INTRODUCTION
Mild cognitive impairment and dementia are among the most important public health issues worldwide.[1] Given their association with aging and the trend towards longer life expectancies exhibited globally, these disorders have steadily increased in both crude incidence and prevalence over the past decade.
Dementia is a syndrome characterized by an acquired, progressive and persistent impairment of higher cognitive functions, personality, behavior, and content of consciousness (without changes in level of consciousness). It hinders people’s satisfactory performance of their daily activities, work, and social life, and, ultimately, their independence. Loss of independence is one of the greatest frustrations, not just for these patients but also for their families, and it compromises affective relationships developed over a lifetime. Because of its impact on daily living and interpersonal relations, dementia requires not only a health care response but also a degree of societal commitment.
There is substantial regional variation in dementia prevalence, from 2.1% in West Sub-Saharan Africa to 8.5% in Latin America, with most regions falling between 5% and 7%.[2] Dementia has multiple etiologies, including neurodegenerative diseases; the most prevalent type, Alzheimer disease (AD), accounts for the majority of dementia cases.[2] Its clinical picture (formally described in 1906 by Alois Alzheimer and later named by Emil Kraepelin) was surprisingly neglected for almost 80 years, but is now one of the neuropsychological disorders receiving most attention (in both basic and clinical research) and causing greatest concern on the part of families and health authorities.[3] It was declared a global health priority by WHO in 2012[1] and is considered by many to be the epidemic of our time.
Cuba’s National Program for Older Adults, considered a priority and included in the Public Health Projections in Cuba for 2015,[4] addresses dementia and disabilities. Dementia deaths (mainly AD) have increased in recent years. It was among the ten leading causes of death from 2007 to 2012,[5] becoming the 6th leading cause of death for all ages in 2011, with a rate of 31.4 per 100,000 population. The Alzheimer Section of the Cuban Neurosciences Society and the 10/66 Dementia Research Group have spearheaded recognition and study of dementia as a public health issue, as well as support for dementia patients and their families in Cuba.[6] The 10/66 Group has produced numerous important studies, reporting a prevalence of dementia in Cuba of 6.3% (CI 5.0%–7.7%) in population studies;[7] and in various local studies in clinical settings of 5.4%[8], 10.8%[9] and 27.3%.[10]
Establishing research priorities is critical for funding allocation and coherent health research policies that, in a longterm and constantly evolving interactive process, eventually reduce the gap between what is studied and the scientific evidence needed for patient care and population health improvement.
An effective strategy for studying and controlling diseases is epidemiological surveillance—a dynamic, ongoing and systematic process to collect, analyze, interpret and disseminate descriptive data from different sources for monitoring public health problems. Its general objective is to provide ongoing technical guidance for decisionmakers on prevention and control activities, supplying updated data on disease incidence, determining factors and at-risk populations.[11] While epidemiological health surveillance originally applied only to the observation, tracking and control of infectious diseases, its use has since been expanded to other health problems with important social and public health implications.[12]
Epidemiological surveillance based on appropriately designed centralized registries provides reliable information for decision-making, planning and resource allocation for prevention, as well as for evaluation of the impact of disease-specific prevention/intervention programs.[13] Furthermore, by combining information from different sources, it provides a timely epidemiological picture of the disease’s incidence and prevalence. While registries have long been developed for cancer and heart disease, they are not common in the field of dementia, although some models do exist. Beginning in the 1980s, several initiatives have been undertaken in the USA (e.g., the Consortium to Establish a Registry for Alzheimer’s Disease, CERAD),[13–16] Spain[17] and Argentina,[18] working with centralized data registries of patients with dementia in their respective countries, although registry methods and environments are not comparable.
This article aims to provide an overview of methodologies used in the dementia registries included in the specialized bibliography as a comparative context for a proposed Cuban registry of cognitive impairment and dementia (ReCeDemCu).[19]
CENTRALIZED DEMENTIA REGISTRIES AND EPIDEMIOLOGICAL SURVEILANCE
Various definitions have been put forward for a disease registry.[20] The US Agency for Healthcare Research and Quality (AHRQ) defines a registry as “an organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure and that serves predetermined scientific, clinical or policy purpose(s).”[21]
Although no standard definition for a dementia registry has been established, epidemiological information on dementia is derived mainly from three distinct types, depending on the origin of the subjects examined: 1) population registries, 2) hospital registries, and 3) “case study” registries. Population registries—the most common—are useful from an epidemiologic viewpoint, since they systematically include all cases of dementia occurring in a specific population and provide maximum reliability for epidemiological variables, such as incidence, prevalence, mortality and recurrence rates. Such registries are expensive, however, and their classification of dementia syndrome etiological subtypes is often incomplete; they also commonly overestimate measurement variables by over-rating symptoms.[16,18,22–28] Within this category of population registries there are also community studies, which are constrained by being limited to a specific geographical area and may show selection bias, but are useful for planning local allocation of social and health resources. An example is Spain’s Girona Dementias Registry.[29]
Hospital registries have the advantage of recording more detailed data (clinical, neuroimaging, laboratory), which improves disease classification by etiological subtype, thus providing important information on clinical characteristics and enabling strategies for health resources allocation. However, these registries are most likely limited due to the bias of obtaining information dependent on the social and health characteristics of the catchment area, as well as the resources of their host facility. A further disadvantage of hospital registries is that most dementia patients are not hospitalized, so these registries are biased toward greater severity than is found in the underlying population. In addition, differences in clinical settings and methods make it difficult to compare information among hospital registries.[15,25,30]
Case study registries are useful for analyzing concrete clinical aspects or for recruiting patients for clinical trials. Most include outpatients;[13,22,29–31] some also include hospitalized ones.[20,23,31] Few include a group of normal controls.[13,19,20] Most do not include pathology data.
Few registries currently rely on data collection solely in paper format.[18,19] In the New York State Dementias Registry, reports were initially on paper, but later included a computerized system designed to extract specific diagnostic codes from hospital discharge databases.[15] Most registries use a digital format.[22,23,25–28]
With regard to publication and access to information, some registries have reported only pilot studies; others have not made their data available.
Another essential factor is diagnostic criteria. Most registries use DSM IV or ICD 9 or 10. Some include specific criteria for various subtypes of dementia, in addition to research criteria for AD.[18,30]
There is no ideal dementia registry. But design features should be selected based on the study’s objective. The registry should strike a balance between simplicity and completeness. Diagnostics employed should be clear and based on the most widely accepted and recommended criteria. There should be flexibility to add new variables in the future, and all patients included in the database should have undergone basic studies (clinical, neuropsychological and neuropsychiatric; as well as laboratory and neuroimaging exams). Patients in predemential or prodromal stages should be included to compile data on the early stages of the disorder. The registry should be easily accessed by other users so as to facilitate multicenter studies. Before starting to use the registry, the user should know, understand and commit to prospectively and consecutively including the variables analyzed for all patients registered, which requires discipline, rigor and perseverance.
Lack of consistency in terminology used by registries hinders access to information. Each registry is unique, with qualitative and quantitative differences in type, case definition, sample size, quality of design, purpose, procedures (to avoid case duplication and for tracking), costs, funding sources, dissemination and communication of results, and short- and long-term impact. This heterogeneity both reflects and contributes to a lack of concrete policies and strategies at the global, national and/or regional levels, and creates obstacles to data extrapolation to the local context. Consistency among registries needs to be improved for the purpose of attaining more homogeneity in reporting across registries.
Most registries reported were designed with clinical-epidemiological purposes to provide global data for health service programs and planning.[13,22,24–28,30] Other registries aim to recruit patients for clinical research on dementia.[23,24,31] Simultaneous establishment of registries with similar objectives and design could go a long way toward addressing the limitations identified.
No longitudinal or cohort studies on dementia have been conducted in Cuba because of the high cost and complexity of the long-term sustainability of such studies. Most epidemiological data on dementia in Cuba have been acquired using a classic epidemiological research model: cross-sectional or prevalence studies, with significant constraints that extend beyond the objectives of this article. Although they provide limited information on the long-term evolution of cases and their impact on the health system, such cross-sectional or prevalence studies cannot be used for determining the real behavior of dementia, its detection, referral and diagnostics in regular clinical practice at the primary, secondary and specialized health care services levels, which is fundamental information for appropriate allotment of social-health resources in the country and rational medium- and long-term planning.
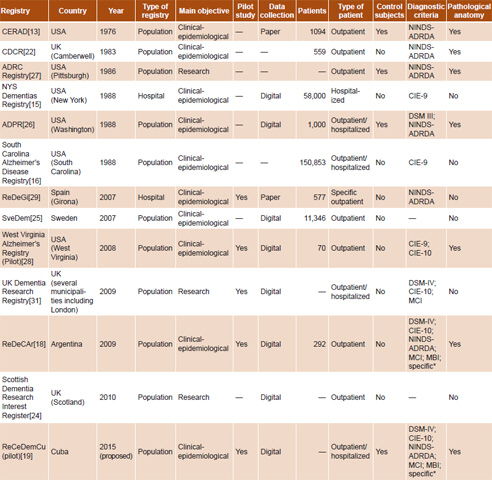
Table 1: Comparative data among cognitive impairment registries

ADPR: Alzheimer’s Disease Patient Registry ADRC: Alzheimer’s Disease Research Center, University of Pittsburgh / CDCR: Camberwell Dementia Case Register / CERAD: Consortium to Establish a Registry for Alzheimer’s Disease / MBI: mild behavioral impairment / MCI: mild cognitive impairment / NINDS-ADRDA: National Institute of Neurological and Communicative Disorders and Stroke, and Alzheimer’s Disease and Related Disorders Association / NYS: New York State / ReDeCAr: Centralized Registry of Cases with Cognitive Impairment in Argentina /ReDeGi: Girona Dementias Registry /ReCeDemCu: Cuban National Dementias Registry / SveDem: Swedish Dementias Registry
— No published data available
*criteria for clinical subtypes
vascular dementia: NINDS–AIREN criteria
degenerative dementia with vascular component
frontotemporal dementia: Lund–Manchester criteria
Lewy body dementia: criteria from Consortium on DLB International Workshop
dementia from progressive supranuclear palsy: NINCDS–SPSP criteria
corticobasal syndrome: Litvan criteria
dementia from multiple system atrophy: AAS–AAN criteria
semantic dementia: Neary criteria
primary progressive aphasia: Mesulam criteria
Application of the epidemiological method to the medical management of dementia and the identification of preventive strategies transcends the individual context to a greater population/environment/public-health context. A preliminary proposal was presented for a national centralized, automated registry on cognitive deterioration and dementia in Cuba[19] during the 50th Annual Scientific Conference of the Neurology and Neurosurgery Institute (INN).
The proposal outlines a plan to implement an automated National Dementias Registry (ReCeDemCu) as a source of clinical-epidemiological data based on the epidemiological surveillance model. A four-module data collection protocol or log for the model has been developed, based on the minimal variables necessary to implement the Registry: a) identification of the health center; b) demographic data and identification of the patient; c) diagnostic data; and d) relevant clinical variables. INN would be the central reference unit and a surveillance network would be set up and uploaded on a secure INN website. The registry’s automated online format would enable 24-hour access for users and researchers throughout the year.
The Registry would enable description of incidence patterns by disease subtype, identify flows of case referrals from primary care, provide information on the workload of health services in different centers, identify patients’ main clinical features, and generate hypotheses for new clinical research projects. Equally important would be the scientific advantage of generating new knowledge, unifying diagnostic criteria, and benefiting research and multicenter studies.
Initially, a pilot study has been proposed, scheduled to begin in 2015 (the design has been in place since 2013 but data collection has not yet begun), to test the operational structure of sentinel centers (hospitals, specialized centers and several primary health care facilities) where registries will be compiled and later extended to the rest of Cuba.[19] Table 1 compares some characteristics of the Cuban proposal with selected international registries in which the author found relevant data.
FINAL CONSIDERATIONS
Cognitive and behavioral disorders constitute a priority health problem, owing to their clinical and social impact, the progressive impairment they produce, and the care needs they create. This health issue needs to be addressed from a multidisciplinary perspective. A family member suffering from dementia has a great impact on his/her family and on society at large. Dementia produces so-called “hidden patients,” namely, the family and, in particular, the primary caregiver. The condition affects the caregiver’s quality of life, makes the patient’s family vulnerable, has financial repercussions and creates the need for special services to assist patients, their caregivers and families.
Registries of patients with dementia provide a fundamental tool for identifying disease patterns in different regions and their variations according to multiple variables (clinical, epidemiological, investigative and administrative), as well as current treatment norms. Despite the wide differences in methods and results that our review found globally, it is extremely important to implement a national dementia registry in Cuba as a source of clinical and epidemiological data and as an efficient strategy to address this chronic disorder and its high social and health costs.
A centralized registry would enable correlation of clinical, neuropsychological, imaging and pathology findings. Epidemiological surveillance, through use and analysis of data from such a registry, would help inform and guide decisionmaking and planning of public health strategies for prevention and improved treatment.
Description and comparison of other registries in this review provide context for Cuba’s first cognitive impairment registry, whose preliminary version, ReCeDemCu, considers the limitations of existing registries and sets goals for improving their design to optimize care of Cuban patients with dementia.