuni.2021.03.002
Conry SJ, Milkovich KA, Yonkers NL, Rodriguez B, Bernstein HB, Asaad R, et al. Impaired plasmacytoid dendritic cell (PDC)-NK cell activity in viremic human immunodeficiency virus infection attributable to impairments in both PDC and NK cell function. J Virol. 2009;83(21):11175–87. https://doi.org/10.1128/JVI.00753-09
Orakpoghenor O, Avazi DO, Markus TP, Olaolu OS. Lymphocytes: a brief review. Sci J Immunol Immunother. 2019 Jun 24;3(1):004–008. https://doi.org/10.37871/sjii.id17
Derosa L, Melenotte C, Griscelli F, Gachot B, Marabelle A, Kroemer G, et al. The immuno-oncological challenge of COVID-19. Nat Cancer. 2020;1(10):946–64. https://doi.org/10.1038/s43018-020-00122-3
Liu T, Zeng G, Tao H, Shi Y; COVID Cancer Patients Research Group, Wang T, et al. Low prevalence of IgG antibodies to SARS-CoV-2 in cancer patients with COVID19. Int J Cancer. 2020 Dec 1;147(11):3267–9. https://doi.org/10.1002./ijc33148
Solodky ML, Galvez C, Russias B, Detourbet P, N’Guyen-Bonin V, Herr AL, et al. Lower detection rates of SARS-COV2 antibodies in cancer patients versus health care workers after symptomatic COVID-19. Ann Oncol. 2020 Aug;31(8):1087–88. https://doi.org/10.1016/j.annonc.2020.04.475
Bejanyan N, Brunstein CG, Cao Q, Lazaryan A, Luo X, Curtsinger J, et al. Delayed immune reconstitution after allogeneic transplantation increases the risks of mortality and chronic GVHD. Blood Adv. 2018 Apr 24;2(8):909–22. https://doi.org/10.1182/bloodadvances.2017014464
Tau N, Shargian-Alon L, Reich S, Paul M, Gaffter A, Shepshelovich D, et al. Reporting infections in clinical trials of patients with haematological malignancies. Clin Microbiol Infect. 2019 Dec;25(12):1494–500. https://doi.org/10.1016/j.cmi.2019.04.029
Keam B, Kim MK, Choi Y, Choi SJ, Choe PG, Lee KH, et al. Optimal timing of influenza vaccination during 3-week cytotoxic chemotherapy cycles. Cancer. 2017 Mar 1;123(5):841–48. https://doi.org/10.1002/cncr.30468
Jamshed S, Walsh EE, Dimitroff LJ, Seguin Santelli J, Falsey AR. Improved immunogenicity of high-dose influenza vaccine compared to standard-dose influenza vaccine in adult oncology patients younger than 65 years receiving chemotherapy: a pilot randomized clinical trial. Vaccine 2016 Jan 27;34(5):630–5. https://doi.org/10.1016/j.vaccine.2015.12.037
Maecker HT, McCoy JP, Nussenblatt R. Standardizing immunophenotyping for the Human Immunology Project. Nat Rev Immunol. 2012 Feb 17;12(3):191–200.
Kokuina E, Breff-Fonseca MC, Villegas-Valverde CA, Mora-Díaz I. Normal values of T, B and NK lymphocytes subpopulations in peripheral blood of healthy Cuban adults. MEDICC Rev. 2019 Apr–Jul;21(2–3):16–21. https://doi.org/10.37757/MR2019.V21.N2-3.5
Bisset LR, Lung TL, Kaelin M, Ludwig E, Dubs RW. Reference values for peripheral blood lymphocyte phenotypes applicable to the healthy adult population in Switzerland. Eur J Haematol. 2004 Mar;72(3):203–12.
Morbach H, Eichhorn EM, Liese JG, Girschick HJ. Reference values for B cell subpopulations from infancy to adulthood. Clin Exp Immunol. 2010 Nov;162(2):271–9. https://doi.org/10.1111/j.1365-2249.2010.04206.x
Litterman AJ, Zellmer DM, Grinnen KL, Hunt MA, Dudek AZ, Salazar AM, et al. Profound impairment of adaptive immune responses by alkylating chemotherapy. J Immunol. 2013 Jun 15;190(12):6259–68. https://doi.org/10.4049/jimmunol.1203539
Verma R, Foster RE, Horgan K, Mounsey K, Nixon H, Smalle N, et al. Lymphocyte depletion and repopulation after chemotherapy for primary breast cancer. Breast Cancer Res. 2016 Jan 26;18(1):10. https://doi.org/10.1186/s13058-015-0669-x
Lv Y, Song M, Tian X, Yv X, Liang N, Zhang J. Impact of radiotherapy on circulating lymphocyte subsets in patients with esophageal cancer. Medicine (Baltimore). 2020 Sep 4;99(36):e20993. https://doi.org/10.1097/MD.0000000000020993
Dovšak T, Ihan A, Didanovič V, Kansky A, Verdenik M, Hren NI. Effect of surgery and radiotherapy on complete blood count, lymphocyte subsets and inflammatory response in patients with advanced oral cancer. BMC Cancer. 2018 Mar 1;18(1):235.https://doi.org/10.1186/s12885-018-4136-9
Das RK, Vernau L, Grupp SA, Barrett DM. Naïve T-cell deficits at diagnosis and after chemotherapy impair cell therapy potential in pediatric cancers. Cancer Discov. 2019 Apr;9(4):492–9. https://doi.org/10.1158/2159-8290.CD-18-1314
Chen X, Lowe M, Herliczek T, Hall MJ, Danes C, Lawrence DA, et al. Protection of normal proliferating cells against chemotherapy by Staurosporine-Mediated, selective, and reversible G1 arrest. J Natl Cancer Inst. 2000 Dec 20;92(24):1999–2008.https://doi.org/10.1093/jnci/92.24.1999
Jia Y, Xu L, Lin Q, Zhu M, Ding L, Wu K, et al. Levels of lymphocyte subsets in peripheral blood prior treatment are associated with aggressive breast cancer phenotypes or subtypes. Med Oncol. 2014 Jun;31(6):981. https://doi.org/10.1007/s12032-014-0981-9
Vahidi Y, Bagheri M, Ghaderi A, Faghih Z. CD8-positive memory T cells in tumor- draining lymph nodes of patients with breast cancer. BMC Cancer. 2020 Mar 20(1);20:257. https://doi.org/10.1186/s12885-020-6714-x
Zhu W, Germain C, Liu Z, Sebastian Y, Devi P, Knockaert S, et al. A high density of tertiary lymphoid structure B cells in lung tumors is associated with increased CD4C T cell receptor repertoire clonality. Oncoimmunology. 2015 Jun 1;4(12):e1051922. https://doi.org/10.1080/2162402X.2015.1051922
Falcke SE, Rühle PF, Deloch L, Fietkau R, Frey B, Gaipl US. Clinically relevant radiation exposure differentially impacts forms of cell death in human cells of the innate and adaptive immune system. Int J Mol Sci. 2018 Nov 13;19(11):3574. https://doi.org/10.3390/ijms19113574
Lahoz-Beneytez J, Elemans M, Zhang Y, Ahmed R, Salam A, Block M, et al. Human neutrophil kinetics: modeling of stable isotope labeling data supports short blood neutrophil half-lives. Blood. 2016 Jun 30;127(26):3431–38. https://doi.org/10.1182/blood-2016-03-700336
Cupp MA, Cariolou M, Tzoulaki I, Aune D, Evangelou E, Berlanga-Taylor AJ. Neutrophil to lymphocyte ratio and cancer prognosis: an umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020 Nov 20;18(1):360. https://doi.org/10.1186/s12916-020-01817-1
Waidhauser J, Schuh A, Trepel M, Schmälter AK, Rank A. Chemotherapy markedly reduces B cells but not T cells and NK cells in patients with cancer. Cancer Immunol Immunother. 2020 Jan;69(1):147–57. https://doi.org/10.1007/s00262-019-02449-y
Gustafson CE, Jadhav R, Cao W, Qi Q, Pegram M, Tian L, et al. Immune cell repertoires in breast cancer patients after adjuvant chemotherapy. JCI Insight. 2020 Feb 27;5(4):e134569. https://doi.org/10.1172/jci.insight.134569
Swanson GP, Jhavar SG, Hammonds K. The effect of pelvic radiation alone on lymphocyte subgroups. Clin Transl Radiation Oncol. 2020 May 30;23:100–2. https://doi.org/10.1016/j.ctro.2020.05.010
Das RK, O’Connor RS, Grupp SA, DM Barrett. Lingering effects of chemotherapy on mature T cells impair proliferation. Blood Adv. 2020 Oct 13;4(19):4653–64. https://doi.org/10.1182/bloodadvances.2020001797
Blair PA, Norena LY, Flores-Borja F, Rawlings DJ, Isenberg DA, Ehrenstein MR, et al. CD19(+)CD24(hi)CD38(hi) B cells exhibit regulatory capacity in healthy individuals but are functionally impaired in systemic lupus erythematosus patients. Immunity. 2010 Jan 29;32(1):129–40. https://doi.org/10.1016/j.immuni.2009.11.009
Napoletano C, Bellati F, Landi R, Pauselli S, Marchetti C, Visconti V, et al. Ovarian cancer cytoreduction induces changes in T cell population subsets reducing immunosuppression. J Cell Mol Med. 2010 Dec;14(12):2748–59. https://doi.org/10.1111/j.1582-4934.2009.00911.x
Jiménez-Sánchez A, Memon D, Pourpe S, Veeraraghavan H, Li Y, Vargas HA, et al. Heterogeneous tumor-immune microenvironments among differentially growing metastases in an ovarian cancer patient. Cell. 2017 Aug 24;170(5):927–38. https://doi.org/10.1016/j.cell.2017.07.025
Tavakkoli M, Wilkins CR, Mones JV, Mauro MJ. A novel paradigm between leukocytosis, G-CSF secretion, neutrophil-to-lymphocyte ratio, myeloid-derived suppressor cells, and prognosis in non-small cell lung cancer. Front Oncol. 2019 Apr 26;9:295. https://doi.org/10.3389/fonc.2019.00295
Zhang B, Zhou X, Zhu C, Song Y, Feng F, Qiu Y, et al. Immune phenotyping based on the Neutrophil-to-Lymphocyte Ratio and IgG level predicts disease severity and outcome for patients with COVID-19. Front Mol Biosci. 2020 Jul 3;7:157. https://doi.org/10.3389/fmolb.2020.00157
Zengin E, Sarper N. Humoral immunity to diphtheria, tetanus, measles, and hemophilus influenza type b in children with acute lymphoblastic leukemia and response to re-vaccination. Pediatr Blood Cancer. 2009 Dec;53(6):967–72. https://doi.org/10.1002/pbc.22135
Top KA, Vaudry W, Morris SK, Pham-Huy A, Pernica JM, Tapiéro B, et al. Waning vaccine immunity and vaccination responses in children treated for acute lymphoblastic leukemia: a Canadian immunization research network study. Clin Infect Dis 2020 Dec 3;71(9):e439–48. https://doi.org/10.1093/cid/ciaa163
Blanchette PS, Chung H, Pritchard KI, Earle CC, Campitelli MA, Buchan SA, et al. Influenza vaccine effectiveness among patients with cancer: a population-based study using health administrative and laboratory testing data from Ontario, Canada. J Clin Oncol. 2019 Oct 20;37(30):2795–804. https://doi.org/10.1200/JCO.19.00354
ESMO [Internet]. Geneva: ESMO; c2021. COVID-19 and Cancer. ESMO statements for vaccination against COVID-19 in patients with cancer; 2020 Dec 22 [updated 2021 Apr 27; cited 2021 Feb 2]. Available at: https://www.esmo.org/covid-19-and-cancer/covid-19-vaccination
Desai A, Gainor JF, Hegde A, Schram AM, Curigliano G, Pal S, et al. COVID-19 vaccine guidance for patients with cancer participating in oncology clinical trials. Nat Rev Clin Oncol. 2021 May;18(5):313–9. https://doi.org/10.1038/s41571-021-00487-z
THE AUTHORS
María del Carmen Arango-Prado, physician specializing in immunology with a doctorate in medical sciences. Full professor, Medical University of Havana, and associate researcher, Immunology Laboratory, National Oncology and Radiobiology Institute (INOR), Havana, Cuba. https://orcid.org/0000-0002-8307-4296
Carlos Agustín Villegas-Valverde, (Corresponding author: carlosvillega@infomed.sld.cu), physician with dual specialties in family medicine and immunology, with master’s degrees in infectious diseases, medical education, and a doctorate in medical science. Associate professor, Medical University of Havana and associate researcher, Immunology Laboratory, INOR, Havana, Cuba. https://orcid.org/0000-0001-7478-0482
Griselda Torres-López, microbiologist, with a master’s degree in microbiology. Immunology Laboratory, INOR, Havana, Cuba. https://orcid.org/0000-0002-6060-1727
Pilar Soto-Pardeiro, physician specializing in immunology with a master’s degree in clinical trials. Immunology Laboratory, INOR, Havana, Cuba. https://orcid.org/0000-0001-5055-064X
Anamary Suárez-Reyes, physician specializing in family medicine and immunology. Instructor, Medical University of Havana, Immunology Laboratory, INOR, Havana, Cuba. https://orcid.org/0000-0003-0289-0230
María Elena Faxas-García, physician specializing in immunology with a doctorate in medical sciences. Full professor, Medical University of Havana and senior researcher, Immunology Laboratory, INOR, Havana, Cuba. https://orcid.org/0000-0001-8853-9198
Elías Gracia-Medina, oncologist. Associate professor, Medical University of Havana and associate researcher, Oncology Service, INOR, Havana, Cuba. https://orcid.org/0000-0002-9389-9291
Roberto Esperón-Noa,general surgeon. Associate professor, Medical University of Havana and associate professor, Oncology Service, INOR, Havana, Cuba. https://orcid.org/0000-0002-7002-0619
Ramón del Castillo-Bahi, oncologist. Assistant professor, Medical University of Havana. Radiotherapy service, INOR, Havana, Cuba. https://orcid.org/0000-0001-6519-1248
Ariadna Méndez-Rosabal, physician specializing in family medicine and internal medicine, with a master’s degree in atherosclerosis. Associate professor, Havana Medical University, Havana, Cuba. https://orcid.org/0000-0003-2906-0958
Luis Curbelo-Alfonso, general surgeon. Assistant professor, Medical University of Havana. Director, INOR, Havana, Cuba. https://orcid.org/0000-0002-6187-2350
Submitted: May 06, 2021 Approved: January 16, 2022 Disclosures: None
Arango-Prado MC, Villegas-Valverde CA, Torres-López G, Soto-Pardeiro P, Suárez-Reyes A, Faxas-García ME, et al. Lymphocyte subsets in defense against new pathogens in patients with cancer. MEDICC Rev. 2022 Apr;24(2):26 – 34. https://doi.org/10.37757/mr2022.v24.n2.5
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.