INTRODUCTION
Chronic kidney disease (CKD) is defined as structural and/or functional damage to the kidney or a glomerular filtration rate (GFR) of <60 mL/min/1.73 m2, for three months or more, irrespective of cause.[1]
CKD is currently recognized as an important global population health problem. In developed countries, the progressive increase in numbers of CKD patients and those requiring renal replacement therapy (RRT) is reaching epidemic levels, growing by 5–8% annually.[2,3] Although data are scarce for developing countries, it is estimated that by 2030, 70% of patients with end-stage renal disease (ESRD, stage 5 CKD), will be in developing countries where such growing demand will outstrip the budgetary capabilities of health care systems.[4,5]
Population-based epidemiological studies in several countries have found high CKD prevalence in its different stages, estimated at 10.0%–16.0% of the adult population.[6–14] Prevalence of chronic renal failure (CRF, stages 3–5 CKD) in the adult population is 1.4%–6.3%.[7–9,15]
The principal reported causes of CKD worldwide are diabetes mellitus (DM) (30–40%) and hypertension (HT) (25–30%), associated primarily with behavioral risk factors and aging.[2,3,15]
Recognized environmental risk factors for CKD include exposure to heavy metals (lead, cadmium, arsenic, mercury and uranium); agrochemicals; and nephrotoxic substances such as aristolochic acid, associated with Balkan endemic nephropathy, found in starfruit (Averrhoa carambola L.) and some Chinese herbal remedies.[16] Other CKD risk factors described are use of nonsteroidal anti-inflammatory drugs (NSAIDs) and the infectious diseases leptospirosis, hantavirus, leprosy and malaria (endemic in Central America). Other rare causes include heat stroke in mine workers and repeated episodes of rhabdomyolysis.[16]
In Central America and southern Mexico, an increase in CKD has been reported in the past decade. Results of epidemiological studies vary, referring to high prevalence in coastal areas in male farmers, primarily aged <60 years, who are exposed to agrochemical products in combination with presence of other risk factors.[17–20]
The 2004 Latin American Dialysis and Kidney Transplantation Registry reported incidence and prevalence of RRT at 147 and 447 per million population (pmp) respectively, and increasing. However, due to great social inequality in this region, only 5%–15% of patients needing dialysis receive it.[21,22]
In 2008, El Salvador reported 3342 patients on RRT, 715 on continuous ambulatory peritoneal dialysis, 745 on hemodialysis and 1413 on intermittent peritoneal dialysis. By then, 469 live-donor kidney transplants had been performed. In 2009, the prevalence of CRF patients on RRT was 566 pmp.[23]
CRF is an enormous population health problem in El Salvador. Nationally, it is the leading cause of hospital death reported in the adult population, the second cause of population-wide mortality in men and the fifth cause of death in persons aged >18 years. Epidemiologic knowledge is incomplete.[24] To make matters worse, there is only one nephrologist in the country for every 188,888 inhabitants, which is quite low compared to the WHO recommended guideline of one nephrologist per 50,000.[25]
The Lempa is the longest river in Central America, emptying into the Pacific Ocean. The riverbed winds through Guatemala, Honduras and El Salvador. The main rivers flowing through the cities drain into the Lempa, carrying with them liquid and solid waste from industries and urban slums.[26] In southern El Salvador, the Lempa’s banks down to its mouth are lined by communities populated by poor people who primarily work in agriculture. This region is known as the Bajo Lempa.[27]
Bajo Lempa residents perceive a high prevalence of CRF in these communities. Officials at the Ministry of Health decided to investigate and address this problem comprehensively, noting that patients from the Bajo Lempa region who begin dialysis are predominantly male agricultural workers aged <60 years who, among other factors, are exposed to agrochemicals.
Hence the design of the current study, known as Nefrolempa, aimed at delving more deeply into this serious health problem by investigating prevalence of CKD in the region, as well as its risk factors, traditional and nontraditional alike. The objectives are to identify risk factors for chronic kidney disease (CKD) and urine markers of renal and vascular damage, measure kidney function and describe the prevalence of CKD in the resident population aged ≥18 years in the Bajo Lempa region of El Salvador.
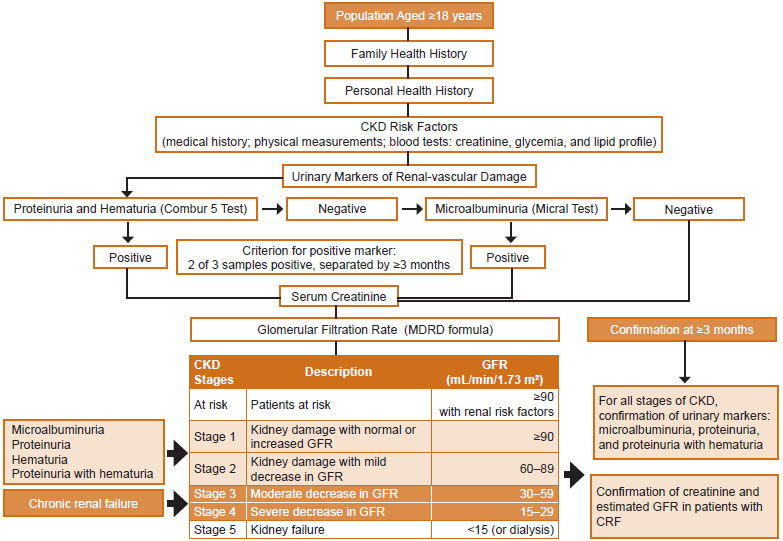
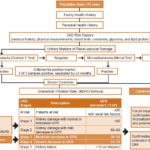
Figure 1: Nefrolempa Study CKD diagnostic algorithm
METHODS
The Nefrolempa study was conducted by a research team supported by El Salvador’s Ministry of Health and professors from the Nephrology Institute of Cuba’s Ministry of Public Health as advisors under PAHO auspices, with active participation by Salvadoran physicians and students from Cuba’s Latin American Medical School and the University of El Salvador Medical School and by the United Bajo Lempa Communities Association.
A cross-sectional descriptive and analytical study was conducted from August through December, 2009, combining epidemiological and clinical methods, involving active screening for CKD and risk factors in population aged ≥18 years resident in three rural communities in the Bajo Lempa area of Jiquilisco Municipality, El Salvador—Nueva Esperanza, Ciudad Romero and La Canoa.
The study was developed in three phases:
- Active screening for CKD risk factors and markers of renal and vascular damage and assessment of renal function in the target population;
- Three months later, confirmations of urine markers for renal and vascular damage, degree of renal function and cases of CKD and their classification by stage and association with risk factors present; and
- Clinical assessment of individual cases of CKD and proposal for a Kidney Health Unit for patient followup.
The CKD diagnosis algorithm is summarized in Figure 1.
Study universe All persons aged ≥18 years in the three communities, identified by a door-to-door population census, were eligible to participate, a total of 878 persons.
Inclusion criteria Permanent residents aged ≥18 years in the communities of Nueva Esperanza, Ciudad Romero and La Canoa, who, following informed consent, expressly agreed to participate in the study. The study included 88.3% of the enumerated population: 775 persons (343 men, 432 women).
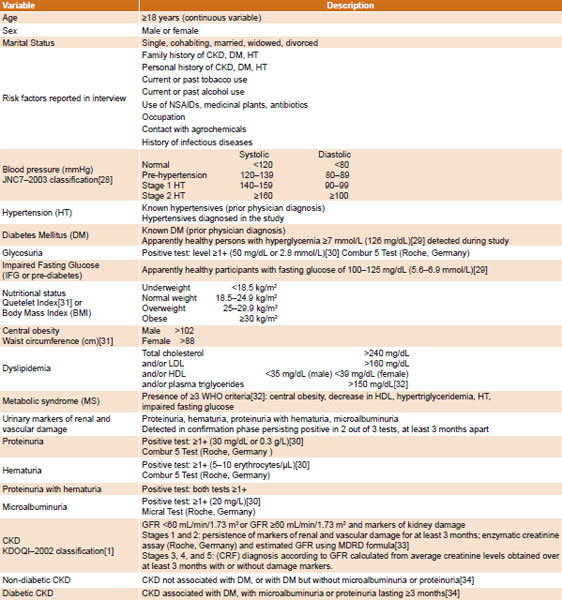
Variables studied See Table 1.
Procedures Registration and coding. Each patient was assigned a registration number and code for subsequent clinical monitoring.
Medical history and examination. These were performed to record personal clinical history (personal data; personal and family history of disease; environmental, occupational and behavioral risk factors) and physical measurements (height, weight, blood pressure, abdominal circumference).
Laboratory tests. First morning urine sample was analyzed with Combur 5 Test and Micral Test strips, and URISYS urine test strip analyzer (Roche Diagnostics, Germany). After fasting, blood was drawn for serum measurement of creatinine, glucose, cholesterol, LDL, HDL and triglycerides. Samples were processed in a clinical laboratory installed in the community equipped with a Cobas c111 spectrophotometer and its respective reagents (Roche, Germany).
Quality control, procedure standardization and data validation. All instruments and measurement tools were calibrated to ensure quality and reliability. Laboratory tests were carried out in accordance with manufacturers’ instructions using appropriate controls. Measurements and analyses were conducted by trained and certified personnel.
Ethical considerations Written informed consent was obtained from all participants. Patients agreed to publication of study results as long as their identities were protected. All patients received medical care and followup through public health services.
Data analysis Data were stored in a database developed using Epi Info 3.4 and Excel. Data were exported to SPSS 11.5 for Windows. Overall CKD and CRF prevalence rates were calculated, as well as specific prevalence rates for study variables.
Contingency tables were constructed for univariate analysis to explore CKD and CRF risk factors and eliminate those exceeding the specified significance level of p ≤0.05. As tests of independence, Bartholomew’s test and chi square for regression were used, depending on whether the independent variable was nominal, ordinal, or quantitative.
To avoid multicollinearity in the logistic regression model, associations were first assessed using the chi-square test for independence of qualitative variables, accompanied by a correlation coefficient (Phi or Cramer’s V, according to whether the tables used one degree of freedom or more than one degree of freedom, respectively). Pearson’s correlation coefficient (ρ) was used to evaluate associations for quantitative variables; a correlation greater than 0.8 was considered strong.
Next, a multiple logistic regression for binary response variables was applied. The models permitted determination of the probability of being affected by CKD or CRF in relation to risk factors present in each case and concurrent estimation of the absolute or pure influence of each factor on appearance of CKD or CRF while controlling for the others. The Enter method (which enters all variables at the same time, rather than stepwise) was used and then variables were identified whose coefficients were significantly different from 0 (p ≤0.05), using the Wald test. In addition, specific prevalence odds ratios (POR) were estimated for each variable and by intervals for each variable selected, then interpreted.
Model goodness of fit was tested using the Hosmer–Lemeshow chi-square statistic. Models were considered to fit data if probability associated with test statistic was <0.05.
RESULTS
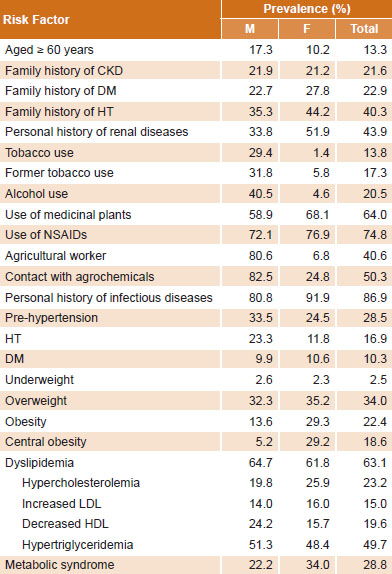
The average age of the study population was 39.2 years (39.3 years for men; 39.4 years for women). The group aged ≥60 years made up 13.3% of the study population (Table 2). Overall, 5.8% of the population had been widowed, 73% of these were women.
Family history of CKD was found in 21.6% of participants and of DM in 22.9%; 40.3% had a family history of HT (Table 2).
Personal history of renal disease was reported by 43.9% of respondents, but 40% of these cited urinary tract infections. Four men (0.6%) aged <60 years said they had CKD: one patient had a diagnosis of diabetic CKD, two had a diagnosis of hypertensive nephropathy, and one had CRF of unknown cause. Two of these patients (0.3%) were in hemodialysis.
Alcohol and tobacco use were much more common in men than in women (40.5% vs. 4.6% and 29.4% vs. 1.4%, respectively) (Table 2). NSAID and medicinal plant use were very high and higher among women (NSAIDs: 76.9% vs. 72.1% for women and men, respectively; medicinal plant use: 68.1% vs. 58.9%, respectively). The most common NSAIDs used were ibuprofen (44.5%), diclofenac (19.5%), and aspirin (3.4%). Consumption of starfruit was not reported.
Table 1: Study variables

Past infectious diseases were reported by 86.9% of participants; 62% had intestinal parasites at some time and 28.6% malaria, with no important differences observed between the sexes.
Among men, 80.6% were agricultural workers and 82.5% were exposed to agrochemicals (Table 2). Most women were homemakers; 6.8% worked in agriculture.
According to participant reports corroborated by site visits to the communities and fields, 11 agrochemical products were responsible for most direct agrochemical exposure. The most common groups were organophosphate insecticides (methyl parathion, methamidophos, phoxim), bipyridylium herbicides (paraquat: Gramoxone), and phenoxyacetic herbicides (2,4–D, hedonal). Prevalence of contact with all these was higher in men than women.
Agrochemical groups with highest male:female prevalence odds ratios for contact were bipyridylium herbicides (3.2), phenoxyacetic herbicides (3.3), organophosphates (3.8), carbamates (4.5), pyrethroids (4.6), triazines (4.7) and phosphonates (4.9).
Table 2: Prevalence of CKD risk factors in adults in Bajo Lempa, El Salvador (n=775; 343 male, 432 female)

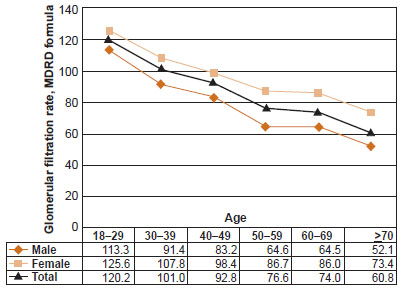
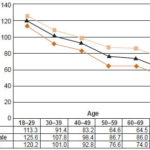
Figure 2: Average glomerular fi ltration rates by age and sex, Bajo Lempa, El Salvador (n=775; 343 male, 432 female)
HT and pre-HT were present in 56.8% of men and 36.3% of women. DM was common, but no substantial difference was observed between the sexes (9.9% and 10.6% in men and women respectively). High prevalence of overweight and obesity was registered, though more common in women (64.5% vs. 45.9% in men). Almost two thirds (63.1%) of participants had dyslipidemia; men more commonly exhibited a pattern of hypertriglyceridemia with low HDL, while women more commonly had hypercholesterolemia with increased LDL. Metabolic syndrome was more common in women (Table 2).
Markers of renal and vascular damage were found in 15.8% of the study population, more often in men than women (22.6% vs.10.6%, respectively); microalbuminuria the most common marker (6.3%). GFR showed a proportional decline with increasing age, and was lower in men in all age groups. In persons aged 18–60 years, decrease in GFR by decade of life was greater in men than women. In the 50–59 year age group, average GFR in men was 22 mL/min/1.73 m2 less than in women, and was close to the cutoff for chronic renal failure (Figure 2).
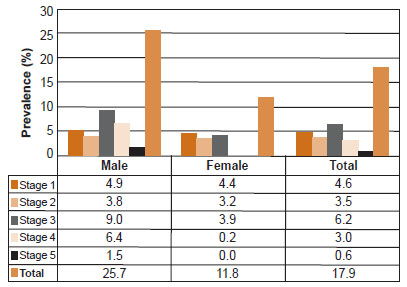
The study population showed high CKD prevalence: 17.9% (139/775 persons). One in four men had CKD (25.7%, 88/343), more than double the prevalence in women (11.8%,(51/432). Overall prevalence of CRF was 9.8% (76/775), with 16.9% (58/343) in men and 4.2% (18/432) in women, for a male:female prevalence ratio of 4:1 (Figure 3). No positive markers of renovascular damage were found in 3.1% of men and 1.1% of women with CRF.
Of all participants with CKD (139 persons), 62.6% (87) were aged 18–59 years and 37.4% (52) were aged ≥60 years. Age group prevalence analysis (n=775) revealed a prevalence of 30% in persons aged 18–59 years (n=672) and 50.5% in persons aged ≥60 years (n=103).
The community of Ciudad Romero had the highest prevalence of CKD (20.7%), followed by Nueva Esperanza (16.4%) and La Canoa (14.9%).
Figure 3: CKD prevalence by stage and sex, Bajo Lempa, El Salvador (n=775; 343 male, 432 female)
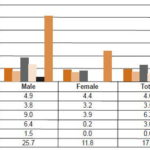
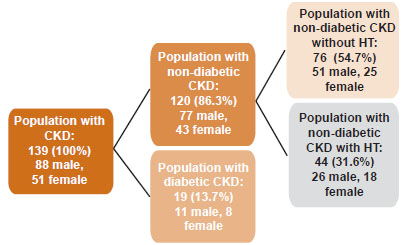
Figure 4: Distribution of CKD etiology, Bajo Lempa, El Salvador (n=139; 88 male, 51 female)
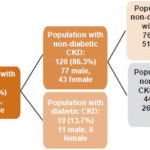
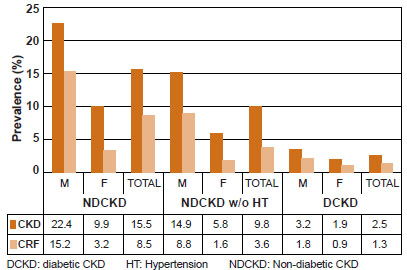
Figure 5: Prevalence of CKD and CRF by etiology and sex, Bajo Lempa, El Salvador (n=775; 343 male, 432 female)
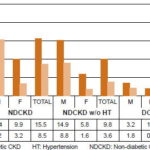
DCKD: diabetic CKD HT: Hypertension NDCKD: Non-diabetic CKD
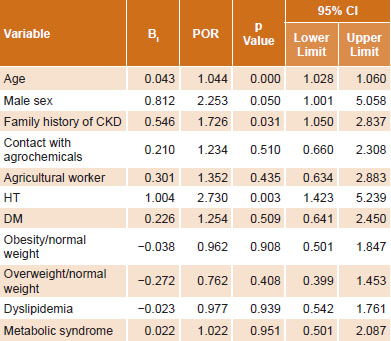
Table 3: Multiple logistic regression for CKD and its risk factors in adults in Bajo Lempa, El Salvador (n=775; 343 male, 432 female)

Constant −4.385; Bi: Coeffi cient POR: Prevalence Odds Ratio
To obtain more evidence on the differences found, it was decided to classify the CKD population by etiology: diabetic CKD and nondiabetic CKD. Of all those with CKD, 86.3% (120/139) were classified as non-diabetic CKD and 13.7% as diabetic CKD (19/139), for a 6:1 ratio. Among non-diabetic CKD persons, hypertensive patients were excluded to rule out a vascular hypertensive etiology; 54.7% (76/139) had neither DM nor HT (Figure 4).
For all presentations of CKD—with or without DM, with or without HT—men predominated (Figures 4 and 5).
In univariate analysis, HT, male sex, family history of CKD, increased age, DM, metabolic syndrome, dyslipidemia, agrochemical exposure, agricultural occupation, obesity and overweight were all significantly associated with presence of CKD. The remaining factors studied that did not show significant association were excluded from subsequent multivariate analysis.
The logistic model revealed that the probability of developing CKD was significantly influenced by male sex, increasing age, HT and family history of CKD. The remaining variables did not show statistical significance. The POR for CKD in men compared to women was 2.253 (95% CI 1.001–5.058); starting at 18 years of age, the risk of CKD increases 1.044 times (95% CI 1.028–1.06) per year of age; having a family member with CKD increases the risk by 1.726 times (95% CI 1.05–2.837); and personal history of HT almost triples the risk of developing the disease (POR 2.73, 95% CI 1.423–5.239) (Table 3).
DISCUSSION
The sociodemographic characteristics of the study communities in Bajo Lempa are consistent with the general characteristics of rural El Salvador: a relatively young, farming population, where agriculture is the primary occupation.[27,35] A striking social trait in the study population is the high rate of widowhood among women, explained by earlier male mortality.
Embedded in the social determinants of health typical of these farming communities are many risk factors for CKD: high prevalence of family history of CKD, DM and HT, suggesting heightened genetic susceptibility to these conditions or predisposing environmental factors; high frequency of infectious diseases, including malaria, affecting the kidney; and nephrotoxicity from frequent use of NSAIDs.[16] All these factors are common to both sexes. No known nephrotoxic plants were identified in herbal medicines used. Prevalence of current and former tobacco use in men was close to that found in a study in a rural Mexico.[36] Prevalence of alcohol use in men in our study was high. In Nicaragua, there is an as yet unproven hypothesis linking CKD with a kind of homemade rum known as lija, due to the high prevalence of its use by men.[37]
The results show a clear vulnerability in the study area to an increased risk in individuals, families and communities to the development, progression and complications of CKD. This is consistent with results from a study in the United Kingdom of the relationship between low socioeconomic status and gravity of CKD in 1657 patients. It showed that patients with a lower economic status were at greater risk for decreased GFR, adjusting for other sociodemographic, behavioral and clinical variables.[38]
Participants presented prevalences of family history of CKD, DM and HT similar to various published studies. For example, in Asia, the KEEP-Japan study[14] reported general population prevalences of these of 19.2%, 32.7% and 58.7%, respectively. In Latin America, the KEEP-Mexico and KEEP-Jalisco studies[12] report a population prevalence of family history of CKD and DM and HT together of 52% and 23% respectively.
We found population prevalence of DM greater than that reported in most studies in other countries: KEEP-USA, 7%;[11] NHANES-USA 1999–2004, 10.3%;[7] EPIRCE-Spain, 9.2%;[9] ISYS-Cuba, 5.4%;[15] and Mexico’s National Health Survey, 8.0%.[39]
HT prevalence found in this study was lower or similar to that reported in other recent studies: NHANES-USA 1999–2004, 29%;[7] EPIRCE-Spain, 24.1%;[9] ISYS-Cuba, 30%;[15] and ENSA-Mexico, with 31%.[39] In earlier studies in Mexico, HT prevalence ranged from 7.7% to 10%.[36]
Overweight and obesity were highly prevalent in the study population, particularly obesity in women, with rates similar to those reported internationally.[7,9,11,15,39] Obesity is associated with vascular and renal damage, pointing to the need for prevention. Obesity is present in 90% of type 2 diabetics and 65–75% of hypertensives; DM and HT are the two leading causes of CKD globally.[40]
Hypertriglyceridemia and low HDL, were more frequent in men—a pattern characteristic of CKD—while hypercholesterolemia and increased LDL were preponderant in women. Similar results were found in an urban area of the Salvadoran capital[41] and in the EPIRCE-Spain study.[9]
Metabolic syndrome (MS) prevalence was high, and more common among females. MS was more prevalent than in a study carried out in urban San Salvador using the same diagnostic criteria, which revealed 22.7% for both sexes.[41] It has been reported that as the presence of MS increases, the possibility of microalbuminuria and of cardiovascular mortality from any cause also increase.[42,43] The Atherosclerosis Risk in Communities (ARIC) Study also found MS conferred increased risk of CKD and CRF (RR for the latter 1.24).[43]
Men led in traditional risk factors for vascular and renal damage—HT, hypertriglyceridemia and low HDL cholesterol, and smoking—as well as other, nontraditional risk factors, such as agricultural workers’ unprotected exposure to agrochemicals—some of which are highly toxic and/or banned—and alcohol consumption.
During community visits and interviews with local opinion leaders, researchers became aware of aerial crop dusting during the past decade—still practiced in one farming area in the community of Ciudad Romero, with agrochemicals landing on homes as well as crops, and up to eight different products used on each field without proper protective measures. Researchers also observed that conditions for storage, handling and sale of these products were inadequate and lacked proper biosafety measures. In such circumstances, organic and inorganic environmental contamination is quite possible. A 2007–2008 study of pesticide contamination in the Bajo Lempa region detected dieldrin—a pesticide used in growing cotton until banned for agricultural use in 1986—in shrimp ponds in concentrations of 0.085–0.182 ng/mL, 1.5 times higher than the United States’ EPA limits.[44]. Six of ten pesticides evaluated in the study were found in the bottom of the shrimp ponds: heptaclor, endrin, dieldrin, DDT and DDT metabolites DDD (dichlorodiphenyldichloroethane) and DDE, which are persistent and strongly adherent to soil.[44]
In Nicaragua, increased CKD rates in male farmers aged <60 years were found to be associated with pesticide exposure, dehydration, alcohol consumption, exposure to heavy metals and residence at lower altitudes.[37] Studies in Sri Lanka have found an association between bipyridylium (paraquat and diquat) and organophosphate poisoning with repeated episodes of acute renal failure.[45]
In Guanacaste department, Costa Rica, CKD—a chronic interstitial nephritis—has been increasing over the past ten years among male sugarcane farmers aged 20–40 years, but this phenomenon has not been investigated epidemiologically.[46]
Men were twice as likely as women to have urine markers of renal and vascular damage. The pattern of microalbuminuria predominance and relatively little proteinuria supports the possibility of tubulointerstitial damage rather than glomerular etiology.
There are no important sex differences in renal physiology,[47] but in all age groups in this population GFR was lower in men than in women. The GFR curve showed that absolute loss of renal function was greater in men than in women; that this functional decline began in youth; that loss of renal function with age was greater in men; and that men reached the renal failure earlier than women.
Screening the entire adult study population using a combination of markers of renal damage and GFR revealed hidden CKD morbidity and CKD prevalence in both sexes to be greater than the average rates commonly reported in the international literature.[6–14] It also found that in this population, CKD was twice as common in men and four times as many men as women had CRF. Four people self-reported CRF at the beginning of the study; screening revealed 76.
Reports on the CKD pandemic emphasize increased numbers of cases with population aging because risk increases with age.[3] In this study population, the greatest number of cases were found in persons aged <60 years, although the rate in those aged ≥60 years was highest, due to the accumulation of multiple risk factors related to the aging process.
In our study, multiple logistic regression did not find a statistically significant association with DM, contrary to the KEEP-Japan study, which reported a statistically significant OR of 1.71 for DM for CKD.[14] KEEP-Japan also reported an OR for HT of 3.42, very similar to that found in the Bajo Lempa study population.
HT prevalence is higher in CKD patients and increases in a linear fashion as GFR decreases; HT is a risk factor for cardiovascular morbidity and mortality and a factor in the progression of CKD.[48] Although HT is strongly associated with CKD, the cross-sectional design of this study precludes establishing temporal precedence, a limitation for interpreting results. The study’s finding that HT was more prevalent in advanced stages of CKD than in initial stages can be explained by the effects of CKD on HT. Some 80–85% of CKD patients develop HT, and HT prevalence increases with the severity of CKD.[48]
Factors associated with CKD, according to the logistic model, were male sex, age as a continuous variable starting at 18 years, HT and family history of CKD. It should be noted that HT is not only a cause of CKD but also a consequence of it and that it is the condition most frequently associated with CKD. The logistic model did not find an association with agrochemicals, as observed in univariate analysis, possibly because the majority of men were exposed to agrochemicals.
In the majority of CKD cases, the etiology was neither DM nor HT, although these two conditions were present as causal factors in a small proportion of cases and as factors for comorbidity and progression of CKD in cases where etiology was not specified originally. Most cases of CKD were of unknown etiology. These results and findings from other research in El Salvador[17–19] suggest we may be seeing a new nosological entity, one that behaves as a “nephropathy of Salvadoran agricultural communities.” Given the unspecified etiology of CKD in this study and cumulative evidence of toxic environmental factors, the hypothesis of environmental toxicity should be investigated in depth.
Reports of elevated prevalence of CKD of unspecified cause in male farmers in various countries of Central America and in southern Mexico[17–20,37,46] could even suggest a hypothesis of the existence of a “Central American or Mesoamerican Regional Nephropathy.”
Among the limitations of this study, it should be noted that although the equation for estimating renal function (MDRD formula) is the most widely used in epidemiological studies,[7] it underestimates renal function in young adults and overestimates it above 60 mL/min per 1.73 m2 of body surface area in elderly patients, which should be taken into account when analyzing results obtained for the different age groups. The equation was designed for the white and Afro-American population of the United States; it should therefore be validated in the Salvadoran population for greater reliability, or a new formula should be developed for estimating renal function in our region.
Nevertheless, the study design is useful for generating research hypotheses, estimating prevalences in the study population, and identifying possible risk factors. Its flexibility for exploring associations among multiple exposures and effects compensates for its limitations in assessing causality.
Finally, the information obtained has been useful in planning for meeting the health care needs of the population affected. It provided the basis for El Salvador Ministry of Health´s development of a Renal Health Unit in the Bajo Lempa region, comprised of a multidisciplinary team to deliver preventive and curative care, providing continuity to the work in the rest of the study area and facilitating new screening and health interventions in other rural Salvadoran communities.
CONCLUSIONS
In this study population, chronic kidney disease and its chronic renal failure phases had a higher prevalence and a distinct epidemiological and clinical pattern from that reported internationally. The disease predominated in agricultural workers exposed to nontraditional (occupational and toxic factors) and traditional risk factors (DM, HT, obesity and dyslipidemia) for CKD that may act synergistically. Significant association was found with male sex, HT, family history of CKD and early onset of renal function decline. Most cases of CKD were associated neither with DM nor with HT; nor did markers indicate glomerular disease. Etiology therefore remains unknown, but the hypothesis of nephrotoxic environmental factors cannot be ruled out.
Elevated prevalence of risk factors examined suggests a possible double burden of causal and progression factors, both nontraditional and traditional.
The results of this study and others by Salvadoran nephrologists suggest a new nosological entity, still not well understood, that could be termed a Salvadoran agricultural nephropathy. Similarities with reports from other Central American countries and southern Mexico could suggest a Central American or Mesoamerican regional nephropathy. Further epidemiological, clinical and toxicological studies are needed to corroborate these hypotheses.