QUALITY CARE REQUIRES QUALITY INFORMATION
The AIDS epidemic has evolved over the last three decades and continues to be a global health priority. Access to antiretroviral therapy reached 42% global coverage in 2008;[1] in December 2009, an estimated 5.2 million people living with HIV/AIDS in low- and middle-income countries were receiving antiretroviral therapy, a 30% increase over the same period the previous year.[2]
Care for people living with HIV is one of the greatest challenges for health systems, providers and their institutions,[3] and requires access by physicians and other health professionals to accurate and comprehensive information.[4] Effective treatment requires innovative methods of disseminating knowledge and information to ensure delivery and monitoring of quality services.[3] Depending on available infrastructure and human resources, different strategies can be used to manage HIV/AIDS information,[5] ranging from independent databases with communications and alerts by e-mail to web-based digital medical registries. Use of digital HIV/AIDS medical registries in developing countries has been shown to be effective in supporting provision of quality medical care, including antiretroviral therapy.[6–10]
AIDS is a major cause of death in the Caribbean, where high HIV prevalence is also recorded.[1] Even with a slight increase in recent years,[1] Cuba maintains an extremely low prevalence of 0.1% in the population aged 15 to 49 years.[11] From 1986 through 2011, 15,824 persons were diagnosed with HIV, 80.8% of them men.[12] HIV transmission in Cuba has occurred mainly between men who have sex with men.[13] By the end of 2011, 2455 people had died of AIDS.[14]
From 1986 to 1993, Cubans diagnosed with HIV were institutionalized and attended exclusively in the 14 sanatoria set up in various provinces, a strategy provoking considerable debate.[15–18] At the end of 1993, the Ministry of Public Health (MINSAP, the Spanish acronym) implemented an ambulatory care system[19] aimed at social reinsertion of persons living with HIV. By late 2008, 74% of HIV-diagnosed persons in Cuba were enrolled in the ambulatory care system and 26% lived in the sanatorial system, now called comprehensive care centers for persons with HIV/AIDS (some there temporarily while completing the Learning to Live with HIV training program).[20]
Until 1996 some patients received antiretroviral monotherapy or bitherapy. From 1996 to 2001, a small number of patients received triple therapy, mainly thanks to drug donations from abroad. Since 2001, with domestic production of several generic medications,[19] antiretroviral therapy (ART) became a standard regimen, free of charge to patients.[14,19] More therapeutic combinations were introduced starting in 2003, with support from the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund). The same year, Cuba achieved universal ART access[19] for all those meeting clinical eligibility criteria: confirmed HIV infection, CD4 lymphocyte count of less than 350 cells/mm3, viral load of more than 55,000 copies/mL and opportunistic infection.[21] By close of 2009, over 4000 persons living with HIV/AIDS were receiving treatment,[11] and by close of 2010, 5692 persons were receiving ART.[13]
ART use has been found effective in Cuba, with improvement in immunological parameters and survival rates, fewer opportunistic infections and lower AIDS-related mortality.[19,22] However, drug resistance and treatment failure associated with non-adherence have been documented.[22,23] Thus, achieving high adherence levels has become a priority health strategy for Cuba’s National Response Program to HIV/AIDS.[24]
This Program depends on strict control and monitoring to ensure satisfactory followup and medication delivery to every patient receiving ART. In a country with limited economic resources such as Cuba, this requires special attention: for example, it is vitally important to know the exact number of persons under treatment in each locale, as well as the combinations prescribed, to ensure supply continuity and avoid shortages. Furthermore, for sound decisionmaking, attending physicians and other health professionals involved in treating persons living with HIV/AIDS need immediate and secure access to clinical information on their patients, especially CD4 lymphocyte counts, viral loads and previous therapeutic combinations.[4,25]
This paper describes the experience of the Pedro Kourí Tropical Medicine Institute (IPK, the Spanish acronym) in implementing an informatics tool to support clinical followup and ART of persons living with HIV/AIDS.
SIDATRAT DEVELOPMENT
Since the onset of the HIV epidemic in Cuba, IPK has been a national reference center for specialized care of persons with opportunistic AIDS-related infections and for training health care providers in clinical approaches to HIV/AIDS. Since 2001, IPK has led implementation of the Cuban government’s strategy to provide universal access to ART for those patients requiring it.
SIDATRAT Users Comment Primary-care physicians on patient
SIDATRAT arose in response to the need to ensure appropriate control and clinical followup for ART patients.
The first version of SIDATRAT was launched in 2001, consisting of a Microsoft Access database located at the IPK[19] that compiled patients’ data: general (from MINSAP’s AIDS limited-access data system), opportunistic infections; clinical information including stage of HIV/AIDS infection, viral load and CD4 counts; treatments; adverse reactions to medications; and studies on therapeutic resistance and adherence.[5] Communication with provinces to update information was done via telephone and email. Compiling all this data in one place had great initial impact, given that the IPK measured only viral load and CD4 count, while all other tests were conducted in provincial hospitals and sanatoria.[19]
SIDATRAT’s second generation was launched in 2005. It was web based and utilized an Apache server, PHP and MySQL, enabling use of a client-server platform. The servers were located at the IPK and connection by authorized provincial users was assured through INFOMED, the public health system’s nationwide telematics network.[26] This version has continued to evolve, including new specialized services and functions to help improve information quality and patient care.
By 2008, all information on CD4 count, viral load and treatment of persons living with HIV/AIDS in the country was registered in SIDATRAT. As decentralized comprehensive ambulatory care for persons living with HIV/AIDS was strengthened at the primary care level,[27] new services were established in various provinces to measure patients’ CD4 count and viral load. But these data were not incorporated into SIDATRAT. Since 2009, due to administrative MINSAP decisions, SIDATRAT contains primarily followup data on patients receiving treatment at the IPK (those in all western provinces plus serious cases seen from throughout the country), with updated data available to physicians anywhere in the country whose HIV patients are seen at the IPK.
SIDATRAT FEATURES
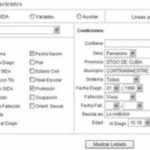
General patient data SIDATRAT is updated with general data on patients from MINSAP’s AIDS limited-access data system. These include: first and last name, gender, date of birth, date of diagnosis, age at time of diagnosis, municipality and province of residence, and date of AIDS onset. All such general information is entered by system administrators, and personnel from IPK services entered data on doctor visits, clinical condition and treatment. Attending physicians, in both IPK and municipalities, have access only to information on their own patients, while provincial or regional health personnel in the HIV/AIDS program can access aggregate data on patients in their province or region registered in SIDATRAT. The system allows multiple reports to be generated from different combinations of these variables (see Figure 1).
Figure 1: Screenshot of menu for generating reports from general patient information
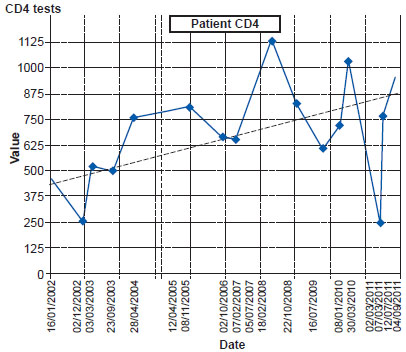
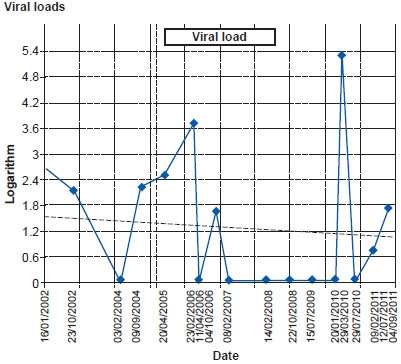
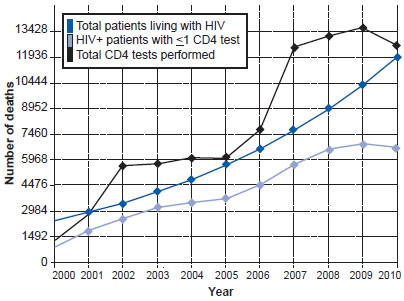
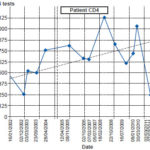
Patient followup data SIDATRAT records CD4 counts, viral loads and the results of other lab tests, as well as endoscopic and imaging studies, AIDS classification, opportunistic infections, subtype and resistance studies, and the scheduling and attending of followup visits. The tool permits extracting reports, totals and graphics from information compiled from laboratories and other services. These are helpful to physicians for making treatment decisions (see Figure 2). Decisionmakers can see which patients are not attending followup appointments or have not had CD4 or viral load studies in a period of time, and track tests conducted (see Figure 3).
ART management The system registers persons in treatment, regimen composition, schedules, number of tablets per day, adverse drug reactions, locations of pharmacies providing medications, and reasons for prescription or treatment changes. It calculates results indicators and patient survival over a given period. By continually updating each patient’s treatment plan, SIDATRAT can identify drug needs for each locale, which is useful to ensure uninterrupted treatment. The system can display the total number of patients using each medication and combination, as well their province of residence. It can calculate total requirements over a given period for each registered locale, province or the entire country. It can alert physicians about patients with low CD4 counts or high viral loads who have not yet started treatment, and about patients in treatment who are not seeing their doctor for followup. Thus, attending physicians have access to the information they need to prescribe or change antiretroviral therapy.
Figure 2: Sample patient CD4 counts and viral loads over time
Information security and confidentiality The central SIDATRAT server is installed at and functions from the IPK network. It is certified and meets national information security standards established by the Ministry of Informatics and Communications’ Office for Security of Information Networks.[28]
Authorized users are issued a user ID and secure password to access SIDATRAT through Infomed, enabling communication among professionals and technicians of national health system institutions.[26,29] Users’ system roles (administration, write/read, read only, access to patient information, connection from local or national network) are defined based on the function they perform and their information needs. Their tasks are defined by a) where they work—specialized laboratories, pharmacies, medical registries, outpatient services, treatment commission (an expert group that decides treatment plans), imaging departments or; b) in the case of phisicians, by the patients in their care. A dynamic menu is constructed for each user, with access dependent on approved privileges.
Each access event is recorded, including date, log-on time, log-off time, and IP address. All webpages visited and searches conducted are recorded to monitor information use and protect confidentiality. A system administrator monitors operations daily, including all user access events and actions. The database is backed up to external hard drives three times a day.
EXPERIENCE WITH SIDATRAT
Since 2005, the current version of SIDATRAT has been used for daily patient monitoring, as a research tool, for regional monitoring and to calculate territorial indicators. The system includes e-mail and instant message services, enabling real-time communication among users, including specialists in medical registries, imaging, and laboratory medicine; as well as physicians treating individuals with HIV/AIDS at IPK, comprehensive care centers for persons with HIV/AIDS and in their municipalities. These services are particularly helpful for new specialists who need advice and support from more experienced colleagues across the country.
By December 2011, SIDATRAT had registered 15,824 HIV-diagnosed persons, 6814 of these patients in ART. This includes 104,781 CD4 counts; 30,994 viral loads; and 14,321 prescribed treatments and changes in treatment. As a result, SIDATRAT has identified the most common drug combinations as: lamivudine + nevirapine + zidovudine (48%) and lamivudine + nevirapine + estavudine (15%). The primary reasons for changing treatment have been adverse reactions to medication, among them: skin rash in patients using nevirapine, nausea and vomiting with indinavir, and anemia in patients using zidovudine. Lipodistrophy has been observed in the combination of protease inhibitors and estavudine.
Problems and challenges Although the system is highly user-friendly, physicians and other health professionals who begin working with SIDATRAT receive training and educational sessions to familiarize them with the system and its options. A search tool has been developed to help SIDATRAT users and administrators find patients whose names have been recorded incorrectly, who are concurrently receiving more than one treatment, or who die while in active treatment.
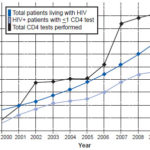
Figure 3: CD4 tests performed annually at IPK, 2000–2010
The two SIDATRAT administrators, who work full-time at IPK, periodically review information quality and completeness, following up with personnel in charge when data are missing. Maintaining updated clinical records is a key challenge to maintaining the system functional. IPK has increased the numbers of computers and trained staff in areas supplying information to SIDATRAT, understood as a contribution to improving quality of care for persons living with HIV/AIDS.
AN EVOLVING SYSTEM FOR AN EVOLVING EPIDEMIC
The first version of SIDATRAT permitted more rapid and complete adoption of clinical guidelines by medical personnel attending persons with HIV/AIDS. As with similar local efforts in the USA[24] and Malawi,[30] SIDATRAT could be implemented at relatively low cost with local resources and great potential to improve medical care. In general, implementation of an informatics system such as this is a difficult and expensive activity calling for substantial interaction between the hospital installing it and the supplier.[31] In this case, SIDATRAT was developed in IPK’s biostatistics and informatics department (registered in the National Copyright Center, CENDA: #2941–2008).
The web version of SIDATRAT, similar to a telemedicine project in Mali,[32] facilitates interchange with experts by remote connection and maintains good infrastructure and national-level access, which helps clinics meet their information needs.[33] At the same time, it demands strict compliance with established security standards for digitized health information.[34]
Our experience is that patients attending periodic checkups at IPK and in the various municipalities feel more confident and secure when the physician can show them monitoring graphs of CD4 counts and viral loads, directly on screen or in hard copy. Similarly, health personnel report finding it helpful to use images to explain to their patients the changes in different parameters related to their health status.
Future development of SIDATRAT includes protocols for research studies involving persons living with HIV/AIDS in the areas of pathological anatomy, nephrology and dermatology. Tools to connect SIDATRAT with laboratory equipment have been developed, helping reduce data entry errors and thus improving information quality.[35] Expanded use of SIDATRAT in Cuba could support researchers and decisionmakers in undertaking a variety of studies related to disease progression, treatment evolution, therapeutic adherence and compliance with clinical followup. SIDATRAT has been offered to the UNDP in Havana for sharing with other developing countries interested in adapting it to their conditions to contribute to better care and followup of persons living with HIV.