The emerging SARS-CoV-2, a novel human coronavirus, caused the COVID-19 pandemic, with more than 9.5 million cases and 484 000 known fatalities to date (June 24th, 2020). In several regions, healthcare systems have collapsed whereas interventions applied to slow the viral spreading have had major social and economic impacts. After China, Europe, and the United States, Latin America has emerged as the new epicenter of the pandemic. By late-June, the region accounted for roughly 50% of global daily deaths (Gardner, 2020). The evolution of the COVID-19 pandemic in the region has been heterogenous as several countries are currently experiencing exponential growth of their daily cases and fatalities, while others have successfully controlled their corresponding outbreaks. Cuba confirmed its first COVID-19 cases in mid-March. After a three-month outbreak, the country recently began to move to a postepidemic phase. This dispatch details some relevant aspects of the strategy deployed in Cuba to face the COVID-19 pandemic and to decrease the impact of this emerging disease in the country. In addition, it describes the evolution of some epidemiological variables which allowed the country to de-escalate some of the non-pharmaceutical interventions applied during the outbreak.
Doctors and pedestrian wearing face masks in Havana, Cuba during the COVID-19 pandemic.
ABSTRACT The emerging SARS-CoV-2, a novel human coronavirus, caused the COVID-19 pandemic, with more than 9.5 million cases and 484 000 known fatalities to date (June 24th, 2020). In several regions, healthcare systems have collapsed whereas interventions applied to slow the viral spreading have had major social and economic impacts. After China, Europe, and the United States, Latin America has emerged as the new epicenter of the pandemic. By late-June, the region accounted for roughly 50% of global daily deaths (Gardner, 2020). The evolution of the COVID-19 pandemic in the region has been heterogenous as several countries are currently experiencing exponential growth of their daily cases and fatalities, while others have successfully controlled their corresponding outbreaks. Cuba confirmed its first COVID-19 cases in mid-March. After a three-month outbreak, the country recently began to move to a post-epidemic phase. This dispatch details some relevant aspects of the strategy deployed in Cuba to face the COVID-19 pandemic and to decrease the impact of this emerging disease in the country. In addition, it describes the evolution of some epidemiological variables which allowed the country to de-escalate some of the non-pharmaceutical interventions applied during the outbreak.
1. COVID-19 in Latin America and the Caribbean: early projections and current situation Early modelling studies suggested that, without the adoption of mitigation/suppression measures to reduce SARS-CoV-2 transmission, by the end of 2020 the COVID-19 pandemic would result in more than 7 billion infections and 4 million deaths (Walker et al., 2020). Under an unmitigated scenario, the study projected more than 566 million cases and 3.1 million deaths for Latin America and the Caribbean. Non-pharmaceutical interventions and policies aimed at controlling the virus’ spread include, among others, stay-at-home requirements, social distancing, school closures, bans on gatherings and public events, quarantines, and, in some cases, complete lockdowns. These interventions were commonly combined with travel bans aimed at diminishing the chances that the virus could seed from imported cases. Following the recommendations of several world renowned epidemiologists and the WHO, the European and Asian countries that were the initial epicenters of the pandemic combined several of these strategies to flatten the curve of infections and avoid overwhelming their hospitals and health care systems (Flaxman et al., 2020).
The COVID-19 pandemic has been particularly challenging for Latin America and the Caribbean. Several countries in the region lack strong public healthcare systems and sanitary infrastructures, have a significantly low ratio of medical doctors and hospital beds per million of inhabitants, and face the health crisis created by the emerging virus with limited diagnostic capacity as compared to some Asian and European countries, or the United States. Significant levels of informal employment and the economic difficulties faced by several countries in the region conspire against governments’ ability to offer financial stimulus and income support, hampering the implementation of stay-at-home restrictions and social distancing policies. Currently, Latin America and the Caribbean is the region with the highest levels of daily cases and COVID-19-related deaths.
At the time of writing, the region accounts for more than 2.2 million COVID-19 confirmed cases and over 103,000 fatalities (WHO, 2020). Brazil, Mexico, Chile, Peru, and Colombia are among the twelve countries with the highest numbers of daily confirmed cases and fatalities in the last weeks of June (updated June 24th) (WHO, 2020). These numbers are likely undercounted as most Latin American and Caribbean countries show remarkably low testing rates, significantly hampering their national response to the pandemic. Indeed, several independent studies have signaled a potential major under-reporting of death tolls, as fatalities in several territories and cities are far above of historical averages, even after taking into account the reported COVID-19-related fatalities (Burn-Murdoch, 2020).
2. Cuba before the national outbreak Early data from China’s epidemic showed that COVID-19 has a case fatality rate of around 5.9% among elderly people (>60 years old) (Zhang, 2020). Further studies, including data from Italy, have confirmed the high case fatality rate among patients aged 60 years or older (Onder et al., 2020). Cuba is one of the countries with the highest life expectancy in the region (78.5 years) (MINSAP, 2019) and a major proportion of its population (20.23%) is included in the age group of people who are at higher risk if they get infected by the novel coronavirus. According to official data, the country also has a significant prevalence of diabetes mellitus (64.3/1000 inhabitants) and arterial hypertension (almost one fourth of the population), both identified as risk factors early on (Zhang, 2020). This data, combined with the challenges associated to economic problems and the fact that Cuban economy is highly reliant on tourism, prompted the Cuban political and public health authorities to design a coordinated national strategy to reduce the impact of the emerging virus on the island.
In the context of the Cuban response to the COVID-19 pandemic, it is important to note certain pre-existing conditions that benefitted the implementation of the national strategy. These include universal healthcare, the highest per capita of medical doctors/millions of inhabitants worldwide, a wellstructured primary healthcare system, and a previous history of facing emergency situations during the annual hurricane season (Morris and Kelman, 2020). Also—in the context of the response to the pandemic—the existence of a statecontrolled economy and public health policies expedited the mobilization of emergency resources and facilitated the rapid isolation of confirmed cases as well as their contacts. It is not the focus of this text to assess the impact of some of the measures implemented in the country (i.e. evacuation to isolation centers, mandatory use of face masks in public places) on individual rights. As a virologist, I will describe these measures’ role in controlling the national epidemic and detail some epidemiological data that show the positive outcome of the strategy applied in Cuba.
In the absence of herd immunity, highly efficient antiviral treatment or complementary therapies, or a vaccine, the early application of nonpharmaceutical interventions as well as other epidemiological tools represents the gold standard to face the COVID-19 pandemic. It is important to note that since there is to date no “silver bullet” to stop the spread of the novel coronavirus, several poli cies must be implemented simultaneously. Cuba started to prepare its national response in late January. The Plan for Prevention and Control of the disease included, among other aspects, the training of the healthcare workers, reinforcement of the National Program for the Surveillance of Acute Respiratory Infections (ARI), and—of particular importance—the preparation and further extension of laboratory infrastructure and facilities for the molecular diagnostic of SARS-CoV-2 infections. On March 11 (coincidentally the same day that the WHO officially declared COVID-19 a pandemic), Cuba confirmed the first cases of its outbreak.
3. The Cuban strategy and its major tools At the discretion of this author, the Cuban approach to cope with viral spread and to control its epidemic has four major virtues. These are, (i) early, or at least timely, application of mitigation/suppression measures, (ii) massive and reinforced ARI surveillance enabling early detection of suspected cases, (iii) comprehensive contact tracing with rapid isolation of confirmed cases and contacts, and (iv) the development of a rational testing program. In this section, the individual contribution of some of these tools will be briefly discussed.
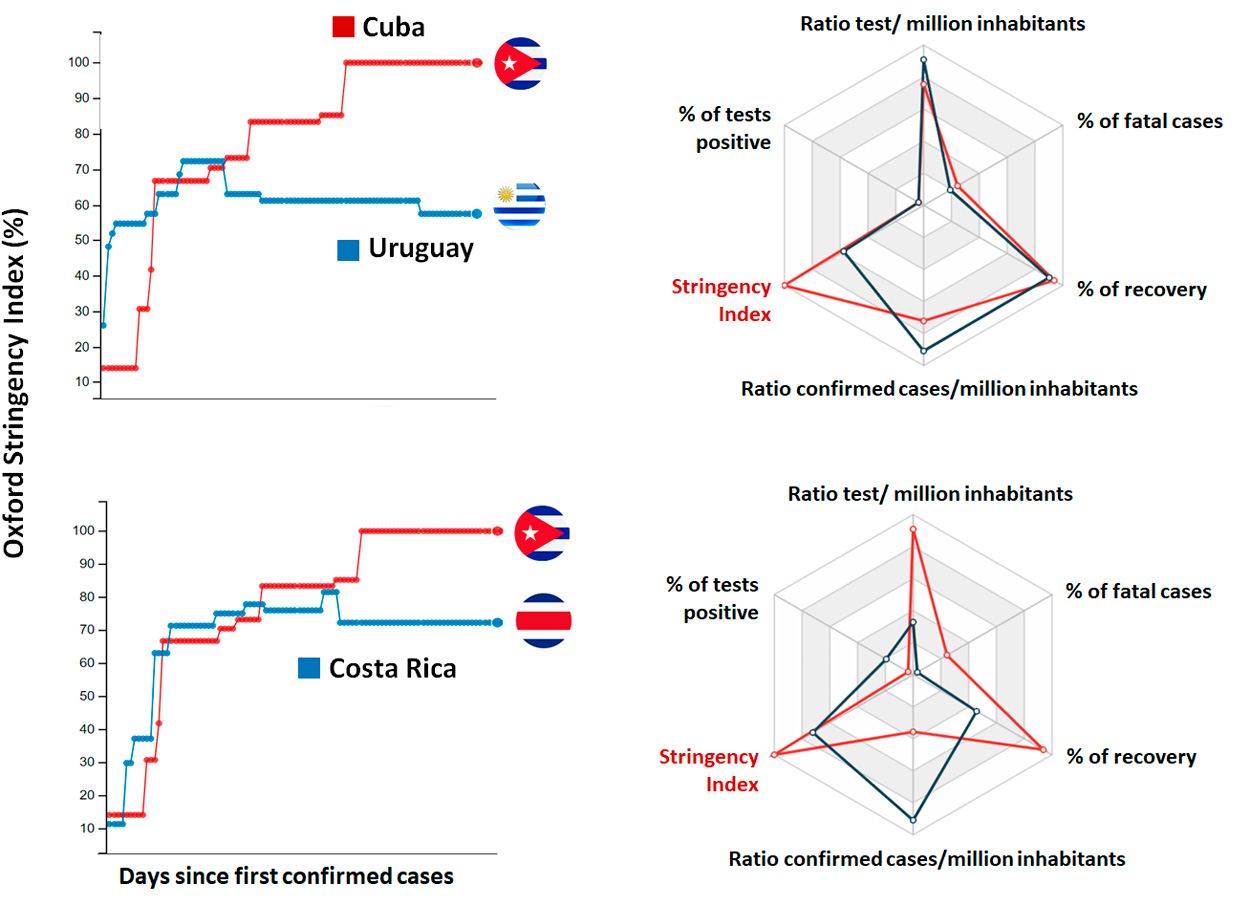
The course and strength of the non-pharmaceutical interventions implemented by each country can be ranged using the Oxford Stringency Index (Hale et al., 2020). Higher values (%) imply strongest mitigation/suppression measures. An analysis of the Index shows a similar temporal pattern for Cuba, Uruguay, and Costa Rica (Figure 1), which represent some of the Latin American countries that have controlled their initial corresponding outbreaks. Among the measures applied by Cuba were a partial travel ban (22.03.2020, 48 confirmed cases and one fatality), and then a complete international travel ban (01.04.2020)–to prevent viral seeding–, the closure of schools Figure 1. Graph representing the Oxford Stringency Index for Cuba as compared to Costa Rica and Uruguay. [Modified with permission from (COVID19 Cuba Data Dashboard, 2020)]. (24.03.2020, 40 cases, one fatality) and public transportation, restriction of internal movement, public events, and gatherings, as well as selective quarantines or restrictive home isolation in territories with community transmission. Also important is the fact that Cuba mandated the use of face masks in public places as a key tool to reduce transmission (Prather et al., 2020). Similar to Uruguay and Costa Rica, most policies applied in Cuba were implemented in the early phase of the epidemic, thus increasing the probability of a positive outcome. At present, some of the interventions remain active in the island.
Figure 1. Graph representing the Oxford Stringency Index for Cuba as compared to Costa Rica and Uruguay. [Modif ed with permission from (COVID19 Cuba Data Dashboard, 2020)].
3.1 Massive surveillance and contact tracing Relying on its broad primary health care system and the collaboration of undergraduate medical students, the country deployed a “door-to-door” surveillance of ARI to identify suspected cases and immediately assess whether to recommend home isolation (Acosta and Marsh, 2020; Miranda, 2020). This massive program for the detection of patients with COVID-19-like clinical symptoms, deployed in the pre-pandemic days and particularly during the early phase of the outbreak in Cuba, represented a key tool to control the spread of the virus. According to official data, by March 22nd (40 confirmed cases in total), the Cuban primary health care system was monitoring over 37,000 persons (MINSAP, 2020). The early identified suspected cases that fulfilled epidemiological criteria such as contact with people who had recently travelled to the island from abroad or with confirmed cases, were immediately evacuated to isolation centers and underwent molecular diagnostics. Meanwhile, confirmed cases were hospitalized and treated according to their clinical manifestations. The unique approach significantly reduced the spread of the virus in the early phase of the Cuban epidemic.
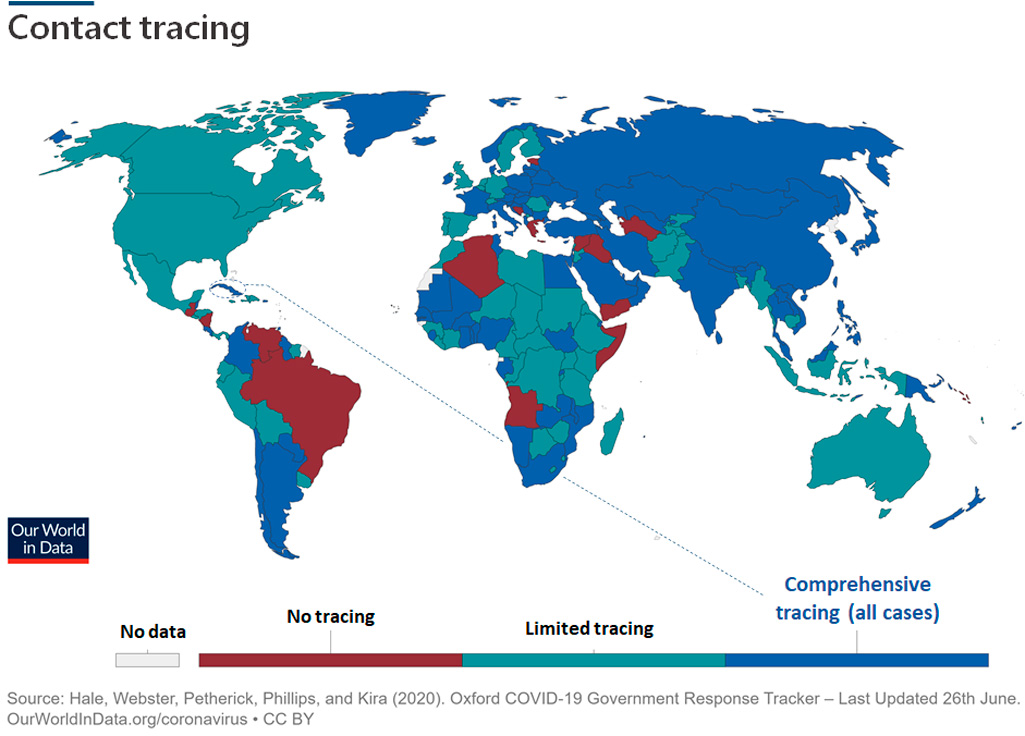
Contact tracing and rapid isolation represent critical tools to reduce the basic reproductive number (R0) of the virus and, therefore, stop the outbreak. A recently published modelling study suggested that by detecting and then immediately Figure 2. Contact tracing status worldwide. Partially modified and reproduced with permission from the Coronavirus Pandemic (COVID-19), Our World in Data (CC-BY license) (Roser et al., 2020). isolating over 60% of the cases and contacts, countries can reduce and control the COVID-19 pandemic. Cuba is one of the countries in the region that traces all contacts (Figure 2). In contrast to the digital approach implemented by other countries (i.e. South Korea), the Cuban approach of massive manual contact tracing was coordinated by the far-reaching primary healthcare system and the collaboration of thousands of medical students and healthcare workers. In combination with molecular diagnostics, a comprehensive program of contact tracing remarkably reduces the impact of asymptomatic and pre-symptomatic patients in fueling virus transmission. The surveillance and contact tracing models deployed by Cuba were praised by José Moya, representative of the Pan American Health Organization in the island (Miranda, 2020), and have been critical to controlling the spread of the virus.
Figure 2. Contact tracing status worldwide. Partially modif ed and reproduced with permission from the Coronavirus Pandemic (COVID-19), Our World in Data (CC-BY license) (Roser et al., 2020).
3.2 Testing program Molecular diagnostics of SARS-CoV-2 infections represents another key player in controlling the COVID-19 pandemic. The Director of the World Health Organization, Dr. Tedros A. Ghebreyesus, highlighted the importance of testing on March 16th by stating “you cannot fight a fire blindfolded (…) we cannot stop this pandemic if we don’t know who is infected.” The RT-PCR (reverse transcription polymerase chain reaction) is the gold standard for laboratory testing of COVID-19. This molecular biology technique allows detection of fragments of the viral genome in early and even pre-symptomatic stages of the infection, facilitating the immediate quarantine of confirmed cases and further contact isolation. Yet RT-PCR is an expensive test and requires a complex infrastructure as well as highly qualify and skilled personnel. As noted, several Latin American and Caribbean countries lack the national infrastructure to develop a mass testing program to detect most COVID-19 cases. Global data show that, in general, countries that deployed a mass, or at least rational, testing program in a timely fashion, significantly reduced the impact of the pandemic by efficiently controlling viral transmission.
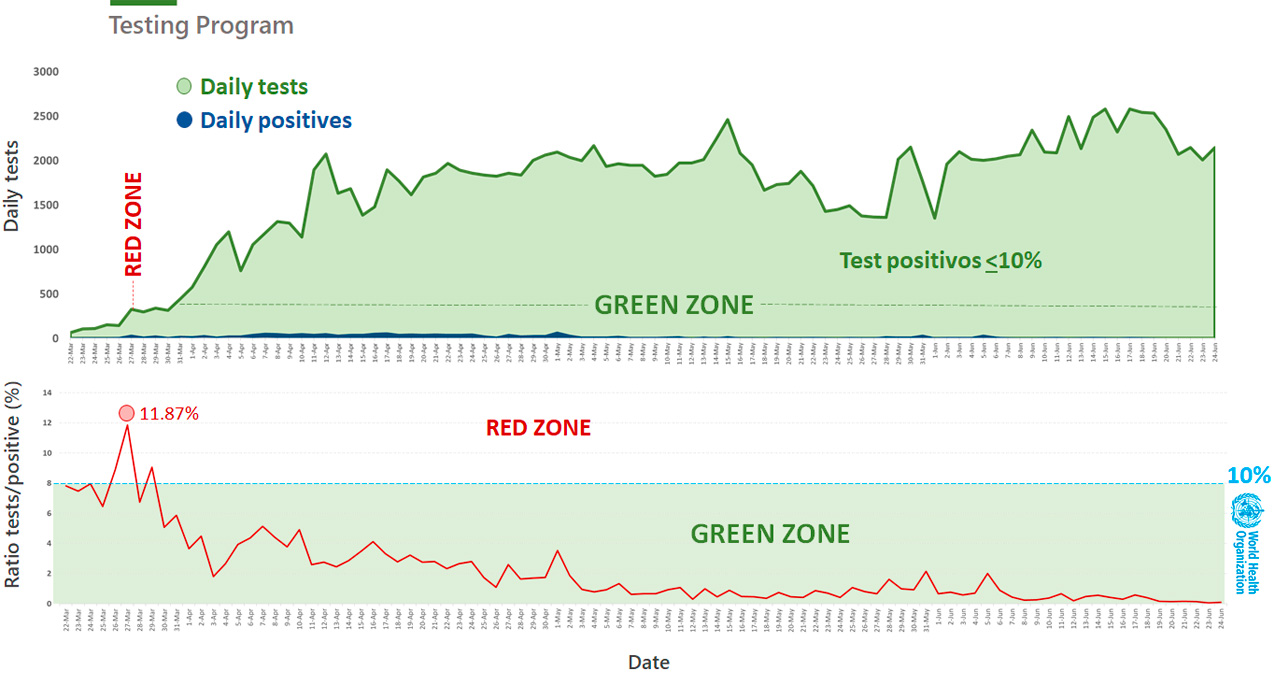
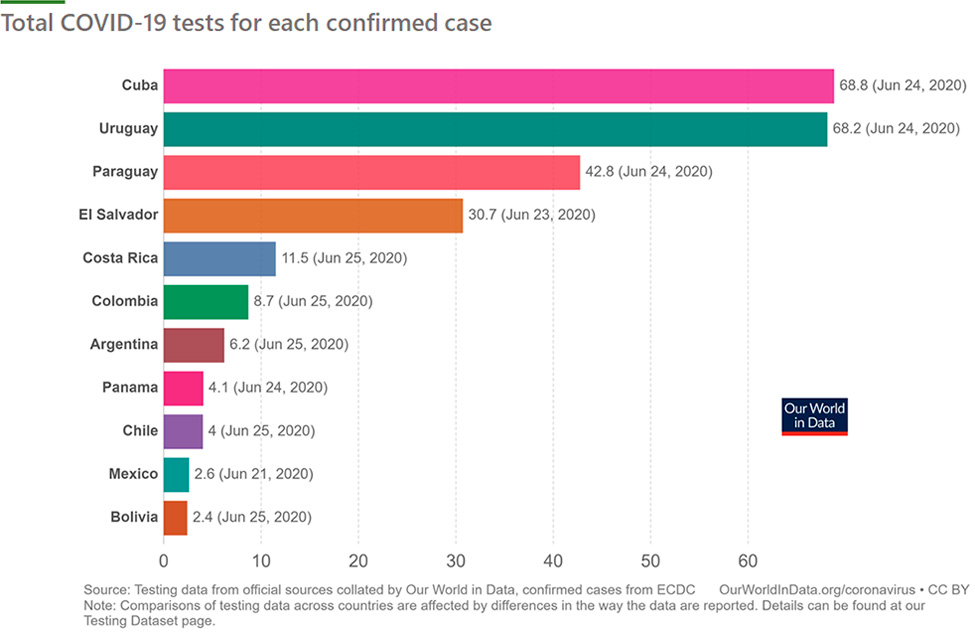
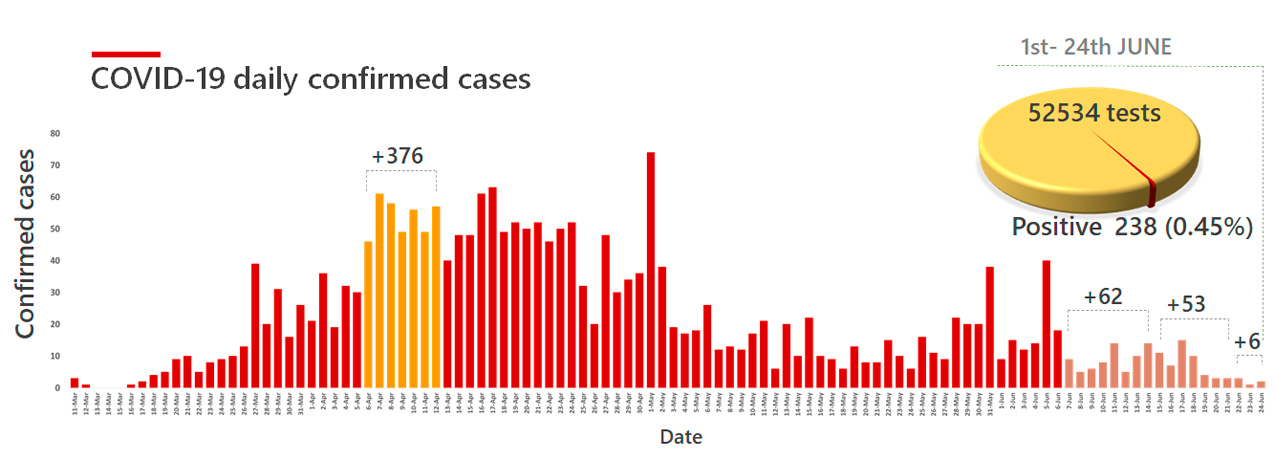
Unable to perform mass testing, Cuba used an alternative scheme of molecular testing enabled by outfitting up to seven laboratories in different regions of the country. The Cuban program followed the WHO recommendations of gradually increasing the laboratorial capacity for the molecular diagnostic of SARS-CoV-2 and, more important, to perform daily tests to ensure that no more than 10% of these tests were positive. This is an important criteria that should be addressed by any national testing program. In contrast to the popular belief which suggests the total amount of tests or the per capita test per million of inhabitants is the primary criteria to evaluate a COVID-19 testing program, it is the ratio of total tests for each confirmed case—which takes into account the size of the epidemic—which is the more accurate indicator. An analysis of the official data shows that, throughout its outbreak, the percentage of positive tests in Cuba (except for 27 March) was always under the 10% recommended by the WHO (Figure 3). Overall, during its outbreak, the ratio of total COVID-19 test/ confirmed cases in Cuba is 68.8 (Figure 4). Considering only data from June, this value increased to 222.2 tests/ confi rmed case.
Figure 3. Results of the Cuban molecular testing program for detection of COVID-19 cases. As noted, during its outbreaks, the percentage of positive cases (except March 27) remained under the 10%, as recommended by the WHO. [Data: Ministry of Public Health, Cuba]
Figure 4. Ratio of COVID-19 test/conf rmed cases for some of the countries in Latin America and the Caribbean. Partially modif ed and reproduced with permission from the Coronavirus Pandemic (COVID-19), Our World in Data (CC-BY license) (Roser et al., 2020).
Evolution of the epidemic and final remarks At time of writing (June 24th), Cuba reported a cumulative total of 2,321 COVID-19 confirmed cases and 85 deaths. The island—except Havana—recently moved to Phase 1 of the post-epidemic period, de-escalating several of the mitigation/suppression measures applied during the critical moment of its outbreak. This decision was made considering the positive trends of epidemiological indicators such as daily confirmed cases and fatalities, active cases, patients recovered, and the occurrence of local events with community transmission. In the month of June, Cuba registered two sequential minimums in weekly confirmed cases, an extremely low ratio of positive tests and one biweekly COVID-19-related death (Figure 5). In addition, along with Uruguay, Cuba reported the highest ratio of recovery, as over 93% of the COVID-19 confirmed cases have been already discharged from hospitalization.
To date, the country has only 63 active cases. Most Cuban provinces (as of June 24th) have gone more than two weeks without new COVID-19 confirmed cases, deaths, or local events. Some of them have reported this trend for more than a month. Finally, the number of daily confirmed cases in Havana has dropped significantly during the last week, suggesting that this territory could be entering Phase 1 of de-escalation shortly.
Cuba applied a functional strategy to control its epidemic, based on the timely application of several mitigation/suppression measures, massive surveil lance of ARI, and the recently so-called “COVID-19 TETRIS”: test, trace, and isolate. In addition, the recommendation to wear face masks in public places contributes to reducing transmission.
Figure 5. Evolution of daily conf rmed cases in Cuba. Weekly maximum (orange) and sequential minimums (brown) are highlighted. The ratio of test/positive cases for June is also shown. [Data: Ministry of Public Health, Cuba]
Some unique aspects of the Cuban response (massive surveillance, contact tracing, the use of isolation centers) were facilitated by preexisting conditions such as a broad and wellorganized primary health care system, the high per capita of medical doctors/millions of inhabitants, and previous experience in rapid evacuations in emergency situations as well as during other epidemics. Remarkably, the massive program of ARI surveillance and contact tracing allowed the early detection of presymptomatic/asymptomatic patients and their early isolation, thus reducing the rate of transmission. Despite some recent controversies, it has been well documented that pre-symptomatic individuals have a high viral load (He et al., 2020) and represent potential major spreaders of the virus. Finally, the Cuban approach reinforced the epidemiological value of applying a rational testing program for the control of the COVID-19 pandemic.
Miranda, B., 2020. Coronavirus en Cuba: cómo funciona el agresivo modelo de vigilancia epi-demiológica contra la COVID-19 [WWW Docu-ment]. BBC Mundo. URL https://www.bbc.com/mundo/noticias-america-latina-52496344 (ac-cessed 6.24.20).
Onder, G., Rezza, G., Brusaferro, S., 2020. Case-Fatality Rate and Characteristics of Pa-tients Dying in Relation to COVID-19 in Italy. JAMA — J. Am. Med. Assoc. 323, 1775–1776.
Roser, M., Ritchie, H., Ortiz-Ospina, E., Hasell, J., 2020. Coronavirus Pandemic (COVID-19) [WWW Document]. OurWorldinData.org. URL https://ourworldindata.org/policy-responses-covid (accessed 6.24.20).
Walker, P., Whittaker, C., Watson, O., Bague-lin, M., Ainslie, K.E.C., Bhatia, S., Bhatt, S., Boonyasiri, A., Boyd, O., Cattarino, L., Cucu-nubá, Z., Cuomo-Dannenburg, G., Dighe, A., Donnelly, C.A., Dorigatti, I., Van Elsland, S., Fitzjohn, R., Flaxman, S., Fu, H., Gaythorpe, K., Geidelberg, L., Grassly, N., Green, W., Hamlet, A., Hauck, K., Haw, D., Hayes, S., Hinsley, W., Imai, N., Jorgensen, D., Knock, E., Laydon, D., Mishra, S., Nedjati-Gilani, G., Okell, L.C., Riley, S., Thompson, H., Unwin, J., Verity, R., Vollmer, M., Walters, C., Wang, W., Wang, Y., Winskill, P., Xi, X., Ferguson, N.M., Ghani, A.C., 2020. The Global Impact of COVID-19 and Strategies for Mitigation and Suppression. Imp. Coll. COVID-19 Response Team March, 19.
Zhang, Y., 2020. The epidemiological character-istics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. China CDC Wkly. Rep. 41, 145–151.
ABOUT THE AUTHOR Amilcar Perez-Riverol is currently Post-Doctor-al Fellow at the University of Sao Paulo State (UNESP) and Post-Doctoral Fellow at the Uni-versity of Aarhus (Denmark) and University of Giessen-UKGM (Germany). He obtained his Doctoral Degree in Biological Sciences (Cell and Molecular Biology) from the University of Sao Paulo State in 2017 and has a Master’s Degree in Microbiology and Virology from the University of Havana (2012). He is former Pro-fessor of Molecular Virology at the University of Havana.
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.