INTRODUCTION
Atherosclerosis is a chronic, progressive, systemic disease that mainly affects medium-sized arteries. It is the underlying cause common to cardiovascular diseases, and is considered the primary cause of morbidity and mortality worldwide,[1] a major contributor to disability and decreased quality of life in countries where non-communicable chronic diseases have surpassed infectious diseases as main population health problems.[2] From a social and economic standpoint, atherosclerosis is one of the major destroyers of human health, a disease that exacts the highest toll in death and sequelae.[3]
Health systems have also had to pay a high price for developments in diagnosis and treatment of atherosclerotic diseases. Prevention is the only way of containing these growing costs, while contributing to the benefits of improved health and quality of life.[4–6]
Atherogenesis, the development of atherosclerosis, is a process that begins at conception and reflects several risk factors in combination. Research to identify atherogenic risk factors in children and adolescents shows that precursor events to adult atherosclerotic disease (unhealthy behaviors difficult to modify in adulthood such as poor dietary habits, physical inactivity and smoking) occur early in life.[7–9] Early detection and control of these factors during adolescence would reduce incidence of cardiovascular disease and its complications in adults.[2]
Early signs of atherogenesis (ESA) are manifestations of atherosclerosis or known atherogenic risk factors present at a young age (before age 34 years) detectable by health professionals before clinical manifestations of atherosclerosis. They include symptoms, signs, syndromes or diseases accepted in international literature as atherogenic risk factors or consequences of atherosclerosis. ESA include the following:[2]
- hypertension (HT), systolic and/or diastolic
- excess body weight
- excess waist circumference
- type 2 diabetes
- high induced or fasting blood glucose
- insulin resistance
- glucose intolerance
- high total serum cholesterol and lipoproteins
- high postprandial blood lipids and glucose
- active or passive smoking
- low birth weight
- poor childhood nutrition
- physical inactivity
- family history of risk factors for, or sequelae of, atherosclerotic diseases at relatively young ages
Since 1970, the Cuban Ministry of Public Health’s Growth and Development Group has conducted a series of studies to understand changes in the physical development and nutritional status of Cuban children and adolescents. Their findings confirm an increasing trend towards higher prevalence of overweight and obesity in recent years.[10,11]
ESA have been identified as a research priority by Havana’s Atherosclerosis Research and Reference Center (CIRAH) and have been the object of several Cuban studies in adolescents.[12] This study was conducted to identify ESA among adolescents in the geographic catchment area of Family Doctor-and-Nurse Office (CMF) No. 13 of the Raúl Gómez García Polyclinic, in order to increase understanding of the topic and contribute to recommendations for prevention strategies in primary care.
METHODS
Design, population and sample A cross-sectional descriptive study was conducted from December 2011 to March 2013 in the above-mentioned CMF. The study universe consisted of 110 adolescents enrolled in the CMF, an office responsible for primary care services offered to the entire population in the surrounding neighborhood (approximately 365 families or 1096 patients). Included were adolescents (aged 10–19 years) in the CMF catchment area; excluded were adolescents with secondary causes of risk factors or diseases under study, who were pregnant or puerperal, or who were outside the area at time of study. The final sample consisted of 96 adolescents.
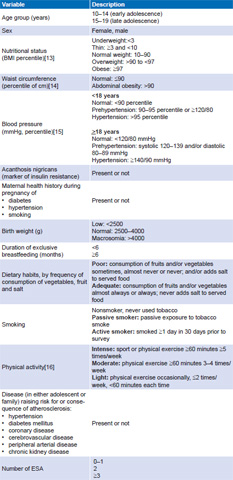
Variables and data collection Detailed in Table 1, variables included age, sex, medical history and physical findings, maternal factors during pregnancy, and first-degree family medical history.
A questionnaire based on CIRAH’s data collection model was created to record sociodemographic data, results of physical exam, prenatal and birth history, breastfeeding duration, dietary and smoking habits, physical activity, and personal and family medical history (siblings, parents and grandparents), obtained through interviews with the participant or with the mother (preferably) or guardian. All interviews and measurements were conducted at an appropriate place, in a well-lit and private space, according to standard procedures. To reduce bias, the same person carried out all physical measurements.
Analysis SPSS v.15.0 for Windows was used for data processing. Descriptive data were used, with results expressed in frequency distribution tables and charts. The chi-square and Fisher exact tests were applied to detect differences between sexes and age groups regarding atherogenic risk factors and number of ESA (significance threshold p = 0.05).
Ethics Written informed consent was obtained from adolescents and parents or guardians following explanation of study objectives and importance of participation. Confidentiality was assured, as was the option of dropping out of the study without repercussion for subsequent medical attention.
Table 1: Variables

ESA: early sign of atherogenesis
RESULTS
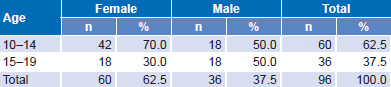
Of 96 adolescents studied, 60 (62.5%) were female and 60 (62.5%) were in early adolescence (aged 10–14 years); 50% of male participants were in the group aged 10–14 years (Table 2).
Table 2: Sample age and sex distribution
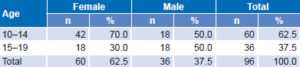
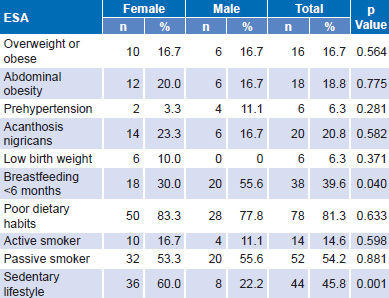
Table 3: ESAs by sex
ESA: early sign of atherogenesis
Among maternal prenatal atherogenic risk factors, smoking during pregnancy was the most frequently reported (14.6%), followed by HT (10.4%) and diabetes (6.3%).
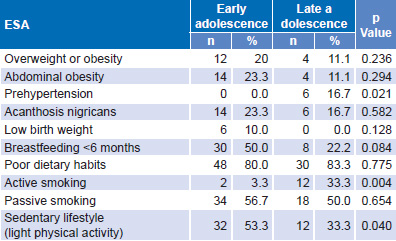
Table 3 displays distribution of atherogenic risk factors by sex. Leading the list are poor dietary habits (81.3%), followed by passive smoking and sedentary lifestyle. Only breastfeeding < 6 months and sedentary lifestyle showed a significant sex difference (p = 0.04 and 0.001, respectively), with greater prevalence of the latter among female participants. Table 4 shows distribution of risk factors by age group, with prehypertension and active smoking predominating in late adolescence by a statistically significant difference, in contrast to sedentary lifestyle, which was more frequent in early adolescence, also statistically significant.
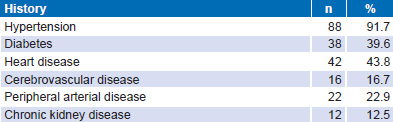
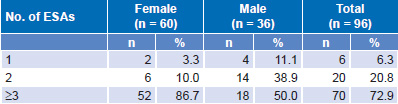
Table 5 displays family history of risk factors and atherosclerotic diseases, with HT predominating at 91.7%. All adolescents had ≥1 ESA and 72.9% had ≥3 ESA, with higher prevalences in female than in male participants (p = 0.022) (Table 6). There was no significant difference between age groups (p = 0.067); 76.7% of adolescents aged 10–14 years and 66.7% of those aged 15–19 had ≥3 ESA.
Table 4: ESAs by age group

ESA: early sign of atherogenesis
Table 5: Family history of atherogenic risk factors and related diseases
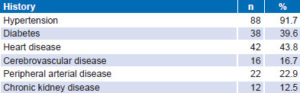
Table 6: Number of ESAs by sex
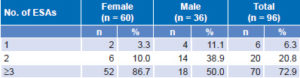
p = 0.022
ESA: early sign of atherogenesis
DISCUSSION
Development of atherosclerosis is related to a confluence of multiple risk factors, including prenatal history of atherogenic risk factors. Our finding that tobacco use during pregnancy was the most frequent maternal antecedent is consistent with reports that 12%–20% of pregnant women smoke (worldwide), a figure that may be low because of pregnant smokers’ tendency to underreport.[17] The complex of disorders affecting the unborn child of a woman who smokes during pregnancy is known as fetal tobacco syndrome. Its consequences include low birth weight, neonatal endocrine disorders, DNA abnormalities, increased perinatal mortality, increased risk of childhood cancer, and altered lung function. Maternal tobacco use is also a leading preventable cause of SIDS and doubles its risk.[18] Lipid abnormalities have been described in newborns of smoking mothers as well.[19]
Other results from our study emphasize the high prevalence of overweight, obesity and abdominal obesity, similar to findings from other research with adolescents.[8,9,20–23] Over the past two decades, obesity has become epidemic in most countries.[24] In Havana, the proportion of children and adolescents with high levels of adiposity rose from 13.3% in 1972 to 28.9% in 2005.[10]
Among atherogenic risk factors in adolescents, poor dietary habits were the most important ones detected. Adequate nutrition is fundamental for adolescents to achieve growth milestones according to their genetic potential, and to prevent short- and long-term harm to health from poor or unbalanced food intake.[25,26] Adolescence is a complex stage of profound changes in all spheres of life. Poor dietary habits develop during this process due to cultural factors, social needs and the desire for independence characteristic of this life stage. Obesogenic dietary habits are characterized by disordered eating, low fruit and vegetable consumption, and high consumption of high-caloric, low-nutrient foods and foods rich in saturated and trans fats.[26–28]
Palenzuela’s study of Spanish adolescents found deficient consumption of milk products, pasta, fruits and vegetables, and significant consumption of foods with “empty calories” (fast food, sweets, soft drinks).[29] Similar results were obtained by the HELENA study of a broad sampling of European adolescents.[30] In Cuba, several studies have identified poor dietary habits as an important atherogenic risk factor in adolescence.[8,9,31] A study of seventh-grade students’ dietary habits in Havana’s 10 de Octubre Municipality also found inadequate consumption of fruits and vegetables to be frequent.[27]
Tobacco use usually begins in childhood or adolescence.[32] A high percentage of adolescents studied are either passive or active smokers, with no significant differences by sex. However, differences by age group among active smokers were significant, coinciding with various studies, including Gulayín’s in Argentina, which showed an average age of 13.8 (SD 1.7) years at smoking initiation, and smoking students’ mean age of 15.7 (SD 1.3) years. The study also identified substantial exposure to secondhand smoke both at home and from friends.[33] Statistics from Cuba’s 2010 National Survey on Risk Factors and Chronic Diseases found 10.4% prevalence of tobacco use in the group aged 15–19 years; that 25% of those surveyed began smoking at ages 15 and 16 years; and that 75% began smoking before age 20.[34] This survey and others in Cuba and Spain indicate that male adolescents smoke more than female adolescents,[20,21,32,35] although smoking in female adolescents has been reported to be increasing in Spain.[36] So it is noteworthy that we observed higher prevalence of smoking in female than in male adolescents. Gulayín’s study also identified female sex as a predictor of tobacco use in this age group, as well as older age, living with a smoker and having a mother and/or friends who smoke.[33]
Our finding that passive smoking was the second most frequent atherogenic factor coincides with Cuban research among adolescents[20,21,35,37] reporting a similarly high proportion of passive smokers. Exposure to secondhand smoke is as prevalent inside the home as it is outside. This underscores the importance of greater engagement with family and community, especially in primary and secondary schools, in health education in general and antismoking education programs in particular, in order to exercise greater influence on adolescent behavior, above all through parents, to facilitate prevention of complications associated with this toxic habit.
Among lifestyle factors observed in this age group, low levels of physical activity are of concern because they lead to excess weight and risk of other dysmetabolic parameters. Sedentary lifestyle, especially in adolescence, is a growing problem, as reported in several studies in this field.[21,32,38] The pull of television, video games and computer use tends to keep youngsters indoors, and lack of safety discourages outdoor recreation in some larger cities,[38] the latter not a factor in Cuba. Actions with this age group should be intensified to promote physical exercise as a healthy lifestyle from early childhood.
Sex differences observed indicate the importance of integrating into the study of health and lifestyles the psychosocial variables of social structure, in which gender plays a leading role. Hernández’s research in Cuba shows how, beginning in infancy, habitat and gender influence lifestyle, owing to many factors that require additional study, among them cultural traditions and the role of our schools and other institutions.[39] Thus, it is essential to apply a gender lens in planning community interventions to achieve healthy lifestyles for both sexes.
Primary health care provides conditions and opportunities to identify atherogenic risk factors among adolescents. Timely assessment to eliminate or minimize these factors is the first step in prevention or delay of disease development, and should be a priority task of family physicians and nurses, pediatricians, parents, relatives and teachers. All primary care workers should promote healthy lifestyles from a comprehensive, family perspective.
It is critical to remember that the atherogenic risk factors presented in the study (poor dietary habits, passive smoking and low physical activity) are modifiable, susceptible to educational interventions for primary prevention of cardiovascular disease, and responsive to actions in organized exchanges with family members, children, adolescents and their health teams.
As to family history of atherogenic risk factors, HT predominates, consistent with the conclusions of a study at the Central Havana Pediatric Hospital, which found such risk factors in 94% of children and adolescents.[21] Family history of HT is a predictor of HT in adolescence,[40] and parental HT has been associated with increased inflammatory mediators and atherosclerosis.[41] Argentina’s FRICELA study found a correlation between parental HT and adolescent blood pressure levels.[32] A history of parents, siblings and grandparents who developed coronary disease before age 55 years in men and age 65 years in women carries increased risk of cardiovascular disease, with risk increasing proportionately to earliness of onset and number of family members affected.[42]
Detection of a cardiovascular risk factor is markedly affected by the intensity of coexisting risk factors. Epidemiological and clinical studies have shown that individuals with multiple risk factors have substantially increased risk of cardiovascular disease compared with individuals having a single factor and that cardiovascular risk factors tend to cluster in individuals.[43] So it is alarming that all adolescents in our study had at least one ESA, and most had three or more, especially female participants. Two studies of children and adolescents in Havana found similar results,[20,21] although number of ESAs by sex was reported only in the latter study, whose subjects had essential HT. Larger sample sizes are needed to study this issue, and a gender perspective should be applied to analyze possible factors influencing these findings. Health promotion and prevention actions must be directed at all adolescents, but especially girls and young women, where ESAs predominate.
Among the limitations of this study is the small sample size, which could have impeded detection of other differences and rules out extrapolation to other populations. Only one facet of the broad topic of dietary habits was explored, without addressing such important elements as consumption of sugar and saturated and trans fats. Nor were biochemical parameters examined.
Nonetheless, the study is useful for generating research hypotheses and for early detection of adolescents at risk of atherosclerosis and other cardiometabolic disease. The study enabled detection and characterization of health problems in the community where it was conducted, so that community participation and the actions of health professionals can contribute to resolving them.
CONCLUSION
The high ESA prevalence we observed warns us that, to reduce incidence and prevalence of risk factors and atherosclerotic disease in Cuba, we need effective promotion and prevention actions in primary health care directed at adolescents (particularly at younger ages and applying a gender lens) and their families. A change of paradigm in cardiovascular disease prevention is needed, moving to a comprehensive approach that includes education from the earliest stages of life, involves the community and health system, and motivates physicians and other health professionals and provides tools to achieve the complex goal of lifestyle modification.