INTRODUCTION Polyserositis is described as inflammation with effusion of more than one serous membrane. There is very little published literature linking it to COVID-19 as a late complication.
OBJECTIVES Present and describe a case of post–COVID-19 polyserositis.
METHODS Data were collected from the medical record of a female patient admitted for fainting spells and marked weakness. The patient underwent a clinical evaluation, additional hematology, imaging and histopathology tests, and a surgical procedure.
The new index, called the abdominal adipose deposit index, was obtained by multiplying the subcutaneous fat thickness by visceral fat thickness, both measured by ultrasound. A cutoff point was established that facilitated discernment of an unhealthy phenotype: normal weight but metabolically obese, a cardiometabolic risk factor.
RESULTS We present the case of a 57-year-old female patient admitted to hospital for fainting spells and marked weakness, four months after COVID-19 infection. She also had a history of obesity, asthma, type 2 diabetes mellitus and a cholecystectomy in December 1992 for gallstones. Clinical assessment revealed pericardial effusion and bilateral pleural effusion, in addition to a tumor-like lesion outside the pericardium, proximal to the right ventricular wall. A surgical procedure and findings from additional tests led to diagnoses of thymic remnants and polyserositis.
CONCLUSIONS This is a case of polyserositis in a post–COVID-19 patient. After other causes of polyserositis were ruled out, and since there is a likely physiological and pathogenic mechanism operating between the two diseases, the polyserositis was determined to be a late complication of COVID-19. To date, it is the second case reported in the world and the first reported in Cuba.
ABSTRACT INTRODUCTION Polyserositis is described as inflammation with effusion of more than one serous membrane. There is very little published literature linking it to COVID-19 as a late complication.
OBJECTIVE Present and describe a case of post–COVID-19 polyserositis.
METHODS Data were collected from the medical record of a female patient admitted for fainting spells and marked weakness. The patient underwent a clinical evaluation, additional hematology, imaging and histopathology tests, and a surgical procedure.
RESULTS We present the case of a 57-year-old female patient admitted to hospital for fainting spells and marked weakness, four months after COVID-19 infection. She also had a history of obesity, asthma, type 2 diabetes mellitus and a cholecystectomy in December 1992 for gallstones. Clinical assessment revealed pericardial effusion and bilateral pleural effusion, in addition to a tumor-like lesion outside the pericardium, proximal to the right ventricular wall. A surgical procedure and findings from additional tests led to diagnoses of thymic remnants and polyserositis.
CONCLUSIONS This is a case of polyserositis in a post–COVID-19 patient. After other causes of polyserositis were ruled out, and since there is a likely physiological and pathogenic mechanism operating between the two diseases, the polyserositis was determined to be a late complication of COVID-19. To date, it is the second case reported in the world and the first reported in Cuba.
INTRODUCTION COVID-19 has presented extraordinary global challenges in virtually all aspects of public and private life, prompting continuing debate and research.[1] On the medical front, complications of this viral infection have included reports of isolated inflammation of the pericardium, pleura and peritoneum.[2–4]
The medical community has also focused on the persistent symptoms identified after resolution of acute COVID-19. These symptoms have been called by different names: post-COVID conditions, long COVID, and post-acute COVID syndrome. Most of these descriptions involve onset of symptoms one to three months after the patient recovers from acute infection.[5,6]
After reviewing acute and late COVID-19 conditions, we found very few reports of polyserositis in adults not attributable to another comorbidity.
The objective of this report was to present and describe a case of post–COVID-19 polyserositis—the first in Cuba and the second in the world considered as a post–COVID-19 complication.[7]
METHODS The patient’s medical record included data collected from the patient interview, the physical exam, additional blood and imaging test results and surgeries, as well as the histopathology test of pleural and pericardial fluid samples and tissue bordering the pericardium. All research was conducted by technicians and professionals in laboratories and hospital departments, following good clinical and laboratory practices.
IMPORTANCE This case of polyserositis as a post–COVID-19 complication is the second case reported in the world and the first in Cuba.
We searched the Scielo, MedCarib, PubMed, LiLacs, and Google Scholar databases for previous reports of polyserositis as a post–COVID-19 complication.
We also conducted an interdisciplinary review of the case.
Ethics The patient voluntarily provided her written informed consent to be studied for her health condition, as part of her healthcare regimen. We took special care to respect the patient’s privacy and anonymity and ensured the integrity and accuracy of the data disclosed.
RESULTS This is the case of a 57-year-old female patient with obesity (body mass index 34.4 kg/m2), a history of bronchial asthma and a 10-year history of type 2 diabetes mellitus regularly controlled with oral hypoglycemic agents. The patient underwent a cholecystectomy in December 1992 for gallstones.
In July 2021, the patient completed her SARS-CoV-2 vaccination series with three doses of Abdala, a Cuban COVID-19 vaccine. On September 15, 2021, she received a diagnosis of COVID-19; she had a mild case, and recovered quickly.
She was admitted to the Medical-Surgical Research Center (CIMEQ), in Havana, Cuba, on January 25, 2022, for fainting spells and sweating that started approximately two weeks before admission, with progressive worsening in intensity and frequency. The spells were accompanied by noticeable weakness.
In the interview, the patient reported dyspnea on moderate physical exertion and when attempting supine position.
Physical examination revealed decreased vesicular breath sounds in both lung bases, rhythmic and somewhat muffled heart sounds, heart rate at 80 beats per minute, blood pressure (in the right arm) at 110/70 mmHg and soft and rounded abdomen. The rest of the physical examination was normal.
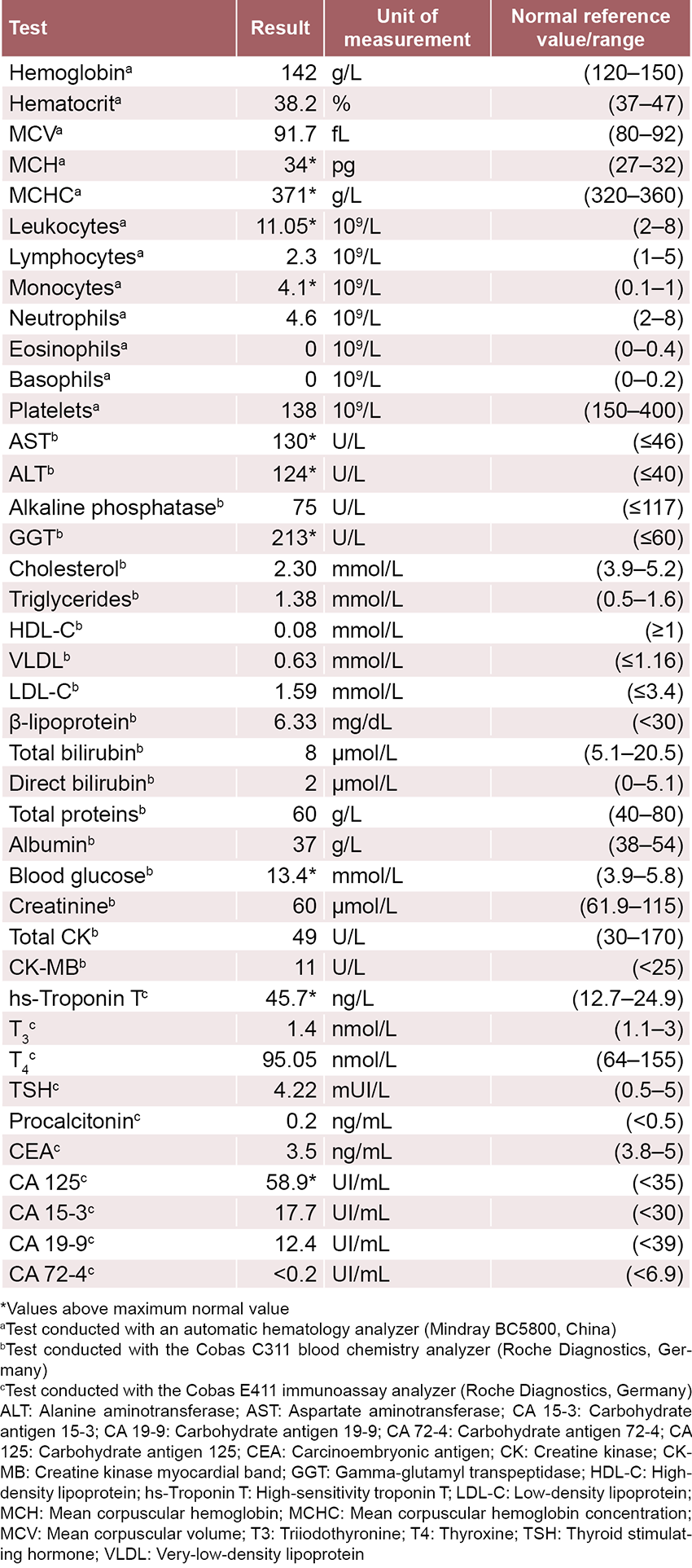
Additional tests showed abnormally high blood glucose (>20 mmol/L), requiring a change in diabetes treatment (discontinuation of oral hypoglycemic agents in favor of insulin), which brought the symptoms under control. Laboratory tests also revealed high levels of high-sensitivity troponin T, aspartate aminotransferase, alanine aminotransferase and gamma-glutamyl transpeptidase. The results of the remaining blood tests were unremarkable (Table 1).
The electrocardiogram was normal.
Table 1: Results of additional laboratory tests performed at hospital admission
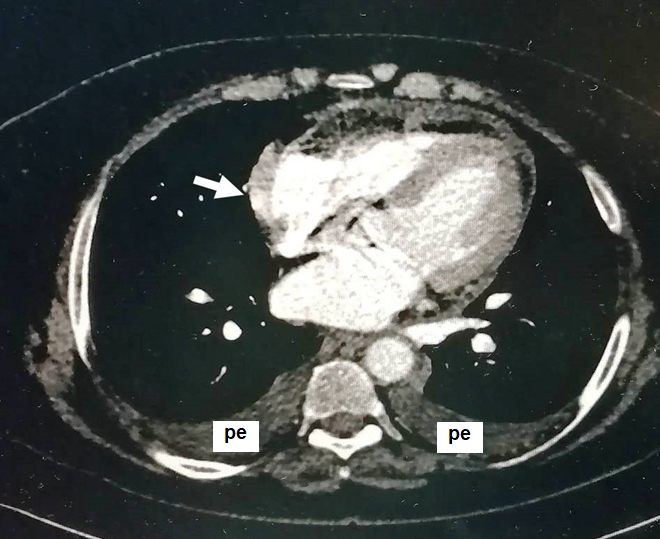
Figure 1: Axial slice of heart CT scan during arterial phase
CT: computed tomography; pe: pleural effusion
The arrow points to the contrast-enhanced lesion projected out from the pericardium, with oval appearance, located in close contact with the outer border of the right atrium. The study was conducted with a 128-slice SOMATOM Definition AS scanner (Siemens, Germany).
Other findings were as follows:
Abdominal ultrasound The liver had increased echogenicity due to steatosis; both kidneys were normal; the pancreas was normal; the uterus was small and involuted with thin endometrial lining; and a small amount of fluid was found at the bottom of the pouch of Douglas.
Computed tomography (CT) The noncontrast study showed pericardial thickening on the outer border of the right atrium, pericardial effusion and bilateral pleural effusion, more evident on the right side. There was no mediastinal lymphadenopathy. The liver showed uniform density. A small amount of fluid was observed in the bottom of the pouch of Douglas. The spleen measured 128 mm. Kidneys were normal in appearance, without stones. The pancreas was normal. There was no retroperitoneal lymphadenopathy. There were incipient degenerative changes in the lumbosacral spine.
Transthoracic echocardiogram (TTE) Valve apparatuses were normal. The right atrium and right ventricle were collapsed due to effusion. The echocardiogram identified a tumor, proximal to the right atrium, which seemed to be attached to the pericardium, but could not be further pinpointed with this study.
Contrasted heart CT The arterial phase showed a hyperdense lesion measuring 1.7 x 4.3 cm, oval in shape, enhanced with a contrast agent, located in close contact with the outer border of the right atrium (Figure 1). This lesion coincides with the pericardial thickening reported in the noncontrast study.
Thoracoscopy Considering the previous findings and especially the tumor-like lesion in the pericardial region, a thoracoscopy was performed to pinpoint whether there were pleural abnormalities and to urgently study the pleural fluid. Slightly cloudy, light-yellow fluid, with fibrin formation and exudate appearance, was collected and analyzed in the pathology department. Malignant neoplasm was ruled out; only isolated lymphocytes were observed.
During the same surgical procedure, a median sternotomy was performed to study the pericardium and remove the lesion reported in the imaging tests. Moderate pericardial effusion was confirmed. The gross characteristics of the pericardial fluid extracted were similar to those described in the pleural fluid.
A lesion with fatty appearance outside the pericardium at the right pericardiophrenic angle was identified and completely removed. A pericardial window was also performed as a therapeutic measure to prevent recurrence of pericardial effusion and to prevent risk of developing cardiac tamponade.
Histopathology A cytopathology test of the pericardial fluid confirmed absence of malignant neoplasm and presence of isolated lymphocytes.
Anatomic pathology report Analysis of the specimen removed during surgery yielded a determination of fibroadipose tissue with Hassall’s corpuscles, leading to the conclusion that this tissue was related to thymic remnants and that this condition is not associated with development of pericardial effusion in this case.[8]
Followup The patient recovered quickly and started treatment with colchicine at low doses (0.5 mg every 12 hours). In the followup conducted one month after the procedure, the patient did not have pleural or pericardial effusion, and she maintained normal cardiac function and diabetes control.
Final diagnosis The patient received a diagnosis of polyserositis, possibly as part of a post–COVID-19 complication.
DISCUSSION The imaging finding of a pericardial lesion with pericardial effusion, along with manifestations of right ventricular failure, led to several possible diagnoses.
Pericardial conditions are variable in clinical practice and may occur as an isolated process or associated with certain systemic conditions. Different benign or malignant diseases can also be established in the pericardium.[9,10]
Initial identification of a pericardial mass, with the aid of TTE and CT, led to different presumptive diagnoses. First, pericardial metastases had to be considered because they are the most common malignant neoplasms of the pericardium.
The most common metastases are those from malignant lung, breast and kidney tumors.[10] Primary pericardial neoplasms are extremely rare. Mesothelioma is the most frequent, followed by fibrosarcomas and other types of sarcomas, lymphomas, neuroectodermal tumors and other benign lesions such as lymphangiomas, hemoangiomas, teratomas, neurofibromas and lipomas.[10] For these reasons, doctors initially turned to a thoracoscopy to evaluate the nature of the pleural effusions and rule out a malignant pleural effusion.[11]
Identifying fatty-like tissue bordering the pericardium with thymic remnants fully ruled out the primary nature of a pericardial lesion, as well as a primary or metastatic malignant lesion. While it may be an uncommon finding, thymic remnants are present in more than half of adults.[12]
After ruling out thymic remnants and neoplastic, infectious and autoimmune diseases as plausible causes for polyserositis in this case, a diagnosis of polyserositis associated with COVID-19 was proposed, a condition that to date has been reported in only one case in a scientific publication.[7] Nevertheless, the characteristics of the pleural and pericardial fluids (exudate) and the high levels of high-sensitivity troponin T support such a diagnosis. Evidence has also emerged indicating that SARS-CoV-2 can cause direct damage to the heart, either affecting the myocardium (myocarditis) or the pericardium (pericarditis).[13]
Polyserositis is a condition characterized by inflammation and effusion in more than one site, including the pericardium, pleura and the peritoneum. Because of the rarity of polyserositis in medical practice, the diagnosis is based on clinical recognition and subsequent screening of probable causes.[9] It has been suggested that polyserositis onset in these patients occurs as a result of immunological phenomena caused by COVID-19, characterized by a disregulated cytokine and chemokine production.[14]
Experience using colchicine to treat acute pericarditis and prevent recurrences indicates that this drug is safe for patients with COVID-19 and can be used during the early phases of the disease and for complications such as pericarditis and pleuritis.[15,16] The previous report of polyserositis as a post-COVID complication also documented successful treatment with colchicine.[7]
CONCLUSION This report described a patient with clinical symptoms consistent with post–COVID-19 polyserositis, which occurred three months after infection by SARS-CoV-2. While it is not possible to establish a definitive causal relationship between polyserositis and history of COVID-19, this link cannot be ignored, especially after ruling out other possible causes of polyserositis and finding a plausible physiological and pathological mechanism between these two diseases. Thus, the studies conducted in this patient led us to conclude that polyserositis may be a late complication of COVID-19. This case is the second reported in the world and the first in Cuba describing such a nosological association.
Pillai A, Lawson B. Coronavirus disease 2019 and cardiovascular diseases: collateral damage? Curr Opin Anesthesiol. 2022 Feb 1;35(1):5–11. https://doi.org/10.1097/aco.0000000000001076
Oleynick C. Symptoms of pleurisy as the initial presentation of COVID-19. Am J Case Rep. 2020 Jul 24;21:e925775. https://doi.org/10.12659/ajcr.925775
Ucan B, Kaynak Sahap S, Cinar HG, Tasci Yildiz Y, Uner C, Polat M, et al. Multisystem inflammatory syndrome in children associated with SARS-CoV-2: extracardiac radiological findings. Br J Radiol. 2022 Jan 1;95(1129):20210570. https://doi.org/10.1259/bjr.20210570
Boix V, Merino E. Síndrome post-COVID. El desafío continúa [Post-COVID syndrome. The never ending challenge]. Med Clin (Barc). 2022 Feb 25;158(4):178–80. Epub 2021 Dec 2. https://doi.org/10.1016/j.medcli.2021.10.002. Spanish, English.
Messin L, Puyraveau M, Benabdallah Y, Lepiller Q, Gendrin V, Zayet S, et al. COVEVOL: Natural evolution at 6 months of COVID-19. Viruses. 2021 Oct 25;13(11):2151. https://doi.org/10.3390/v13112151
Harris E, Shanghavi S, Viner T. Polyserositis secondary to COVID-19: the diagnostic dilemma. BMJ Case Rep. 2021 Sep 27;14(9):e243880. https://doi.org/10.1136/bcr-2021-243880
Klimek-Piotrowska W, Mizia E, Kużdżał J, Lazar A, Lis M, Pankowski J. Ectopic thymic tissue in the mediastinum: limitations for the operative treatment of myasthenia gravis†. Eur J Cardiothorac Surg. 2012 Jul 1;42(1):61–5. https://doi.org/10.1093/ejcts/ezr268
Losada I, González-Moreno J, Roda N, Ventayol L, Borjas Y, Domínguez FJ, et al. Polyserositis: a diagnostic challenge. Intern Med J. 2018 Aug;48(8):982–7. https://doi.org/10.1111/imj.13966
Wu Y-B, Xu L-L, Wang X-J, Wang Z, Zhang J, Tong Z-H, et al. Diagnostic value of medical thoracoscopy in malignant pleural effusion. BMC Pulm Med. 2017 Aug 4;17(1):109. https://doi.org/10.1186/s12890-017-0451-1
Mizia E, Klimek-Piotrowska W, Kużdżał J, Konopka T, Lis M, Pankowski J, et al. Residua of thymus in the mediastinum – clinical aspects – cadaveric study. Folia Med Cracov [Internet]. 2017 [cited 2022 Feb 7];LVII(1):23–8. Available at: http://wwwfmc.cm-uj.krakow.pl/pdf/57_1_23.pdf
Piccioni A, Brigida M, Loria V, Zanza C, Longhitano Y, Zaccaria R, et al. Role of troponin in COVID-19 pandemic: a review of literature. Eur Rev Med Pharmacol Sci. 2020 Oct;24(19):10293–300. https://doi.org/10.26355/eurrev_202010_23254
Rodríguez Y, Novelli L, Rojas M, De Santis M, Acosta-Ampudia Y, Monsalve DM, et al. Autoinflammatory and autoimmune conditions at the crossroad of COVID-19. J Autoimmun. 2020 Nov;114:102506. https://doi.org/10.1016/j.jaut.2020.102506
Furqan MM, Verma BR, Cremer PC, Imazio M, Klein AL. Pericardial diseases in COVID19: a contemporary review. Curr Cardiol Rep. 2021 Jun 3;23(7):90. https://doi.org/10.1007/s11886-021-01519-x
Deftereos SG, Giannopoulos G, Vrachatis DA, Siasos GD, Giotaki SG, Gargalianos P, et al. Effect of colchicine vs standard care on cardiac and inflammatory biomarkers and clinical outcomes in patients hospitalized with Coronavirus Disease 2019: the GRECCO-19 randomized clinical trial. JAMA Netw Open. 2020 Jun 1;3(6):e2013136. https://doi.org/10.1001/jamanetworkopen.2020.13136
THE AUTHORS
Julio César Hernández-Perera (Corresponding author: julio.hernandez@infomed.sld.cu), internist with a doctorate in medical sciences. Senior researcher, Medical-Surgical Research Center (CIMEQ), Havana, Cuba. Full professor, Medical University of Havana (UCMH), Cuba. https://orcid.org/0000-0002-8567-5642
Dania Piñeiro-Pérez, general surgeon. Assistant researcher, CIMEQ, Havana, Cuba and assistant professor, UCMH, Cuba. https://orcid.org/0000-0002-5150-2719
Juan Oscar Martínez-Muñiz, general and cardiovascular surgeon, with a master’s degree in emergency medicine, CIMEQ, Havana, Cuba. Assistant professor, UCMH, Cuba. https://orcid.org/0000-0003-1529-6871
Jorge Miguel Correa-Padilla, physician with dual specialties in family medicine and anesthesiology and resuscitation, with a master’s degree in emergency medicine, CIMEQ, Havana, Cuba. Assistant professor, UCMH, Cuba. https://orcid.org/0000-0001-8732-3635
María Caridad de Armas-Fernández, pathologist with a master’s degree in cytopathology, CIMEQ, Havana, Cuba. Assistant professor, UCMH, Cuba. https://orcid.org/0000-0003-0785-0908
José Antonio Jordán-González, specialist in imaging, with a doctorate in medical sciences, CIMEQ, Havana, Cuba. Assistant professor, UCMH, Cuba. https://orcid.org/0000-0003-3610-0954
Submitted: March 01, 2022 Approved: August 07, 2022 Disclosures: None
Loading...
Loading...
Related articles
From the Editors ►
Early Online
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.