INTRODUCTION
Article 50 of Cuba’s Constitution states that all Cubans have the right to health protection and care, and that the State is responsible for ensuring this right.[1] The Ministry of Public Health (MINSAP) is mandated to manage, implement and monitor national public health policies, including management of the National Health System (NHS).[2] NHS’s guiding principles are: medical services are government-financed and delivered in public facilities at all levels; access is universal and free of charge; standards are centralized, while operations are decentralized; a preventive approach is built upon strong primary health care; scientific and technological advances are applied appropriately; and key components include community and intersectoral participation, as well as international collaboration.[2]
This essay addresses intersectoral action for health using the example of cervical cancer, which is a health problem in Latin America and the Caribbean, including Cuba, and indeed worldwide. It describes joint efforts by public health and the domestic biotechnology industry to reduce invasive cervical cancer incidence and mortality rates.
INTERSECTORAL ACTION
Intersectoral action constitutes a coordinated process whereby strengths, knowledge and resources from various sectors are combined to understand and solve complex issues. It brings to bear the different sectors’ knowledge and experience in planning, implementing and assessing interventions, with the aim of achieving integrated results with a synergistic impact on social development.[3] Intersectoral action facilitates promotion and achievement of common goals in various areas: policy, research, training, operations and financing.[4] Such collaboration encompasses a horizontal dimension, linking different sectors at a given level (e.g., community-level health, education, sports and civil society organizations) and a vertical dimension linking different levels within a given sector (e.g., health promotion at national, provincial and municipal levels). The key to success is to work in both dimensions.[4]
In this paper, intersectoral action for health is understood as the coordinated intervention of institutions representing more than one social sector in activities designed, either fully or in part, to address problems related to health, well-being and quality of life. It is an important component of an organized social response. Fundamentally, this means transforming chance or occasional cooperation into actions that, led by the health sector and supported by well-coordinated national and local policies, are strategically geared to address priority issues where other sectors’ actions can play a decisive role.[5] In this case, cervical cancer is the health problem and biotechnology is the partner sector. Although biotechnology is part of the health sector broadly defined, it is not part of the NHS, and in many countries, population health is not its primary motivating factor. Thus, this example of intersectoral collaboration geared to public health objectives merits examination.
CERVICAL CANCER
In 2012 (latest available data), 265,672 women worldwide died from cervical cancer (6.8 per 100,000), the fourth most common cancer in women. The incidence rate was 14 per 100,000 women (527,624).[6] The same year, cervical cancer killed 28,565 women in Latin America and the Caribbean (8.7 per 100,000), ranking second as a cause of cancer death in women; the incidence rate was 21.2 per 100,000 women (68,818).[6]
In 2014 in Cuba, cervical cancer was the sixth most common cause of cancer death in women, with 471 deaths and a crude mortality rate of 7.9 per 100,000 women. The age-adjusted incidence rate in 2011 (latest published) was 20.1 per 100,000 women,[7] similar to that of the Latin American and Caribbean region. In 2014, 798,159 cuban women aged ≥25 years had screening cytology, resulting in diagnosis of 1461 positive cases of cervical cancer (0.2% of women screened). Of these, 60% were diagnosed with clinical stage 0; 20.3% with stage I; 13.9% with stage II; 4.6% with stage III; and 1.2% with stage IV.[7]
Improving early diagnosis through screening the asymptomatic population promotes appropriate treatment and helps reduce mortality.[8] According to WHO, a good cervical cancer screening program should have broad coverage (80%–100%) of women at risk (i.e., who had ever had heterosexual intercourse), routinely tested every three years.[9] In 2009–2011, the Cuban cervical cancer control program’s screening coverage was still below this threshold, at 67%.[10]
CONFRONTING CERVICAL CANCER: HEALTH AND BIOTECH SECTORS IN CUBA
After initial investments in biotechnology in the early 1980s, Havana’s Scientific Pole was created in 1992 to integrate scientific results—from research through marketing—in the spheres of medicine and its specialties, pharmaceuticals and agroindustry in general.[11] This further facilitated biotechnology development and offered an outlet for its productive capacities. Besides linking scientific research to production, or advancing knowledge sharing, its creation fostered interdisciplinary participation and formation of networks of cooperation.[11] The Pole eventually clustered 50 institutions, including regional branches in 12 of Cuba’s 15 provinces (15 since 2010; formerly, 14).[12]
At the close of 2012, the health-related biotechnology centers joined the BioCubaFarma Business Group, created through the merger of biotechnology and pharmaceutical manufacturers.[13] All companies operate in a closed loop that covers research, development, production, marketing and technical support to customers.[12,14,15]
Since its creation, Havana’s Scientific Pole has had a close working relationship with MINSAP. Biotechnology provides the health sector over 160 products, including biopharmaceuticals, diagnostic kits, drugs, and therapeutic and preventive vaccines, all produced by the professionals working in this industry.[12,15] A member of this group is the Immunoassay Center (CIE), the Cuban biotechnology facility responsible for developing diagnostic testing systems, including equipment, reagents and software programs.[13,15]
Since the early 1960s, cancer has been a health priority for Cuba. The National Cancer Registry was created in 1964 and has been managed by the National Oncology and Radiobiology Institute (INOR) since the latter’s creation in 1966. In 1969, the National Cancer Control Program was created, and is still evolving. Cuba’s Comprehensive Cancer Control Program was implemented in 2007, and in 2011 the National Cancer Control Unit (UNCC) became the Independent Cancer Control Section (SICC).[16,17]
In the early 2000s, relations between MINSAP and the biotechnology sector were formalized with creation of the Cancer–Scientific Pole Working Group, whose main objectives were to address cancer comprehensively as a health problem and determine specific actions that biotechnology should undertake, e.g., provision of diagnostic systems, drugs and medical equipment. This group has been operating as the Cancer–BioCubaFarma Group since 2012. It continues to hold monthly meetings to propose and assess strategies, manage actions and optimize biotechnology and pharmaceutical resources for cancer control. The group holds methodological meetings and national workshops as forums for training, evaluation and exchange between the biotech industry and the NHS.[17]
Cervical cancer screening in Cuba is done by periodic Pap smears in the asymptomatic population.[16,17] There is strong evidence that treatment of noninvasive lesions found by Pap smear screening is highly successful. In particular, early diagnosis associated with proper therapy and routine followup can be quite effective in reducing invasive cervical cancer incidence rates and mortality.[16–18] Since 1997, routine screening is done in a primary care setting every three years for women aged 25–64 years,[16] according to WHO recommendation for both procedures and periodicity.[9]
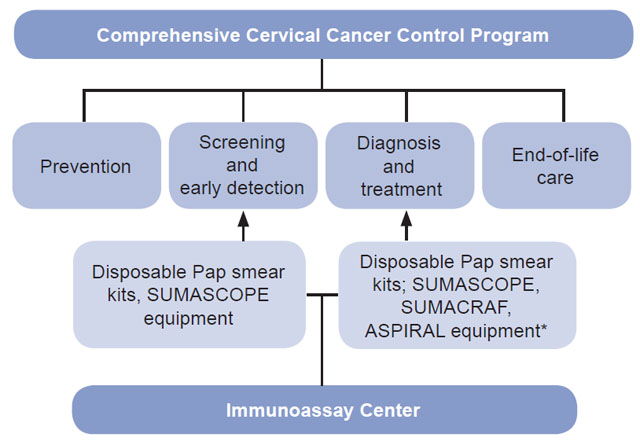
In 2009, MINSAP’s UNCC requested technological support from CIE for cervical cancer control. As a result, CIE’s technologies have been instrumental in reinforcing various cervical cancer control measures such as screening, early detection and diagnosis (Figure 1).[19]
Figure 1: Immunoassay Center contributions to cervical cancer control in Cuba
*Tecnosuma Internacional S.A.[19]
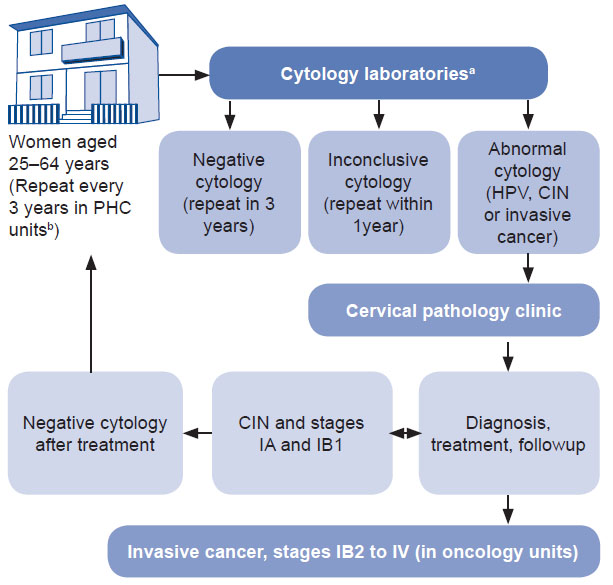
Since 2010, CIE has supplied the NHS with disposable Technosuma S.A. Pap smear test kits, including fixative spray for cytology specimen collection. The kits are provided at low cost and include specula (small, medium and large), slides, slide holder, Ayre spatula, swab, applicators and a pouch. Samples collected are sent to cytology labs at the secondary care level for processing. Women with abnormal Pap smear results are referred to cervical pathology clinics at this level of care (Figure 2).
Figure 2: Cervical cancer screening and diagnosis algorithm

aResults are always sent to health facilities and reported to patients
bFamily medicine, community polyclinics and rural hospitals
CIN: cervical intraepithelial neoplasia HPV: human papillomavirus
PHC: primary health care
Table 1: SUMASCOPE video colposcopes in primary care centers treating benign cervical lesions (Cuba 2015)

*Special Municipality
There are 45 such clinics throughout the country, providing coverage to all community-based polyclinic catchment areas.[16] Each is equipped with a video colposcope (SUMASCOPE), electrocautery (SUMACRAF) and a smoke aspirator (ASPIRAL) (Table 1), all produced by CIE and supplied through its commercial branch, Tecnosuma Internacional S.A.[19] Disposable parts were also designed to enable these clinics to perform colposcopy and electrocautery (for which the ASPIRAL smoke aspirator is attached to the SUMACRAF speculum to suction smoke during electrocautery).
We infer from the foregoing that biotechnology support to MINSAP has been instrumental in increasing the number of Pap smears among the healthy or asymptomatic population. Availability of the Pap smear kits, in particular, may have contributed to greater coverage of this screening program: for instance, 199,780 more tests were done in 2014 than in 2009 (before CIE products were available), amounting to a 25% increase.[7] To put this in the context of coverage, an estimated 65.3% of women aged 25–64 years were screened in 2006–2008; by 2012–2014, the figure was 71.8%.[20,21] Clearly, other factors besides the introduction of CIE products affect screening coverage.
In addition, having the right equipment available at the right time, as permitted by CIE technologies, enables early diagnosis and timely treatment of both premalignant lesions and malignant neoplasms. Such early treatment is less complex, less costly, and leaves fewer sequelae or serious and irreversible events in women with advanced cancer.[18] Assessment of the CIE kits’ impact on reducing invasive cervical incidence and mortality rates is still in process, and the lack of available data thus far constitutes a limitation of this paper. Such evaluation is necessarily an important topic for further research.
Looking ahead, another action under way to reinforce the intersectoral strategy to fight cervical cancer is installation of SUMASCOPE equipment in all Cuban 168 municipalities to provide access to colposcopy for any woman with other cervical lesions. This approach should increase early diagnosis of cervical cancer, as well as diagnosis and treatment of other, benign conditions (cervical ectopy, ectropion, erosion, cervicitis). Installation of SUMASCOPE in municipalities is 80.6% complete (141/175 planned; particularly populous municipalities need more than one colposcopy service) (Table 1). CIE is currently developing a system for detecting infection with HPV types 16 and 18, in order to increase diagnosis specificity.
CONCLUSIONS
Intersectoral action by the CIE and NHS to introduce use of new, domestically-produced technologies for early diagnosis of premalignant and malignant cervical cancer lesions has been ongoing since 2010. Availability of the technology at various levels of the health system since then should be the focus of further research, as well as assessment of the organization and application of national cervical cancer screening programs, in order to determine their impact on cervical cancer incidence and mortality trends, as Cuba continues to reach for the 80% screening uptake recommended by the WHO and to step up efforts to reduce both incidence and mortality.
This collaboration is an example of intersectoral action in public health for identifying and solving health problems affecting people’s well-being and quality of life.