INTRODUCTION
Suicide, a subcategory of intentional self-harm in ICD-10,[1] is defined as an act deliberately initiated and performed by a person with full knowledge or expectation of its fatal outcome.[2]
WHO estimates that over 800,000 people commit suicide each year, representing 50% of violent deaths in the male population and 71% in the female. The number, expected to reach 1.5 million by 2020, is already higher than all deaths caused by war and homicide.[3] According to burden of disease studies, in 2010, self-harm, suicide attempts and deaths by suicide ranked 18th globally in disability-adjusted life years lost (DALY) and constituted 1.5% of all DALY.[4]
WHO ranks suicide as one of the three leading causes of death worldwide in the group aged 15–34 years and it accounts for 12.9% of annual deaths among all age groups.[3] Family history of suicidal behavior, belonging to a cultural subgroup with tolerant attitudes toward suicide, economic difficulties, diminished ability to adapt to new situations, lack of coping strategies, insufficient resources for developing interpersonal relationships, and history of sexual and physical abuse in childhood are factors associated with the epidemiology of suicide.[5,6]
In the Americas, 65,000 deaths by suicide occur annually—12% of deaths by external causes. These proportions vary by PAHO subregion: for example, 19.7% in North America (excluding Mexico) and 7.8% in Central America, Mexico and the Spanish-speaking Caribbean. In Latin America, suicide accounts for 1.3% of DALY.[7]
A substantial upward trend in suicide rates has raised concern among many governments, health systems and international organizations, because policies and programs aimed at prevention and control of suicidal behavior often yield disappointing results.[8] In May, 2013, the 66th World Health Assembly adopted a mental health action plan—the first in WHO history—and proposed a target of a 10% reduction in global suicide rates by 2020.[9] In its Regional Strategies for Mental Health document, PAHO declared suicide prevention one of its highest priorities and proposed suicide rates as an impact indicator.[10]
In Cuba, suicide is the ninth cause of death overall, third in the group aged 10–19 years and fourth in the group aged 15–49 years. Rates increase after age 60 years.[11] The objective of this study was to characterize the epidemiology of suicide in Cuba in 1987 through 2014, including analysis by sociodemographic variables.
METHODS
Study type and data sources A retrospective descriptive study was done using death records from January 1, 1987 through December 31, 2014, retrieved from the database of the Cuban Ministry of Public Health’s National Statistics Division (DNE). Data for denominators for rate calculations also came from DNE.[12]
Variables
Sex: male, female
Age: grouped as <20 years (subgroups 10–14 and 15–19 years); 20–59 years (subgroups 20–29, 30–39, 40–49, and 50–59 years); ≥60 years (subgroups 60–69, 70–79, and ≥80 years)
Skin color: white, black, mestizo, unknown
Marital status: with stable partner, without stable partner, unknown
Employment status/occupation: retiree or pensioner, homemaker, other (includes youth in military service, armed services and working-age individuals who did not disclose their occupation), farmer or fisherman, unemployed, skilled worker, under legal working age, service worker, scientist or academic, not working because of disability, student, unskilled worker, director/manager, office worker, professional or middle-level technician, machine operator, unknown
Methods used for suicide: hanging, self-immolation, poisoning, firearms, jumping from high places, stabbing, self-placement before moving objects, drowning, motor vehicle collision, explosives, electrocution, other
Data collection, processing and analysis DNE authorized use of death records. ICD codes were used to classify suicide: ICD 9: E950–E959 for 1987–2000[13] and ICD 10: X60–X84[1], from 2001 on. Cumulative mortality rates by age group were calculated for the entire study period and the four year period 2011–2014 (considered most representative of the current situation). Crude, adjusted and specific mortality rates per 100,000 population were calculated by sex and age group; the sex ratio (ratio of number of male suicides to number of female suicides) was calculated. Rates were directly standardized to Cuba’s 2002 census population. Relative change in rates was calculated as a percent change and percentages were used to show distribution of variables: sex, age, skin color, marital status and employment status/occupation (to indicate its respective suicide burden), and suicide methods used. DNE code books were used to establish variables. Two code books were used for employment status/occupation, one for 1987–2006, and the other for 2007–2014. An Excel database was created and data were displayed in tables and graphs.
Ethics The study used only death records and population data, exclusively for this research. Collection procedures preserved anonymity of the deceased. The study was approved by the National Hygiene, Epidemiology and Microbiology Institute’s Ethics Committee.
RESULTS
There were 51,113 deaths by suicide in the period studied (annual average 1825), with an average annual age-standardized rate of 16.9 per 100,000 population. From 2011–2014 the average rate was 13.2 per 100,000 population. The rate in 1987 was 23.9 per 100,000 and in 2014 10.8 per 100,000, a decrease of 54.8%.
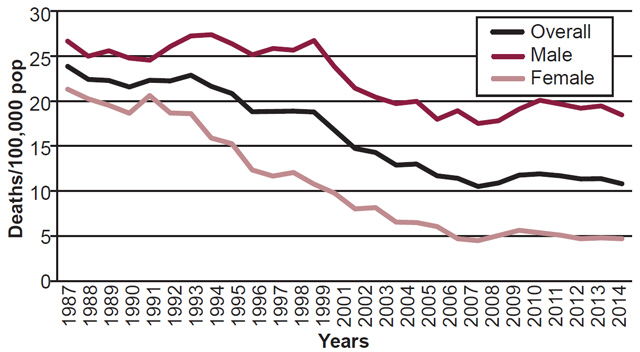
Rates among both sexes declined over the time period, with a slight increase between 2007 and 2010, particularly among men. At the beginning of the period, the age-standardized suicide mortality rate among men was 26.7 per 100,000 population; it reached its maximum in 1994 at 27.4 per 100,000 population, and fell to 18.4 in 2014 (31.1% decrease). The rate was 21.3 per 100,000 among women in 1987 and fell to 4.7 in 2014 (77.9% decrease) (Figure 1).
The age-standardized suicide rate at the beginning of the 2011–2014 period was 11.6 per 100,000, falling to 10.7 in 2014 (7.6% decrease). Among men, the rate fell from 19.6 per 100,000 in 2011 to 18.4 in 2014 (6.1% decrease), while among women it went from 5.1 per 100,000 in 2011 to 4.7 in 2014 (7.8% decrease).
The sex ratio increased over the time period, from 1.1:1 [hereafter, :1 will be left implicit—Eds.] in 1987 to 3.9 in 2014. The mean for the entire period was 2.1, and for 2011–2014 it was 3.9. The lowest sex ratio by age was found in the group aged <20 years at 0.6. This ratio was reversed in 2000 and for the period 2011–2014 the ratio was 2.5. The group aged 20–59 years had a sex ratio of 2, which increased to 4.2 in the 2011–2014. In the group aged ≥60 years the ratio was 2.8 for the whole period and 3.7 in 2011–2014.
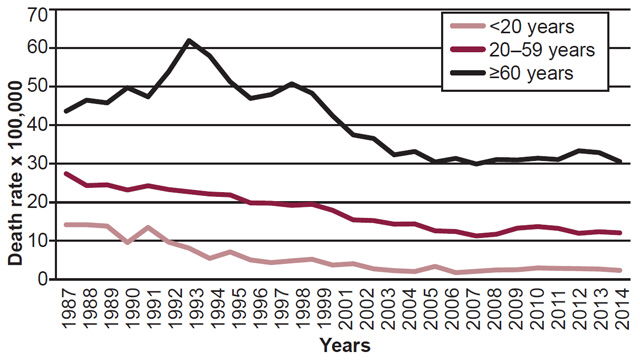
The average suicide rate in the group aged <20 years was 6.5 per 100,000 population over the entire study period, and 2.5 per 100,000 for 2011–2014. In 1987, this age group’s rate was 14.2 per 100,000 population, which decreased to 2.3 in 2014 (Figure 2). The relative decrease was 83.8% for 1987–2014 and 17.9% for 2011–2014 (the rate in 2011 was 2.8 per 100,000 population). This age group accounted for 5.3% of all suicide deaths over the period (Table 1), the proportion dropping to 2.3% for 2011–2014. Within this group, the highest percentage of deaths (88%) occurred in the subgroup aged 15–19 years. The rate in the subgroup aged 10–14 years was 0.4 per 100,000 population, and in those aged 15–19 years was 9.1 per 100,000 population.
The average suicide rate for the entire period in the group aged 20–59 years was 17.5 per 100,000 population, decreasing to 12.4 in 2011–2014 (Figure 2). The rate in 1987 was 27.4 per 100,000 population, falling to 12 per 100,000 in 2014 (56.2%). The rate was 13.2 in 2011, for a relative decrease of 9.1% from 2011–2014. This group accounted for 60.5% of deaths; 30.6% in the subgroup aged 20–39 years and 29.9% in the subgroup aged 40–59 years (Table 1). The rate was 15 per 100,000 population in the subgroup aged 20–39 years and 21 per 100,000 population in the subgroup aged 40–59 years. In 2011–2014, 54.8% of deaths occurred in the group aged 20–59 years (18.2% in the subgroup aged 20–39 years and 36.6% in the subgroup aged 40–59 years).
The group aged ≥60 years had the highest mortality rate, averaging 44.6 per 100,000 population over the entire period, and 31.7 in 2011–2014. In 1987, this group had an age-standardized rate of 43.6 per 100,000 population, which fell to 30.5 in 2014 (Figure 2). The relative decrease for the entire period was 30%, and 1.6% for 2011–2014 (from a rate of 31 per 100,000 population in 2011). This group accounted for 34.1% of deaths by suicide over the study period (Table 1), 25.2% in the subgroup aged 60–79 years and 8.9% in the subgroup aged ≥80 years. The rate was 35.4 per 100,000 population for the subgroup aged 60–79 years age and 74.4 per 100,000 in the subgroup aged ≥80 years.
Figure 1: Suicide mortality rates by sex, Cuba, 1987–2014
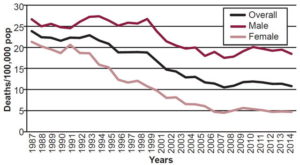
Figure 2: Suicide mortality rates by age groups, Cuba, 1987–2014
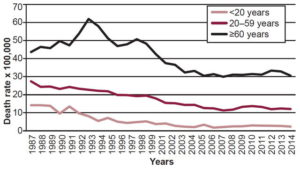
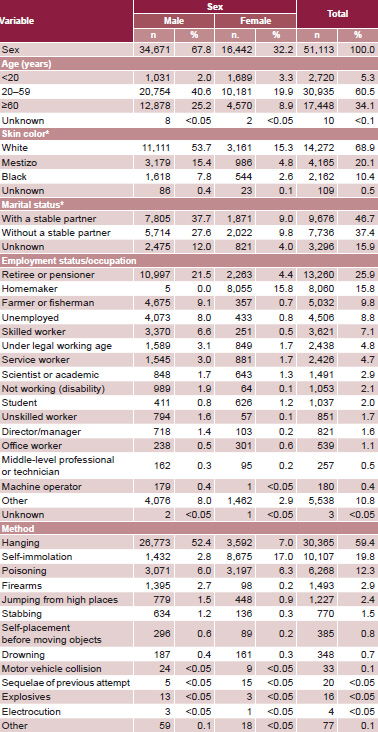
Table 1: Suicides by selected variables, Cuba, 1987–2014

People with white skin accounted for 68.9% of suicides and people with stable partners constituted 46.7% (variables reported from 2001 forward); retirees or pensioners were 25.9% (Table 1).
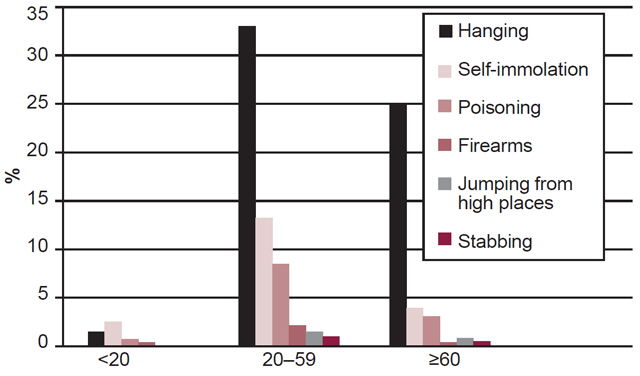
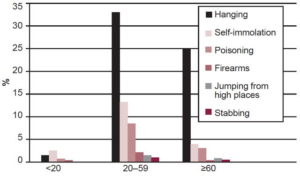
The most widely used method for suicide was hanging, accounting for 59.4% of deaths. This and stabbing were the only methods that showed a relative increase over the study period (0.9% and 10.5%, respectively). The method most used by men was hanging (52.4%), while among women it was self-immolation (17%). Among those aged <20 years, the most common method was self-immolation. In the groups aged 20–59 years and ≥60 years, hanging was the most common (Figure 3, Table 1). From 2011–2014 the predominant method was hanging (79.1%), followed by poisoning (9.3%) and self-immolation (6.9%).
DISCUSSION
The highest age-standardized suicide rate for both sexes combined in Cuba was reported in the first year of the study period, 1987. This is consistent with other research finding that suicide rates in Cuba reached 23 per 100,000 population in the 1980s, prompting a national study by the Ministry of Public Health (results remain unpublished), and design of a suicide prevention program.[14,15]
In 2012 WHO reported global suicide rates of 11.6 per 100,000 population (15 for men and 8 for women). In the same report, Cuba’s overall rate was similar at 11.4 per 100,000 population, but the rate among Cuban men was higher than the international one while among women the rate was lower (18.4 and 4.5, respectively).[16] Although Cuba’s rates have fallen, they are still higher than those reported by PAHO for the Americas, where in 2005–2009 the age-standardized suicide rate was 7.3 per 100,000 population (11.5 among men and 3 among women). The same report showed rates of 9.8 per 100,000 population (14.9 among men and 4.4 among women) in Cuba.[17] The rates among men and women were 8.3 and 2.1 per 100,000, respectively, in Latin America and the Caribbean, lower than the rates we found. Rates in North America (excluding Mexico) were 15.8 per 100,000 among men (higher than among Cuban men) and 4.2 among women (similarly to rates among Cuban women). In South America, Argentina, Colombia, Brazil, Paraguay, Peru, Venezuela and Ecuador had lower rates than Cuba.[17]
Figure 3: Suicide method by age group, Cuba, 1987–2014
Men are most affected in Cuba, which coincides with the global pattern: 79% of all deaths by suicide around the world occur among men.[16] China is the only country in which suicide rates among women are much higher than among men.[16] Men have higher rates of suicide in all age groups in the Americas, with sex ratios ranging between 2 and 6.[17] In our study, women had lower rates and a greater decrease than men did, so the sex ratio has increased and is close to those of other studies—such as in Argentina, Colombia, and Venezuela—with sex ratios of approximately 4. The region comprising Central America, the Spanish-speaking Caribbean and Mexico had the highest sex ratio at 4.2, slightly higher than we observed. The sex ratio in North America (excluding Mexico) is 3.7.[16,17] A 2000 study in Cuba found a sex ratio of 2.2, less than we observed, but it was conducted in only 8 of the then 14 provinces, and thus may not have reflected the national situation.[14]
The highest sex ratio was found among persons in the group aged 20–59 years, which does not coincide with other reports claiming that gender gaps in suicide rates are higher among people aged ≥60 years, as in the Americas where the sex ratio in this group is 7.9, higher than the findings in this study.[17]
The lowest sex ratio in Cuba was found among children and adolescents (<20 years), which is similar to PAHO’s report of the lowest sex ratio (2.2) in this age group.[17] During the first half of the period studied, the sex ratio was less than 1, but after 2000 the trend was reversed and now male children and adolescents are most affected. This coincides with a study conducted among US adolescents from 2004–2012, which reported 73.6% of suicides in this group in the male population.[18]
Suicidal behavior among adolescents is an increasingly common mental health problem in several countries, including Cuba.[18–20] There are national reports showing that severe family dysfunction, broken intimate relationships, history of suicide attempts, alcohol and drug use, hopelessness, depression or other mental disorders increase the risk of suicide.[19,21] According to the Health Statistical Yearbook, people aged 15–19 years made up 27% of the Cuban population aged <20 years in 2015,[22] but accounted for 88% of suicides in the group aged <20 years from 2011–2014. This is a clear, albeit indirect, expression of this age group’s increased vulnerability to the causes of suicidal behavior. Possible contributing factors include the need to reaffirm one’s independence in later stages of adolescence, including expressions of rebellion, “acting out,” anxiety and depression, increased conflict with adults and peers, difficulty complying with social norms, all of which make them more prone to suicide.[23,24] Adolescents experience substantial stress, confusion and pressure to succeed. Some are extremely bothered by their parents’ divorce, the formation of a new family, relocation and natural disasters, among other events, leaving them disturbed with intensified self-doubt, consequently increasing suicide risk.[24,25]
The group aged 20–59 years had the second highest mortality rate. PAHO reported rates for the Americas of 9.2 and 11.9 per 100,000 population for the groups aged 20–44 and 45–49 years, respectively,[17] rates lower than we found for Cuba. These groups are made up mainly of students or workers, in whom economic and social problems (such as providing care for children and/or the elderly, bearing the brunt of family responsibilities, the stress of everyday life, and other risk factors such as alcohol and drug abuse, family conflict, depression and anxiety) may have influenced suicidal behavior. A study conducted in Havana in 2010 revealed that suicide was the second highest cause of death in the 46–55 years age group, at 19.4%. The authors associated this with alcohol consumption, loss of motivation and interests, and premature aging.[26]
The group aged ≥60 years had the highest suicide rate, especially in the 1990s, a decade when economic and social problems in the country worsened, with scarcity of food, transport, electricity and medications, and difficulties in recreation and other aspects of daily life. Stress during this period may have influenced suicidal behavior.[27,28] WHO reports the highest suicide rates worldwide in the group aged ≥70 years, as did we.[16] PAHO Americas Regional Report found a rate of 12.4 per 100,000 population[17]—lower than what we found in Cuba.
Cuba’s aging population is a major demographic concern. By 2050, Cuba (along with Barbados) will have the oldest population in Latin America and the Caribbean, and one of the oldest populations in the world.[29] Cuba’s health system must be ready to provide care for the elderly population. Studies among older Cuban adults have identified depression and anxiety, unmet needs, bereavement, chronic illness, social deprivation, family conflicts, unfavorable economic situations, isolation and feelings of hopelessness, among others, as risk factors for suicidal behavior.[30,31] Old age can bring reduced incomes; loss of physical or cognitive ability; loss of family, friends and social roles once enjoyed earlier in life, and unmet needs. Although some of these can be avoided, some are inevitable.[32,33] Older adults need the understanding and protection of both family and society.
About 55% of the Cuban population has white skin (self-reported)[34] but they accounted for a higher proportion of suicides in our study, consistent with a 2000 study in Cuba that found the distribution of suicide among persons with white, black and mestizo skin color to be 79%, 20% and 0.9%, respectively.[14] A US study reported that cultural differences and ethnicity can affect suicide risk, noting lower suicide rates among Hispanic and African Americans than among white Americans. The authors commented that strong family relationships among Hispanic Americans could help explain their suicide rate 50% lower than that of white Americans, and that the social support systems in Black churches could similarly contribute to lower suicide rates among African Americans.[35]
Retirees or pensioners and homemakers were the most affected occupational groups, also in keeping with the 2000 Cuban study cited earlier.[14] Low income, diminished quality of life and other previously mentioned age-related challenges could help explain this.[31,33] With respect to marital status, the largest group was people with steady partners, a finding common to our study and the 8-province Cuban study in 2000. The authors of that study theorized that if a marriage lacked strong affective and spiritual ties, there would be deficits in communication and support needed to face adversity.[14] Other studies have observed an association between lack or loss of a stable partner and suicide.[30–32] Without data for the denominators needed for rate calculations, we are unable to speculate on whether our results are associated with effect of marital status in either direction.
Methods of suicide are influenced by sociocultural factors to the extent that individual attitudes and lifestyle reflect prevailing national or community customs.[35] The most common methods used in the Americas are hanging (39.7%), firearms (33.3%) and poisoning (18.2%).[17] Hanging was the main method used by both sexes in the last four years of the period we studied, consistent with the 2000 study.[14] The proportion of suicides by hanging is similar to ours in the region of Central America, the Spanish-speaking Caribbean and Mexico (64.3%), and in South America (58.2%).[17]
That poisoning ranked third in Cuba for the entire study period and second for 2011–2014 is consistent with PAHO’s report on suicide in the Americas, where poisoning ranked second in the Spanish-speaking Caribbean at 18.7% and first in the rest of the Caribbean, at 47.3%, higher than the proportion we discovered.[17]
The proportion of suicides using firearms is almost 20 times greater in North America (excluding Mexico) than we found in Cuba: North America has the highest rate of suicides by firearms in the Americas, where 47.2% of suicides are by firearms (Canada 15%, USA 51%).[16] In the Americas, the biggest difference between men and women in method of suicide was in the use of firearms, with men using them 1.9 times more often than women. Women who commit suicide are 2.7 times more likely than men to use poisoning as a method, and 4.2 times more likely to die by self-immolation.[17]
We are interested in examining statistics on methods because controlling access to means of suicide is part of WHO’s proposed suicide prevention plan. Unlike the USA, access to firearms in Cuba is very limited. Given that impulsivity is a trait often associated with suicidal behavior, availability and easy access to lethal means can increase risk of suicide.[16,17]
A major limitation of this study relates to DNE code books and the fact that values for the variable employment status/occupation are out of date. They still define retirement age as 55 years for women and 60 years for men, but these have been extended to 60 years for women and 65 years for men, so that some older working adults could have been wrongly classified as retired, which affects the distribution of burden by occupation. There are no codes for self-employed workers, a relatively new occupational category in Cuba, and the category other includes both military and other nonspecified occupations, preventing specific analysis. Also, skin color and marital status were not recorded on death certificates until 2001, and these variables could therefore not be analyzed for the full period. Finally, although providing proportions of suicides for variables such as occupation and skin color was intended to indicate distribution of suicide burden, not to convey risk, readers might be inclined to interpret a result as an indicator of risk, when it merely reflects population composition.
In spite of these limitations, the study is important because it describes the characteristics of suicide in Cuba over a period of almost three decades.
CONCLUSIONS
The study analyzes the epidemiology of suicide in Cuba, a topic that has been little studied until now. Although suicide rates fell over the study period by more than 50%, they remain higher than rates for the Americas. The results can contribute to the development of programs and policies aimed at reducing an important preventable cause of death in Cuba.
ACKNOWLEDGMENTS
The authors thank scientific and technical information specialists, Silvia Serra-Larín and María del Carmen Hinojosa-Álvarez, for their help in the literature review, and Dr Pedro López-Saura for his assistance and advice.