INTRODUCTION
Global prevalence of obesity has reached alarming proportions.[1] In Cuba, the rise in numbers of overweight and obese children, especially preschoolers and adolescents, is similar to that observed in developed countries.[2]
Possibly the most common disorders related to child and adolescent obesity are psychological. They include low self-esteem; stigmatization and school failure; distorted body image; social maladaptation; social inhibition; and feelings of inferiority, rejection and insecurity; as well as emotional problems, most commonly depression and anxiety.[3–6] In many cases, it is hard to tell whether these disorders are the cause or effect of obesity.
Dias-Encinas reported that the health-related quality of life of morbidly obese children was similar to that of children with cancer.[7] Other investigators have found that obese adolescents and young adults tend to have a lower household income and live in poverty in adulthood.[8]
Recent studies have revealed association between body weight and family lifestyles and noted the psychological repercussions of excess body weight. They indicate that obesity is associated with family dysfunction, unhealthy diet, unhealthy habits around family meals, a family pattern of excessive sedentary leisure activities, lack of regular physical exercise, irregular meals, lack of family involvement in treating obesity in children and adolescents, and difficulty providing the emotional and behavioral support so necessary for people in treatment. The term “obese family identity” has even been coined.[4,6,9–11]
The purpose of this study is to describe the psychological, behavioral and familial factors present in a group of obese children and adolescents in Cuba.
METHODS
This is a qualitative cross-sectional study of obese children and adolescents in the Medical–Surgical Research Center (CIMEQ, the Spanish acronym) psychology service from January 2009 through December 2012. The study population consisted of all obese children and adolescents seen in that time period: 202 (117 male and 85 female) aged 3–18 years, with an average age of 9.9 years.
Procedures A psychological assessment was performed to explore psychological, behavioral, and familial factors associated with obesity, as well as psychographic characteristics of the study population. This involved projective drawing (a self-portrait, a family portrait and a drawing on a subject chosen by the child/adolescent),[12] interviews with the child/adolescent and parents, and a sentence completion test.[13]
Drawings are nonverbal techniques that enable children or adolescents to express themselves freely, with fewer defenses, enabling researchers to approach them in their own language. This affords opportunity to learn how they perceive their environment, while assesing their ability to express their ideas as well as emotional responses to their reality. Drawings were done alone to prevent copying; participants were given 8½ x 11-inch sheets of paper and red, blue, yellow, green, brown, black, purple, and orange colored pencils and the option of using an ordinary pencil. No rulers or other implements were permitted. García’s indicators were used to analyze drawings: formal or structural indicators (e.g., legibility, size, proportion), color indicators (e.g., presence of color, appropriateness, color preference) and human figure drawing indicators (e.g., completeness, mutilations, expressivity).[14]
The drawings were followed by interviews and application of the Rotter Incomplete Sentence Blank.[13] These activities were conducted in a location with good lighting and no interruptions.
The personal interview is a qualitative technique that was used to explore certain topics in greater depth and assess the subject’s understanding and emotions, feelings, attitudes, and conceptions related to obesity. For interviews with parents and children (conducted separately) we developed an outline that addressed:
- eating habits and physical activity;
- family history of obesity;
- psychological impact of obesity;
- risk perceptions and sense of family responsibility for child or adolescent’s obesity;
- ideals of beauty and health;
- child’s and family’s strategies to deal with obesity;
- attitudes that can potentially lead to psychological alterations in the family; and
- potentially traumatic events.
We used an adaptation of the Rotter Incomplete Sentence Blank to explore conflicts and essential problem areas. The patient is instructed to complete sentences spontaneously; individual responses are scored by the examiner according to a guide and scores calculated for the entire instrument and by spheres—nutrition and physical activity, psychological impact of obesity and body image satisfaction.[13]
Variables We assessed individual psychosocial and familial factors that affect judgments and attitudes about obesity, as well as its treatment and evolution.[14]
Eating habits were defined as healthy when a balanced diet (balance and variety of types of food) was the rule and unhealthy when fat- and sugar-rich foods predominated. Assessed in both children/adolescents and families.
Physical activity level was defined as active if the subject engaged in sports or active play three or more times per week; sedentary if less frequently. Assessed in both children/adolescents and families.
Body image satisfaction was considered to exist when a subject expressed acceptance of and comfort with his or her body image; dissatisfaction when the subject expressed lack of acceptance linked with obesity.
Emotional state was considered disturbed when there was a prevalence of anxiety, hostility, irritability, distress or depression; and undisturbed in the absence of any of these symptoms.
Family attitudes were those directly related to family functioning and the types of relationships, connections, losses, stimuli, limits, norms, and effects surrounding the child/adolescent. Classified as negative were attitudes such as overprotection; rigidity and authoritarianism; permissiveness; rejection, conflicts over parenting; abuse; paranoid behavior; guilt-inducing attitudes; inconsistency; complacency; stimulation of socially inappropriate behavior; and perfectionism. Attitudes were described as positive if no potentially pathogenic attitudes were reported by the family.
Ethics Study purpose and methods were thoroughly explained and confidentiality of information was assured. Children/adolescents old enough as well as their parents provided written informed consent for participation. The study was approved by the CIMEQ research ethics committee.
RESULTS
We triangulated information from all three techniques to describe the behavioral, psychological and familial characteristics of participants. In 96% (194/202) of cases, children/adolescents had unhealthy eating habits, such as:
- preference for such foods as sweets, bread, ‘junk food’ and fried foods;
- food compulsions, with a climate of anxiety around food;
- inappropriate mealtime locations and activities (e.g., eating in front of the television) and rituals parents developed to prompt children to eat; and
- difficulty complying with a medically prescribed diet.
Some 88.1% (178/202) of children/adolescents were sedentary, with a pronounced preference for computer games, watching television, drawing, reading, playing handheld video games, as well as resistance to physical exercise.
The majority (92.1%, 186/202) were dissatisfied with their body image in relation to obesity and suffered low self‑esteem, which was heavily reinforced by external forces (such as teasing by other children). A smaller majority (80.2%, 162/202) reported emotional disturbances, chiefly anxiety, hostility, irritability, low tolerance for frustration, and problems with impulse control and acceptance of limits. Also present, although to a lesser extent, were symptoms of distress and depression.
Negative family attitudes were found in 72.3% (146/202), most important among them:
- permissiveness—affection without authority—where behavioral limits are neither set nor adequately defined, causing children/adolescents to have low tolerance for frustration and poor impulse control;
- overprotection, linked in some cases to emotional dependence on parents, to the point where the child does not achieve independence and cannot function without parental presence or permission; and
- conflicts over parenting (arguments about parenting in front of the child, divided parental authority, inconsistent enforcement of rules and limits, and even rifts between parents).
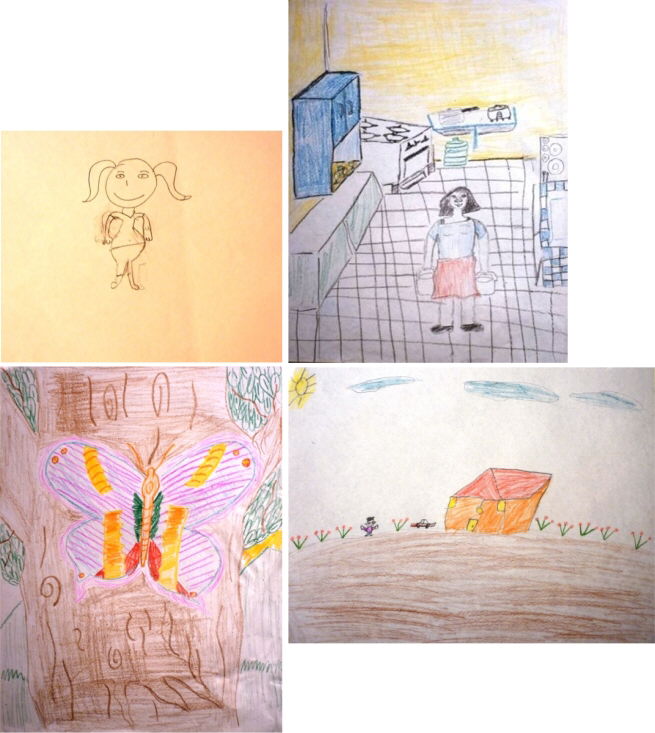
Psychographic analysis of children’s drawings Structural indicators revealed problems with muscle control, which could indicate problems with impulse control; inanimate movement while drawing, indicating probable internal stress and conflict; heavy lines, especially when drawing houses, possibly indicating worry or upset associated with home or family life; and human movement in drawn figures suggested high intellectual, creative and expressive capacity in many of the children.
What stood out among the color indicators, although to a lesser extent, was the orderly color seriation, which could denote mood swings. Color preference tended toward greens and blues, indicating anxiety. The set of indicators related to human figure drawing revealed problems, especially when participants destroyed the drawing in progress, suggesting problems with body image and concept of the human figure. We also observed mutilations (omission of some element of the figure), which could indicate problems with social relations, and incomplete figures (omission of some element of the face), which point to communication problems.
Below we briefly describe examples of drawing analysis according to some of these indicators:
Figure 1 is a self portrait. The most striking element is the subject’s dissatisfaction with her body image; while drawing herself as obese is realistic, the lack of color suggests emotional inhibition with respect to what she is depicting.
In Figure 2 (free drawing), what stands out is the color seriation in the figure of the butterfly, which indicates emotional swings and instability.
In Figure 3 (family portrait) blue and black are the preferred colors, which could indicate latent anxiety and some suggestion of depression. Moreover, most of the family members are left out, including the subject, indicating intrapersonal and interpersonal conflicts in the family, as well as low self-esteem.
Figure 1: Self portrait, girl, 6 years

Figure 2: Free drawing, boy, 14 years

F igure 3: Family portrait, boy, 14 years

Figure 4: Free drawing, girl, 11 years

Figure 4 (free drawing) uses heavy lines depicting the house, which could indicate worry or upset related to the family environment. The colors used to fill in the lines point to aggressiveness (red) and impulsiveness (orange) in this area. Difficulties with muscle control are also evident in both execution of geometric figures and the subject’s ability to color within the lines (expected of a child aged 11 years), which could indicate problems with impulse control.
DISCUSSION
Our results with respect to eating habits are consistent with those from related studies. According to Jiménez, some of the main factors that promote and perpetuate obesity are excessive intake of high-calorie processed foods, reactive psychological disorders in which food holds a pleasurable place, and lack of knowledge about obesity as a disease associated with small imbalances maintained over time, indicating a diminished perception of risk by family members.[15] Our results appear to contradict those of Edo, whose research found no statistically significant differences of eating habits evaluated between obese and non-obese children.[16]
A study in Spain found obesity in children and young people to be more prevalent in those who obtained a higher proportion of calories from fats, and in those with diets rich in sugary foods, baked goods, processed meats and soft drinks.[17] Morales also found consumption of high-energy foods to be a determinant of obesity, observing that eating these more than twice a week increased a child’s likelihood of becoming overweight.[18]
There is no doubt that the amount, and almost more importantly, the quality of food consumed are determinants in the development and persistence of excess weight problems in children.
Our results regarding physical activity are consistent with those of Jiménez, who asserts that a sedentary lifestyle and increased time spent watching television, using computers and playing video games are among the main factors in development and persistence of childhood obesity.[15] A much higher prevalence of obesity has been found among children who spend more time engaging in these types of activities than among those who spend less.[4] Likewise, children who regularly participate in sports have a lower prevalence of obesity than those who do not. Tirado, moreover, concludes that excessive television viewing has negative consequences for eating habits and development of obesity and high cholesterol levels.[19] In fact, Morales found that children’s physical inactivity was more influential than their diet on their chances of becoming overweight or obese.[18] Furthermore, Edo concludes that once obesity is established a vicious cycle ensues, in which obese children increasingly prefer passive activities.[16]
Satisfaction with body image has often been investigated in studies such as those of Galache, who suggests that obese children have a greater propensity to have a distorted body image, with high levels of anxiety, depression, and low self-esteem.[3] Similarly, Fuillerat contends that one of the factors most associated with obesity is body image, which decidedly affects self-esteem and, if impaired, results in negativity and avoidance of social activities and those in which displaying or using one’s body is important, as in sports and cultural performances.[20] Calderón concludes that obese children are more concerned about their physical appearance and social environment, have greater body awareness and experience more subjective stress.[5] In line with most of the studies we reviewed, Ortega found obese children have poor self-images and express feelings of inferiority and rejection.[21]
Findings regarding children’s emotional state vary. In this regard, we agree with Calderón, who posits that as body mass index increases, so do eating disorders and symptoms of anxiety.[5]
Chueca states that discrimination by adults or peers triggers in these children antisocial attitudes that lead to isolation, depression and inactivity; this often results in greater food intake, which in turn exacerbates, or at least perpetuates, their obesity.[22] Fuillerat found a relationship between family dysfunction and childhood obesity.[20] Bruss likewise reported that family conflicts can lead to poor eating habits and hence, obesity.[11]
We concur with Gussinyé, who asserts that family structures, parental lifestyle, the quality of the parent–child relationship, and family support have a significant impact on children’s eating habits, preferences and physical activity.[6] Concerning the issue of overprotection, Gussinyé states that when mothers, who usually have the closest relationship with the child, surround him or her with overly anxious care, offering food in such abundance that it not only fulfills a natural need but becomes something of considerable emotional value, then food becomes the mother’s way of expressing affection and allaying guilt, and for the child a means of soothing anxiety.
There has been some controversy in the scientific literature about the validity of projective techniques such as drawings and sentence completion, which may be considered by some to be a study limitation.[23] These techniques are widely used in clinical psychology to explore emotions, experiences, memories and imaginings; they are not substitutes for expert psychological assessment. We did not depend on a single mode of assessment, but triangulated results from projective techniques and interviews to obtain a more robust sense of the children’s and adolescents’ emotional states.
Given their virtually absolute dependence on adults, children—especially younger ones—are the most vulnerable group in the population. It is adults—family and those in the broader society who make decisions affecting their environments—who determine how the young live (physical activity, leisure, food) and who are responsible for their acquiring healthy or unhealthy habits.[18] Jódar asserted that parents play a vital role in setting guidelines that prevent development of obesity in young children.[24] This suggests that efforts be made to convince adults that a “chubby” child is not a healthier child, and that parental childrearing obligations include instilling and maintaining healthy habits in their children. And, to create public policy that supports healthy choices by both parents and children.
CONCLUSIONS
The majority of obese children and their families exhibit psychological, behavioral and familial traits that foster development and perpetuation of obesity. This is a first diagnostic stage that will aid in design and implementation of a psychological intervention program for obese children and their families.