

Figure 1: Neuronica. Cuban computerized system for neurophysiological studies such as evoked response testing and electromyography.
Nearly one quarter of the global burden of disease stems from neurological, psychiatric and neurodevelopmental disorders due to malformations or dysfunctions of the central nervous system.[1] Such neuropsychiatric conditions influence quality of life worldwide, causing one third of years lost due to disability (YDL).[2]
Ranging from congenital conditions to dementias of the elderly, these disorders appear throughout the life cycle and also account for a substantial proportion of mortality. Recent advances in neuroimaging and neuroinformatics have opened the way for early identification of dysfunctional brain networks, providing essential information for the early detection, proper diagnosis, treatment selection, and follow-up of people with disabilities due to brain disorders.
Technology thus holds the promise of effectively improving management of these conditions. In most of the world, however, fulfillment of this promise is derailed by the essential contradiction between the vast number of people needing diagnosis and treatment, and the high cost and elitist application of neurotechnologies. The inequitable use and distribution of these resources is especially critical in the developing world, where the acquisition of neuroscience technology is scant and usually profit-driven.

Alternatives are being developed in Cuba, where an attempt has been made over time to use scarce resources in a rational, patient-centered way in the context of a universal, public health system. The essential philosophy is to use the most readily available and least expensive technology in broad-based screening programs designed to identify those patients who require more sophisticated testing and access to more costly and complex diagnostic tools. Key to implementation has been the training of human resources with a mandate for innovation; hence the development of a domestic medical equipment industry capable of introducing technologies that are both cutting-edge and cost effective.
One example of this approach can be seen in neurosciences. Since the early 1970s, the Cuban Neuroscience Center (CNEURO), in collaboration with the Ministry of Public Health,has been designing and introducing new technologies to diagnose and assist persons with disabilities due to brain disorders (Figure 1) (Table 1).[3] The first decade was dedicated to setting up the national industry for such domestically engineered medial equipment, which wouldserve as the foundation for the development of a national neuroscience diagnostic network in the 1980s. Creation of this network enabled us to launch one of the world’s first national programs for early detection of hearing loss, which, in turn, enabled the health system to pinpoint the children most in need of hearing aids and other special services, including the 145 (22 of them deaf-blind) who have been fitted with cochlear implants. (See Pérez, MC, et al, A 25-Year Review of Cuba’s National Screening Program for Early Detection of Hearing Loss, pp. 22-29, this issue.) During the 1970s, we also collaborated with US colleagues on developing of one of the earliest methods for computerized EEG analysis or qEEG,[4] and Cuba became the first country to introduce this technique systematically in a public health system.[5]
Stratified Active Screening for Brain Disorders
The hearing loss study became the prototype for a stratified active screening strategy, which relies on Cuba’s comprehensive primary health care system for rational, equitable use and distribution of diagnostic technologies for brain disorders. This process involves three levels of testing using increasingly more sophisticated equipment with increasingly smaller numbers of patients at higher levels of care (Figure 2).
Level I: Active cognitive/neurophysiological screening of whole populations for brain disorders. Screening at this stage is done by paramedical technicians using low-cost diagnostic tools built around a hand-held computer or personal digital assistant (PDA), which guides the user through a decision tree and even administers several sensory and cognitive tests. This stage of screening is designed to be very sensitive but allows a certain
percentage of false positives that are winnowed out at subsequent levels.
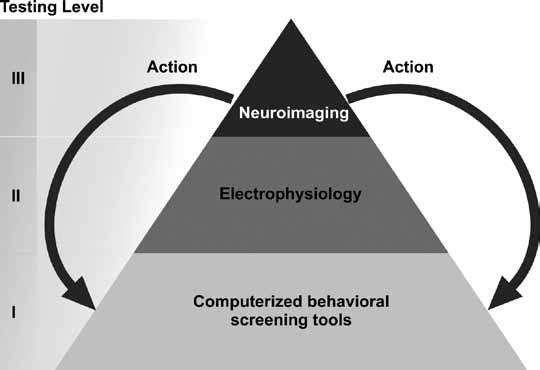
Figure 2: Stratified Active Screening for Brain Disorders
Level II: Initial diagnosis by specialists, including low-cost electrophysiological testing complemented by expert consultations via telemedicine. Treatment for some cases may be indicated at this stage.
Level III: Specialized diagnosis using more sophisticated and more costly tools, including neuroimaging. In most cases, treatment can be provided at the primary care level.
Figure 3 outlines the steps in this strategy for development and application of neuroscience technologies. Several examples illustrate how this strategy is applied in practice.
Active Screening for Neurodevelopmental Disorders
Neurodevelopmental disorders are a health problem among children. An early detection strategy during the first five years of life is crucial, given the brain’s plasticity during this stage of development.
In 2005, a study of several neurodevelopmental disorders was carried out among 222 infants and children in Havana City province, representing the total population aged 0-5 years in the geographical catchment areas of two polyclinics in Cotorro Municipality. The children were screened for impaired cognitive and motor development, hearing and visual impairment, language difficulties, and autism. The tests relied on paper and pencil.
The study, using the three-level stratified active screening model, included: 1) community-based screening for neurodevelopmental disorders, 2) neurophysiological and clinical testing and diagnosis by an interdisciplinary team, and 3) specialized intervention and treatment. After the evaluation, we were able to establish 95% sensitivity and 86% specificity. Based on these results, the Cuban Ministry of Public Health decided to scale up the screening program to the whole country. In order to make this next step possible, CNEURO developed the N-PED hand-held automated tool for Level I screening (Figure 4).[7] This PDA-based tool is programmed to perform a structured set of sensory and neuropsychological tests that can easily be applied by paramedical personnel and has proven to be even more sensitive and specific than the paper-and-pencil tests.
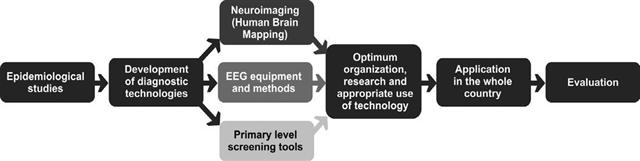
Figure 3: Active Screening Implementation Flowchart

Figure 4: N-PED: Automated PDABased Neurodevelopmental Disorder Screening Tool
Active Screening for Learning Disabilities
Epidemiological data provide the foundation for establishing any healthcare strategy or educational program aimed at protecting the neurodevelopment of school-age children. Therefore, in 2006, a large-scale National Learning Disability Prevalence Study was conducted with 16,097 children in the 3rd and 6th grades in urban and rural schools throughout Cuba. In the
first level of testing, achievement tests were administered that found a 6.35% prevalence of Reading Learning Disorder (RLD) and a 7.19% prevalence of Arithmetic Learning Disorder (ALD).
In the second level, batteries of neuropsychological tests were used to assess the prevalence of Developmental Dyslexia (RD) and Developmental Dyscalculia (DD), yielding a 4.27% prevalence of RD and a 3.17% prevalence of DD.[8] Results of this study established the need for school-based rehabilitation programs to aid children with these learning disabilities. CNEURO therefore devoted resources to a) adapt well-established
software for use in Cuba, such as “Number Race,” developed by Wilson and Dehaene, for treating ALD and DD, and b) create its own rehabilitation software, such as “ABC” for
RLD and RD. The Ministries of Education and Public Health are currently studying how to put these technologies to work in joint national programs.
The Cuban Human Brain Mapping Project
Finally, the Cuban Human Brain Mapping Project exemplifies one of the most advanced applications of neuroscience technology in the country. This project was initiated in 2004 to produce a normal human brain atlas that clinicians, pathologists, and technicians can use for comparison when examining signs of brain disorders, injuries and abnormalities.[3] The project involves active screening, data gathering, standardization of normative data, analysis of new knowledge provided by EEG procedures and results, prediction of individual differences, and clinical applications.
For this project, active screening was used to detect the healthiest subjects for more advanced testing, rather than subjects with a problem requiring further examination and diagnosis. A random sample of 2,104 residents of La Lisa municipality in Havana City province was selected by age groups. Several screening tests and a questionnaire were applied to detect existing pathologies, and specialized evaluations were also conducted
by neurologists, psychiatrists, and others. A total of 590 individuals were found to be in good general health, and they were then examined with high-field MRI (SIEMENS 1.5 Tesla) and high-density EEG (MEDICID-5, 64 channels, designed by CNEURO). Blood samples were also taken for further genetic studies.
New neuroinformatics software was also developed by CNEURO and used to store and analyze each piece of information. The neuroinformatics processing pipeline,[9] for example, is a set of software tools for processing and extracting relevant information
from brain images (Figure 5).
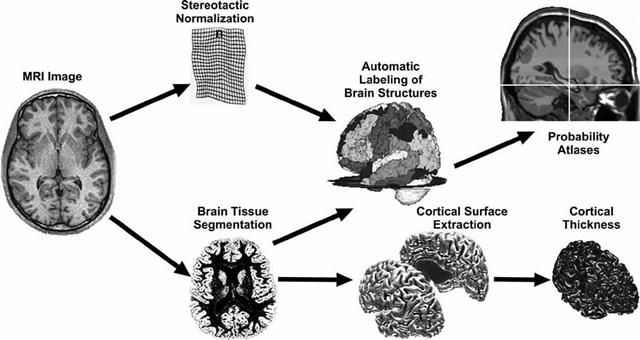
Figure 5: MRI Processing Pipeline
Each subject’s structural MRI image is put through several automatic processes by specialized neuroinformatics software. One line of processing (top, Figure 5) first warps the image into a standardized space called stereotactic space. It is also segmented into gray and white matter (bottom, Figure 5). With the segmented brain in stereotactic space, over 116 brain structures can be identified, and their volume measured. This information is then used to construct probability atlases. Brain structure sizes vary with age and sex, as well as with disease.
The segmented brain image can also be used to view the cortical surface separately and, in turn, to measure its thickness at all points. Cortical thickness is a sensitive measure of brain maturation and is altered by disease. This part of the pipeline was incorporated
thanks to joint work with the Montreal Neurological Institute.
These methods have been used to study groups of patients with different brain disorders. Work is in progress to establish these techniques as part of the third level of active screening.
Moving Forward
The strategy described above is not without its fits and starts: while domestically designed and produced technologies are ideal for active screening, the pinch of economic limitations can still be felt in unavoidable delays at various stages. Nevertheless, if
the developing world is to aim for healthy populations, then the experience and results of Cuban neuroscience encourage us to think that such equitable, rational, community-based and patientcentered stratified screening holds the key to moving scarce resources
to the places and people who need them most—and also spurs the kind of innovation that generates better and more appropriate technology.

- Reynolds EH. Brain and mind: a challenge for WHO. Lancet. 2003 Jun 7;361:1924-5.
- World Health Organization. The global burden of disease. 2004 update. Geneva: WHO; 2008. Available from: http://www.who.int/healthinfo/global_burdendisease/GBI)_report_2004update_full.pdf.
- Reed G, Torres J. Riding the brainwaves of Cuban science: Pedro Valdés Sosa, MD, PhD, Vice Director for Research and Director of Neuroinformatics, Cuban Neuroscience Center, Havana. MEDICC Review. Spring 2008;10(2):11-3.
- John ER, Karmel BZ, Corning WC, Easton P, Brown D, Ahn H, et al. Neurometrics. Science. 1977;196:1393-410.
- Valdés P, Valdés M, Carballo JA, Alvarez A, Díaz GF, Biscay R, et al. qEEG in a public health system. Brain Topogr. 1992;4:259-66.
- Camacho H, Cobas M, Icart E, editors. Lives to live: Psycho-social study of people with disabilities and psycho-pedagogic, sociological and clinical genetic study of people with intellectual disabilities in Cuba. Havana: Abril; 2003.
- Santos E, Pérez MC, Alvarez MB. Certificado de depósito legal facultativo de obras protegidas. Registro CENDA Habana No. 2738. 2007, Havana.
- Butterworth B, Reigosa V. Fundamental information-processing deficits in dyscalculia. In Berch D, Mazzocco M, editors. Mathematical Learning Disabilities.
New York: Brookes Publishing for NIH/NICHD, 2007. - CNEURO’s MRI Processing Pipeline is available as an online open access tool at: http://www.thomaskoenig.ch/Lester/ibaspm.htm
