INTRODUCTION
Walter Sisulu University (WSU) is located in a rural area of Eastern Cape Province, South Africa. It has designed an admissions process that considers secondary (high) school academic results along with the candidate’s personal and sociocultural attributes.[1] Seventy-five percent of MBChB enrollees come from secondary school (twelfth grade), and the remaining 25% hold a college degree in science or health sciences. Students are culturally representative of the South African population, that is, more are black as compared to Indian, colored (a self-declared category in the South African census) or white.
Curricular design at WSU medical school, Mthatha, South Africa, includes six educational strategies, called SPICES: Student-centered, problem-based learning favors integrated disciplines and also pursues learning goals involving work in the community (community based). Its flexible learning components (electives) are articulated within a planned curriculum (systematic), so that students’ autonomy to organize their learning goals does not compromise the quality of graduates’ preparation.[2] Problem-based learning (PBL) and community-based education (CBE) are the cornerstones of the WSU undergraduate program leading to the Bachelor of Medicine and Bachelor of Surgery (MBChB).[3,4]
PBL takes place in tutorial groups of 10–12 students, meeting in 2-hour sessions 3 times a week. Other teaching scenarios are arranged around the tutorial groups, and involve active methods, complementing the tutorial learning process. The tutorial groups work with clinical cases that have been pedagogically modeled into learning problems. Students identify what they know and what they need to learn about the problem. These needs become research topics for self-directed learning (SDL) in which students should assess and select the resources they will use.[5] This evoked-knowledge exercise then serves as a bridge for knowledge transfer, since students may connect this learning to encounters with new “patients.”[6]
The variety of cases provides a favorable framework for knowledge application, since knowledge transfer occurs not only within a given learning block, but also across blocks. (In this curriculum, problem contents are organized in four learning blocks: musculoskeletal system, neurosciences, cardiovascular and respiratory systems, and renal and reproductive systems.)
According to McGrath, three levels of causal dynamics, not mutually exclusive, shape a group’s evolution: dynamics within and between individuals; dynamics originating from individuals that influence, for example, the group’s identity, norms and values; and dynamics originating from the group’s particular setting. These dynamics leave their imprint on the group’s adaptations, as in any other open system.[7] From a pedagogical standpoint, Keyton identified five characteristics that define a group and determine its functioning: size, common goals, member interdependence, group structure, and identity.[8] Slavin devided the complex interactions characterizing collaborative learning environments into the following dimensions: motivational, social and cognitive. These were the same observed by De Grave.[9,10]
The use of collaborative learning methods has made it possible to study both the conditions in which a group functions efficiently, as well as the distinctive features in its evolution towards becoming a team. In a team, members collaborate cohesively to reach common goals, showing commitment, respect and personal responsibility; and they regularly assess their performance and contributions to re-direct their work as needed.[11]
Tutorials are constructivist learning environments, in which the search for solutions to a problem that is ill-structured (in the sense that it is messy, like real-world problems) leads to complex reasoning, including analogy, induction, deduction, hypothesis rationale, and prediction.[12,13] In early years of study at WSU, these tutorial groups are the center around which all other student learning scenarios are arranged.
Initial dysfunction is normal, part of the group’s natural evolution involving social and cognitive adjustments, but, if it persists, this will conspire against achieving PBL objectives. Conditions favoring group dysfunction include a problem too complex for an accessible solution; an unreasonable number of topics for students to study effectively; unresolved interpersonal conflicts; insufficient SDL preparation by students; inadequate tutor assistance in cognitive and social interactions; too many students in a group; and lack of group cohesion (students competing instead of collaborating).[14–17]
The objective of this study was to determine student perspectives on which factors affect tutorial group functioning and to detect the presence of these factors in the four learning blocks comprising the second year of medical studies.
METHODS
All 97 second-year medical students were invited to participate in focus groups to begin the research; of these, 38 volunteered.
Two 10-student focus groups were chosen with by simple random sampling within educational and ethnocultural strata in the class to ensure proportionate representation. One group discussed factors favorable to effective tutorial group functioning and the other examined factors negatively affecting the tutorials. Later, the 2 groups met and jointly identified 17 items that had been detected by both groups (despite their different approaches) for later inclusion in a survey questionnaire. All 97 students received the survey questionnaire at the end of their second academic year, asked to voluntarily report the number of blocks (0–4) where they detected each item.
Of the 17 items included in the survey, 14 related to tutorial sessions as such, whereas 3 related to students’ experience with the SLD process; 15 were deemed by the focus groups to have a positive impact on tutorials and 2 negative (“I usually prepared only the learning objectives I was assigned” and “The tutor frequently told us what study topics were needed to fulfill our learning objectives”). For ease of understanding, concepts were expressed in positive terms (e.g., “The topics included were interesting” versus “The topics discussed were not interesting”). For each item, we calculated the percentage of students perceiving it as influential on tutorial group functioning, as well as the percentage of students detecting it by number of blocks, from zero to four. Means and standard deviations were calculated for each item. The 17 items were devided for analysis into motivational, social, cognitive, and SDL learning dimensions (not independent or mutually exclusive) to understand their impact on tutorial functioning. Means and standard deviations were calculated for each dimension.
Ethics The study was approved by the ethics committee of the WSU Faculty of Health Sciences, and students provided written consent prior to participation in focus groups. Questionnaire respondents remained anonymous.
RESULTS
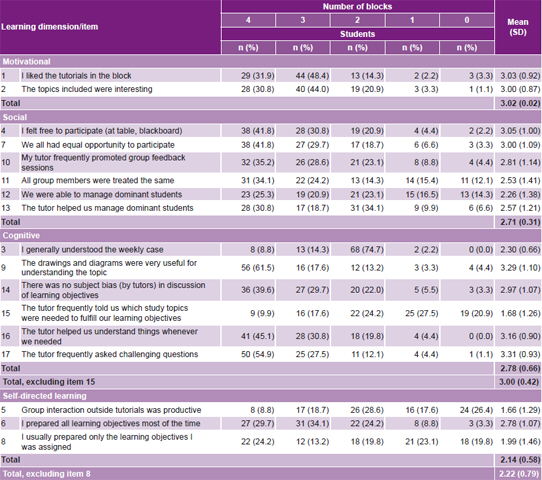
Survey items identified by focus groups as affecting tutorial group functioning were sorted according to the dimensions described by Slavin and De Grave[9,10] (items 1 and 2, motivational; items 4, 7, 10, 11, 12 and 13, social; items 3, 9, 14, 15, 16 and 17, cognitive), with additional information on self-directed learning (items 5, 6 and 8) (Table 1).
Response rate was 93.8% (91/97). Motivational dimension: 80.2% of students (73/91) liked the tutorials in ≥3 blocks, and 74.7% (68/91) said the topics included in the weekly problems were interesting in ≥3 blocks.
Social dimension Most reported that in ≥3 blocks they felt free to participate (66/91, 72.5%) and that everyone had the same opportunity to participate (65/91, 71.4%); 58.2% (53/91) believed that in ≥3 blocks the tutor treated all group members the same. Although 63.7% (58/91) reported that in ≥3 blocks the tutor promoted frequent group feedback sessions, 8.8% (8/91) said this was so in only 1 learning block.
Cognitive dimension A minority of students, 23.1% (21/91) reported that they generally understood the weekly cases in ≥3 blocks. According to 75.8% students (69/91), in ≥3 blocks the tutor helped them understand whenever they needed assistance; and 82.4% (75/91) said the tutor asked them challenging questions that generated discussion in ≥3 blocks.
Self-directed learning Few students found work as a group outside of tutorials productive, and 26.4% (24/91) had no beneficial extra-tutorial experience in any block. Students tended to study all topics defined as learning objectives, 63.7% (58/91) doing so in ≥3 blocks; 37.4% (34/91) prepared only the topics they were assigned.
DISCUSSION
When members of a group feel engaged and accepted, they express their opinions and openly ask for help when needed—signs that the group is working well and that a good learning environment is being created.[18] The fact that in three or more blocks a substantial majority of students liked the tutorials and were interested in the topics studied, and that two thirds felt uninhibited and that all had equal opportunities to participate, suggests that these individuals were part of a group dynamic that stimulated them to participate in interactions fostering knowledge construction.
Tutorial groups at WSU are culturally, ethnically and academically heterogeneous. Their average duration is eight weeks, and during that time, the tutor is responsible for seeing to it that the group structure adopted offers opportunities for all members to participate.[19] One way to do this is to encourage the group to define goals and agree on ground rules to be respected by all members,[20] so that the learning pace of both shy and dominant students can be balanced in favor of group functioning. The identification as a survey item of the need to manage dominant students as a factor affecting group dynamics may indicate that students are better able to deal with shy students than with dominant ones, but also that they can better tolerate shy students, believing that they will not adversely affect the group’s learning process.[14,17]
Table 1: Student perceptions of factors affecting PBL tutorial functioning, Walter Sisulu University, SA (n = 91)
PBL: problem-based learning
Poor oral participation by students does not necessarily mean lack of preparation; cultural differences and level of proficiency in the language of instruction affect student behavior[21] and may explain why one third of students for whom English was not their mother tongue felt their participation inhibited in at least one learning block. At the same time, in PBL, the effectiveness of individual preparation becomes evident in the quality of each student’s participation in group discussions, where those who feel that they are not up to the group’s standard, either in content or language skills to express themselves, may hold back to cover their vulnerability. An alert tutor promotes other learning strategies, such as visual or kinesthetic methods, offering alternative options for active participation in information processing while enhancing individual motivation by achieving better perceived self efficacy.[22]
The inclusion by focus groups of the item “my tutor promoted frequent group feedback sessions” shows that the students appreciated such sessions as a way to get group work back on track. Sessions where group performance and individual contributions are reviewed help develop skills in metacognition, assess group dynamics and learning strategies, and monitor group progress towards collective and individual goals.
When the tutor actively enforces respect for group behavioral ground rules, without promoting and sharing reflection within the group about them, these actions may be interpreted as “personal” by students and regarded as the differential treatment perceived by 87.9% of respondents in at least one block. Medical students at WSU believe that a good group feedback session is not restricted to cognitive learning alone, and they underline that empathy and clarity in the tutor’s message are crucial in eliciting the desired reaction (response) from the students.[23]
The combination of items 9, 16 and 17 should favor deeper learning since the use of drawings and diagrams on the blackboard (79.1% found these useful in 3 blocks or more) complement discussions with visual representations and the tutor’s effective guidance. Furthermore, tutors who stimulate groups with challenging questions and provide explanations when needed (both factors observed by a solid majority in three or more blocks), facilitate concept clarification and application, which promote good group discussions. In turn, when the group engages in quality discussions, this becomes a source of motivation for its members,[24] since this satisfaction encourages them to continue actively constructing knowledge.[25]
Although the survey did not explore the quality of group discussions, it did inquire into students’ understanding of the weekly problem, which can be interpreted as the individual’s self-assessment of effectiveness in finding a solution. The understanding of a new problem depends, first, on the quality and quantity of students’ baseline knowledge as they begin to grapple with it; and, second, on their logical reasoning skills, displayed while trying to apply what they have learned to a specific clinical case.
Each case is a learning opportunity for the gradual construction of knowledge interdependent with the development of clinical reasoning skills, and the “transfer connectors” between cases may enable individuals to complete their understanding of the problem in the following weeks. However, if the topics studied are not addressed in the proper depth in a tutorial session, a poor problem analysis is produced and its understanding slows down; this contributes to what has been called “ritual behavior,” in which students go through the motions of PBL without truly engaging.[26] All the foregoing could account for the findings in the survey (23.1% understood the weekly problem in ≥3 blocks; while 74.7% did so in at least 2 blocks).
The student:tutor ratio at WSU is such that new groups formed in each learning block come from the same set of students and tutors. Since tutors facilitate all four learning blocks, they are aware of students’ learning progress over the academic year. One could speculate that, over time, the student’s self-appraisal of their understanding of the problem may have new connotations, since the learner has more skills to generate hypotheses as well as the necessary inductions and deductions when processing new information about the patient. This would result in poor understanding of the weekly problem in the initial blocks, compared to what the same student may achieve in subsequent blocks. This could be a hypothesis for further research.
One PBL characteristic is that the students decide, in a relatively autonomous manner, which topics they should study in order to progress in understanding and solving the problem.[27] While 27.5 % of students surveyed said that their tutor told them which study topics to study to fulfill their learning objectives in ≥3 blocks, 20.9% did not experience this in any of the blocks. If learning needs are not detected, this may imply insufficient knowledge to establish a connection that enables identification of implicit content in problem construction; but also that the interest generated by the problem, and its analysis, did not advance in the exact direction foreseen by the team designing it. Dolmans found a coincidence of 64% between objectives generated by the students and those foreseen by the school in discussion of twelve problems.[28]
The “hints” offered by the tutor, giving the expression “self-directed” in PBL a more flexible meaning, are used to ensure that the course taken by the group is not too far from the route designed for learning,[29] and also from the planning of self-directed studies, so as to avoid an unnecessary cognitive load.
Some students may like to have a tutor indicating their learning needs (it is faster and requires less cognitive effort), but we consider that this may have a negative effect on tutorial functioning; this item is justifiably excluded when calculating the mean of the cognitive dimension of the survey, resulting in an increased score for that dimension. Students’ knowledge of their tutor’s expertise and preferences could have introduced bias in the selection of learning objectives; the percentage of tutor bias reported in discussion of learning objectives suggests this may be the case.
Tutorial group productivity depends on the individual’s self-directed preparation. The two items that explored students’ strategies for organizing and implementing their SDL indicated that a substantial proportion of students studied only the topics in which they would be expected to actively participate in the tutorial. Weekly meetings on tutorial group functioning at WSU led to a recommendation that work should not be subdivided, since the smaller the number of individuals studying the same topic, the lower the probability of enriching problem discussion.[30]
Individual assignment of specific topics decreases cognitive load and produces “experts” with narrower cognitive scope to apply to case comprehension and, consequently, to actively participate in co-construction of knowledge. The tutor’s skills in content facilitation compensate for students’ uncertainty about how thoroughly a topic should be studied by offering a holistic vision achieved by understanding the patient and the patient’s problem.[31]
Advancing in construction of knowledge about a problem over the three weekly sessions is not linked to a single discipline, but rather contributes to a transdisciplinary approach. Therefore, the group’s strategy for problem-solving and moving ahead in each problem through various disciplines determines SDL organization and implementation. The students showed no pronounced preference for preparing all the learning objectives versus preparing only those assigned (items 6 and 8, respectively), and although at the group level both can lead to problem solution, this is not so at the individual level; hence the decision to recalculate means and SDs, excluding item 8.
Study groups convened without the tutor, while optional at WSU, are recommended because they build esprit de corps, and enable monitoring and coregulation of the learning process.[32] The fact that so few students found them productive in a majority of blocks suggests scope for improvement. It would be worth exploring in more depth the reasons these groups are unproductive and ways they could be reinforced as a learning tool.
Students at WSU assigned the tutor an important role in tutorial functioning and productivity, expressed through the number of items included in the survey that indirectly appraise the social and cognitive congruence of the tutor, who is expected to motivate interactions between and among individuals while constructing knowledge.[31] Tutors were reported to be more effective in the cognitive realm than in facilitating social aspects of tutorials. Other research with WSU students also found the social facilitation skills of tutors weaker than their cognitive skills,[33] the latter also assigned greater importance by students.[34]
The subjectivity implicit in individual reports about the factors explored in the survey is a study limitation, but it does provide useful insights into student preferences and priorities in tutorial functioning, and their perceptions of what needs to be improved.
CONCLUSIONS
Tutorial group work at WSU is reinforced more by motivational and cognitive factors than by social and SDL factors. Skills for managing social aspects of the tutorials should be included in tutor training, with particular emphasis on systematic practice of group performance feedback. Students should receive more in-depth training in SDL strategies, and SDL analysis should be included in group feedback sessions. Poor productivity of study groups outside tutorials suggests the need for their assessment and probable redesign.
ACKNOWLEDGMENTS
The authors thank Dr Agustín Vicedo for his critique of the manuscript in preparation, as well as the students involved in this study.