
INTRODUCTION Ferritin is the best biomarker for assessing iron deficiency, but ferritin concentrations increase with inflammation. Several adjustment methods have been proposed to account for inflammation’s effect on iron biomarker interpretation. The most recent and highly recommended method uses linear regression models, but more research is needed on other models that may better define iron status in children, particularly when distributions are heterogenous and in contexts where the effect of inflammation on ferritin is not linear.
OBJECTIVES Assess the utility and relevance of quadratic regression models and quantile quadratic regression models in adjusting ferritin concentration in the presence of inflammation.
METHODS We used data from children aged under five years, taken from Cuba’s national anemia and iron deficiency survey, which was carried out from 2015–2018 by the National Hygiene, Epidemiology and Microbiology Institute. We included data from 1375 children aged 6 to 59 months and collected ferritin concentrations and two biomarkers for inflammation: C-reactive protein and α-1 acid glycoprotein. Quadratic regression and quantile regression models were used to adjust for changes in ferritin concentration in the presence of inflammation.
RESULTS Unadjusted iron deficiency prevalence was 23% (316/1375). Inflammation-adjusted ferritin values increased iron-deficiency prevalence by 2.6–4.5 percentage points when quadratic regression correction model was used, and by 2.8–6.2 when quantile regression was used. The increase when using the quantile regression correction model was more pronounced and statistically significant when both inflammation biomarkers were considered, but adjusted prevalence was similar between the two correction methods when only one biomarker was analyzed.
CONCLUSIONS The use of quadratic regression and quantile quadratic regression models is a complementary strategy in adjusting ferritin for inflammation, and is preferable to standard regression analysis when the linear model’s basic assumptions are not met, or when it can be assumed that ferritin–inflammation relationships within a subpopulation may deviate from average trends.
KEYWORDS Alpha-1-acid glycoprotein, C-reactive protein, anemia, iron deficiency, ferritin, acute phase protein, Cuba
INTRODUCTION Anemia is a public health problem worldwide and is most prevalent in preschool children, for whom it is the most frequent cause of nutritional deficits. In turn, iron deficiency is the main cause of anemia, affecting 43% of children globally. Previous studies in Cuba show rates of iron deficiency in preschool children between 38.6% and 57.6%, higher in infants (71.2% to 81.1%). WHO recommends using serum ferritin as an indicator of iron deficiency accompanied by acute (C-reactive protein) and chronic (α1-acid glycoprotein) inflammation biomarkers.
OBJECTIVE Assess how inflammation affects measuring and reporting of iron-deficiency anemia rates in Cuban preschool children.
METHODS Data were obtained from serum samples contained in the National Anemia and Iron Deficiency Survey, and included presumably healthy preschool Cuban children (aged 6–59 months). Serum samples were collected from 1375 children from randomly selected provinces in 4 regions of the country from 2014 through 2018. We examined the association between ferritin and two inflammatory biomarkers: C-reactive protein and α1-acid glycoprotein. Individual inflammation-adjusted ferritin concentrations were calculated using four approaches: 1) a higher ferritin cut-off point (<30 g/L); 2) exclusion of subjects showing inflammation (C-reactive protein >5 mg/L or α1-acid glycoprotein >1 g/L); 3) mathematical correction factor based on C-reactive protein or α1-acid glycoprotein; and 4) correction by regression with the method proposed by the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia Group. We estimated confidence intervals of differences between unadjusted prevalence and prevalence adjusted for inflammation by each method.
RESULTS The proportion of children with inflammation according to C-reactive protein concentrations >5 mg/L was lower (11.1%, 153/1375) than the proportion measured according to the concentrations of α1-acid glycoprotein, at >1 g/L (30.8%, 424/1375). The percentage of children with high concentrations of at least one of the aforementioned biomarkers was 32.7% (450/1375). Thus, each correction method increased the observed prevalence of iron deficiency compared to unadjusted estimates (23%, 316/1375). This increase was more pronounced when using the internal regression correction method (based only on C-reactive protein) or the method based on a higher cut-off point. Adjustment using all four methods changed estimated iron deficiency prevalence, increasing it from 0.1% to 8.8%, compared to unadjusted values.
CONCLUSION One-third of preschool children had biomarkers indicating elevated inflammation levels. Without adjusting for inflammation, iron deficiency prevalence was underestimated. The significant disparity between unadjusted and inflammation-adjusted ferritin when using some approaches highlights the importance of selecting the right approach for accurate, corrected measurement. The internal regression correction approach is appropriate for epidemiological studies because it takes into account inflammation severity. However, other models should be explored that account for inflammation and also provide better adjusted ferritin concentrations.
KEYWORDS Anemia, iron deficiency; child, preschool; inflammation; Cuba
INTRODUCTION Cirrhosis of the liver is a chronic disease that is widespread and irreversible. It represents the final stage of numerous diseases that affect the liver. By the end of 2017, it was the 11th most common cause of death, with a loss of 41.4 million years of disability-adjusted life years, which represent 2.1% of the total years of life lost in the global mortality burden. In Cuba, cirrhosis and other chronic liver diseases have been among the top 10 causes of death for several decades, their rates consistently increasing, from 576 deaths in 1970 (6.7 per 100,000 population) to 1738 in 2017 (15.5 per 100,000 population), with a risk of death that is 4.6 times higher in men.
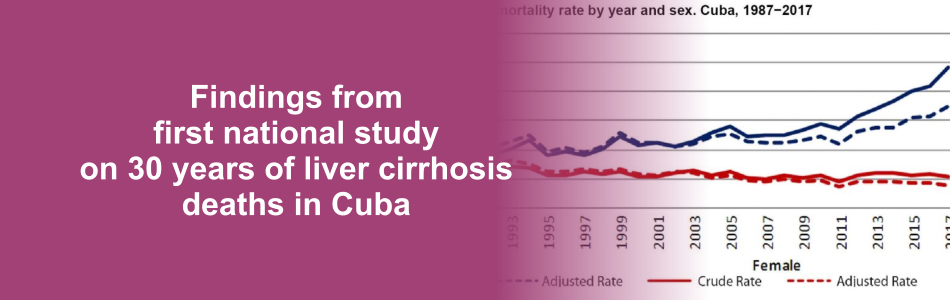
OBJECTIVE Characterize deaths from cirrhosis of the liver in Cuba from 1987 to 2017.
METHODS An ecological time-series study was conducted for 1987 to 2017 using information obtained from the mortality database of the Medical Records and Health Statistics Bureau of Cuba’s Ministry of Public Health. The study universe consisted of all deceased persons in the country whose underlying cause of death was cirrhosis of the liver. Both general mortality rates and specific mortality were calculated by age group, sex and etiological classification using adjusted and crude rates. Rates were age-adjusted using the direct method, and the population from the 2002 Census of Population and Housing was considered as the standard population. Percentages and means were also calculated according to selected variables and the relative risk of death due to the disease according to sex, age group and etiological classification. The trend and forecast for mortality rates were estimated for this disease.
RESULTS The crude mortality rate from cirrhosis of the liver was 9.0 per 100,000 population for the period. Those aged ≥75 years had the highest risk of death (48.3 per 100,000 population). The crude and adjusted mortality rates were almost double for men (12.4 vs. 5.6 and 11.7 vs. 5.6 per 100,000 population, respectively), as was the total relative risk of death, which was 2.2 times higher. Nonalcoholic cirrhosis accounted for 71.6% of deaths. By the end of 2017, risk of death from cirrhosis had climbed to 14.8 per 100,000 population (adjusted rate: 10.6 per 100,000 population), a signal that mortality had progressively increased over the 31 years analyzed. In addition, forecasts predict that death rates will continue their gradual increase, reaching 19.2 per 100,000 population in 2025.
CONCLUSIONS Deaths from cirrhosis of the liver constitute a substantial health burden in Cuba. The upward trend and forecast, in addition to increased risk of mortality in men and older adults, are similar to those reported internationally. The finding that most of these deaths result from nonalcoholic cirrhosis should be further studied, as formulation of effective public health strategies depends largely on attaining a better understanding of the etiology, progression and social determinants of the disease.
KEYWORDS Liver cirrhosis, alcoholic liver cirrhosis, fatty liver, mortality, Cuba
INTRODUCTION Recent decades have seen an uptick in suicide attempts and completed suicides among adolescents and young adults worldwide. In the Americas, including Cuba, suicide is the third leading cause of death in adolescents (ages 10–19 years).
OBJECTIVE Characterize the epidemiology of attempted and completed suicide in Cuban adolescents from 2011 through 2014.
METHODS A descriptive epidemiological study was carried out. The information was gathered from morbidity records for suicide attempts and mortality records for suicide deaths in adolescents, taken from the Cuban Ministry of Public Health’s Medical Records and Health Statistics Division database for January 1, 2011 through December 31, 2014. Variables were sex, age, occupation or employment status, and suicide method. Suicide attempt incidence rates and suicide mortality rates by age group per 100,000 population (crude, adjusted and age/sex specific), mortality sex ratio and attempt/suicide ratio were calculated. Relative change was calculated as a percentage, as were frequencies by variable for attempted suicide and suicide, and by age and sex for method used.
RESULTS A total of 19,541 suicide attempts and 149 suicides were reported. Average annual numbers were 4,885.2 suicide attempts and 37.2 suicides (131:1 ratio). There were 3,966 suicide attempts among boys, for a sex ratio of 0.25:1. Age-adjusted suicide attempt rates decreased from 391.8 per 100,000 population to 304.5 (22.3% reduction over the study period). Boys accounted for 107 of 149 suicide deaths, for a sex ratio of 2.5:1. Age-adjusted suicide mortality rates decreased from 2.8 to 2.3 per 100,000 population (17.9% reduction). The group aged 15–19 years had the highest age-adjusted suicide rate (3.9 per 100,000 population) and contributed the most deaths (114/149, 76.5%), although it did experience a 31.8% reduction over the study period. The group aged 10–14 years recorded a relative increase of 60% over the study period. Hanging was the most common suicide method (116/149, 77.9%). The suicide rate in Cuban adolescents (2.6 per 100,000 population, 3.7 in boys and 1.5 in girls) is less than that reported by the Region of the Americas between 2005 and 2009, 3.7 per 100,000 population (5/100,000 in boys and 2.3/100,000 in girls).
CONCLUSIONS Suicide rates in Cuban adolescents are lower than reported elsewhere in the Americas. Suicide attempts and suicide rates decreased modestly between 2011 and 2014. Hanging is the most commonly used method. The highest rates occur in the group aged 15–19 years, but those aged 10–14 years showed a relative increase over the study period. These results update the epidemiology of suicide in Cuban adolescents and demonstrate the extent of the problem. Suicides and suicide attempts show opposite patterns in boys and girls; suicides are more frequent among boys while suicide attempts are more frequent among girls.
KEYWORDS Suicide, suicide, attempted, mortality rate, adolescents, Cuba
CONTRIBUTION OF THIS RESEARCH These results update the epidemiology of suicide in Cuban adolescents and reveal the extent of the problem for one of the main preventable causes of death in this age group.
INTRODUCTION Systematic measurement of population physical activity levels is an important component of public health surveillance.
OBJECTIVES Describe patterns of physical activity in the Cuban population aged 15–69 years and identify factors associated with regular physical activity.
METHODS A descriptive cross-sectional study was conducted using a complex sampling design, representative of urban and rural areas, sex and age groups, including 7915 individuals. The International Physical Activity Questionnaire (short format) was applied. The population was classified as active, irregularly active and sedentary, according to sex, age, marital status, education, skin color, employment and perception of health risk related to physical inactivity or overweight. Percentages, odds ratios (OR) and 95% confidence intervals (CI) were calculated and a multinomial regression model was fitted with active persons as the reference category.
RESULTS Approximately 71% of the population self-classified as active, 23% as sedentary and 5.9% as irregularly active. Women had a higher probability of being sedentary (OR 2.51, CI 2.12–2.98) and irregularly active (OR 2.56, CI 95% 1.87–3.49). The probability of being sedentary increased with age (OR 1.19, CI 1.12–1.26), and also with the condition of being a homemaker, retired, or unemployed. Perceiving overweight as a high risk to health reduced likelihood of inactivity (OR 0.49, CI 0.29–0.83).
CONCLUSIONS Some 7 of 10 Cubans are physically active. The groups with the highest probability of inactivity and irregular activity and associated factors have been identified through national application (for the first time) of the International Physical Activity Questionnaire. The results should be taken into account for implementation of specialized strategies to promote systematic physical activity.
KEYWORDS Physical activity, physical exercise, sedentary lifestyle, health behavior, risk factors, chronic disease, women’s health, surveillance, Cuba
INTRODUCTION Suicide is a health problem influenced by biological, genetic, psychological, social and economic factors. It is responsible for 50% of violent deaths in the male population, worldwide, and 71% in the female. In the Americas, 65,000 deaths by suicide occur every year. It is the ninth most frequent cause of death in Cuba, and third among people aged 10–19.
OBJECTIVE Characterize the epidemiology of suicide in Cuba from 1987 to 2014.
METHODS A retrospective descriptive study was conducted. The information comprised all records of death by suicide from January 1, 1987 to December 31, 2014, in the Cuban Ministry of Public Health’s National Statistics Division database. The variables were sex, age, skin color, employment status/occupation, marital status, and method of suicide. Crude and age-standardized mortality rates and age–sex specific mortality rates were calculated, all per 100,000 population, as well as the sex ratio. Relative change over the series was calculated as a percentage. Distribution of suicides by variable was calculated and proportions expressed as percentages.
RESULTS A total of 51,113 deaths by suicide were reported (annual average 1825), of which 34,671 (67.8%) were among men. The sex ratio was 2.1:1 for the entire study period, and 3.9:1 for 2011–2014. Over the course of the period studied, age-standardized suicide rates decreased from 23.9 to 10.8 per 100,000 population (54.8% reduction). The group aged ≥60 years had the highest average age-standardized rate, 44.6 per 100,000 population. The highest suicide burden by age was in the group aged 20–59 years (60.5%). By skin color, the highest burden was in those recorded as white, 68.9%. By marital status, the highest burden was in persons with a stable partner (46.7%), and by employment status/occupation, in retired (25.9%). The most commonly used method was hanging (59.4%).
CONCLUSIONS Over the course of about three decades, suicide mortality rates have declined by almost half and they are still slightly higher than overall rates in the Americas. The most commonly used method is hanging. The sex ratio is greater than two and has increased over time. The highest rates occur in the group aged ≥60 years, but finer stratification is needed to identify an age-related risk trend. In view of Cuba’s aging population, these results are of interest for epidemiology and public health.
KEYWORDS Suicide, suicide attempt, death, mental health, Cuba
