INTRODUCTION In Cuba, 29,939 deaths from ischemic heart disease were recorded in 2020. Myocardial revascularization surgery and percutaneous coronary intervention are well-established methods of treating patients with multivessel coronary artery disease. These methods can reduce overall deaths, but choosing the optimal strategy for treating left main coronary ischemia is a source of debate among specialists.
OBJECTIVE Estimate survival and major cardiac and cerebrovascular events in patients treated with percutaneous coronary intervention versus myocardial revascularization surgery and their relationships with pre-existing patients’ clinical and angiographic characteristics.
METHODS We conducted a retrospective cohort study in 41 patients; 35 men and 6 women aged 40–85 years who had been diagnosed with multivessel coronary artery disease and treated with percutaneous coronary intervention (n = 17) or myocardial revascularization surgery (n = 24) at the Medical–Surgical Research Center in Havana, Cuba, in 2016. The main variable under consideration was the occurrence of major adverse cardiovascular events over a four-year period following these interventions. We collected clinical and angiographic characteristics, and used the Kaplan–Meier test to calculate survival curves. Survival probabilities were compared using the log-rank test. A value of p <0.05 was considered statistically significant. The Cox proportional hazards model was used to estimate the hazard ratio, with 95% confidence intervals used for both procedures.
RESULTS There were a total of 20 major adverse cardiovascular events, 75% (15/20) of which occurred in patients who underwent percutaneous coronary intervention and 5% in patients who had myocardial revascularization surgery. The probability of survival was 70.6% in surgery and 37.5% in interventionism; p = 0.043; hazard ratio 1.58 (95% confidence interval 0.987–2.530), p = 0.047. The need to repeat a revascularization procedure was the only major cardiovascular event that showed significant differences between methods (log-rank p = 0.015), and was more frequent in percutaneous intervention.
CONCLUSIONS Myocardial revascularization surgery offers a better chance of survival than percutaneous coronary intervention. Major adverse cardiovascular events are more frequent in patients with coronary interventionism, due to the need to repeat revascularization.
KEYWORDS Coronary disease, myocardial revascularization, coronary artery bypass, angioplasty, Cuba
ABSTRACT INTRODUCTION In Cuba, 29,939 deaths from ischemic heart disease were recorded in 2020. Myocardial revascularization surgery and percutaneous coronary intervention are well-established methods of treating patients with multivessel coronary artery disease. These methods can reduce overall deaths, but choosing the optimal strategy for treating left main coronary ischemia is a source of debate among specialists.
OBJECTIVE Estimate survival and major cardiac and cerebrovascular events in patients treated with percutaneous coronary intervention versus myocardial revascularization surgery and their relationships with pre-existing patients’ clinical and angiographic characteristics.
METHODS We conducted a retrospective cohort study in 41 patients; 35 men and 6 women aged 40–85 years who had been diagnosed with multivessel coronary artery disease and treated with percutaneous coronary intervention (n = 17) or myocardial revascularization surgery (n = 24) at the Medical–Surgical Research Center in Havana, Cuba, in 2016. The main variable under consideration was the occurrence of major adverse cardiovascular events over a four-year period following these interventions. We collected clinical and angiographic characteristics, and used the Kaplan–Meier test to calculate survival curves. Survival probabilities were compared using the log-rank test. A value of p <0.05 was considered statistically significant. The Cox proportional hazards model was used to estimate the hazard ratio, with 95% confidence intervals used for both procedures.
RESULTS There were a total of 20 major adverse cardiovascular events, 75% (15/20) of which occurred in patients who underwent percutaneous coronary intervention and 5% in patients who had myocardial revascularization surgery. The probability of survival was 70.6% in surgery and 37.5% in interventionism; p = 0.043; hazard ratio 1.58 (95% confidence interval 0.987–2.530), p = 0.047. The need to repeat a revascularization procedure was the only major cardiovascular event that showed significant differences between methods (log-rank p = 0.015), and was more frequent in percutaneous intervention.
CONCLUSIONS Myocardial revascularization surgery offers a better chance of survival than percutaneous coronary intervention. Major adverse cardiovascular events are more frequent in patients with coronary interventionism, due to the need to repeat revascularization.
KEYWORDS Coronary disease, myocardial revascularization, coronary artery bypass, angioplasty, Cuba
INTRODUCTION In Cuba, 29,939 people died in 2020 from heart disease, at a rate of 267.3 per 100,000 population. Of these, 18,572 died from ischemic-type diseases.[1] Among ischemic heart diseases, multivessel coronary artery disease is a heterogenous group, due to its anatomical and functional complexity. This requires a similarly complex approach to treatment that focuses on each patient’s individual characteristics when choosing the best available therapeutic strategy.
Myocardial revascularization surgery (MRS) or percutaneous coronary intervention (PCI) are common methods used in treating these patients, but the ideal method for multivessel coronary artery disease or ischemia of the left main coronary artery (LMCA) is controversial among interventional cardiologists and cardiovascular surgeons. Although clinical practice guidelines lean toward MRS, decisions on treatment options changed for many patients after PCI was introduced.[2]
IMPORTANCE This paper provides information on survival rates and complications following percutaneous coronary intervention and myocardial revascularization surgery over four years comparing these procedures. This may help determine the optimal revascularization strategy for patients with multivessel coronary artery disease.
The Cuban cardiocenter network practices both revascularization methods, but few reports are available on long-term survival for the two procedures. We set out to estimate survival and major adverse cardiac and vascular events (MACE) in patients treated with PCI or MRS, and the relationships these events have with patients’ clinical and angiographic characteristics prior to both procedures.
METHODS Study type and sampling We carried out a cohort study in 41 patients; 35 men and 6 women aged 40–85 years, who were diagnosed with either three-vessel coronary artery disease or LMCA, treated with percutaneous coronary intervention (n = 17) or myocardial revascularization surgery (n = 24) at the Medical–Surgical Research Center (CIMEQ) in Havana, Cuba, in 2016. MRS was performed in most of the more complex lesions. Patients were followed up for 48 months after PCI or MRS.
Inclusion criteria
Patients undergoing revascularization for the first time with three-vessel arterial disease or LMCA
Patients with stenoses ≥50.0% in vessels 1.5 mm in diameter
Exclusion criteria
Patients who underwent previous interventions (PCI or MRS)
Patients with ST-segment elevation acute myocardial infarction (MI)
Patients with MRS concomitant with other types of cardiac or vascular surgery
PCI patients had either conventional or paclitaxel-eluting stents (a drug limiting growth of scar tissue after stent placement).
The primary focus was MACE, defined as: death from any vascular cause, cerebrovascular events, MI, or the need for repeat revascularization. MI was defined by the fourth universal definition[3] and cerebrovascular disease was defined as a focal neurological deficit lasting >72 hours. Demographic, clinical and angiographic variables were examined. The anatomical complexity of coronary artery disease (CAD) was graded by SYNTAX scoring.[4]
Data were obtained from medical records, MRS operation reports, PCI reports and followup records.
Statistical analysis MACE-free survival curves were constructed using the Kaplan-Meier method. Survival probabilities were compared using the log-rank test. A value of p <0.05 was considered statistically significant. Cox proportional hazards modeling was used to estimate hazard ratios (HR) using 95% confidence intervals (CI), comparing PCI and MRS.
Ethics This research was approved by CIMEQ’s research ethics committee and followed the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from patients before inclusion in the study. Identifying information was kept confidential.
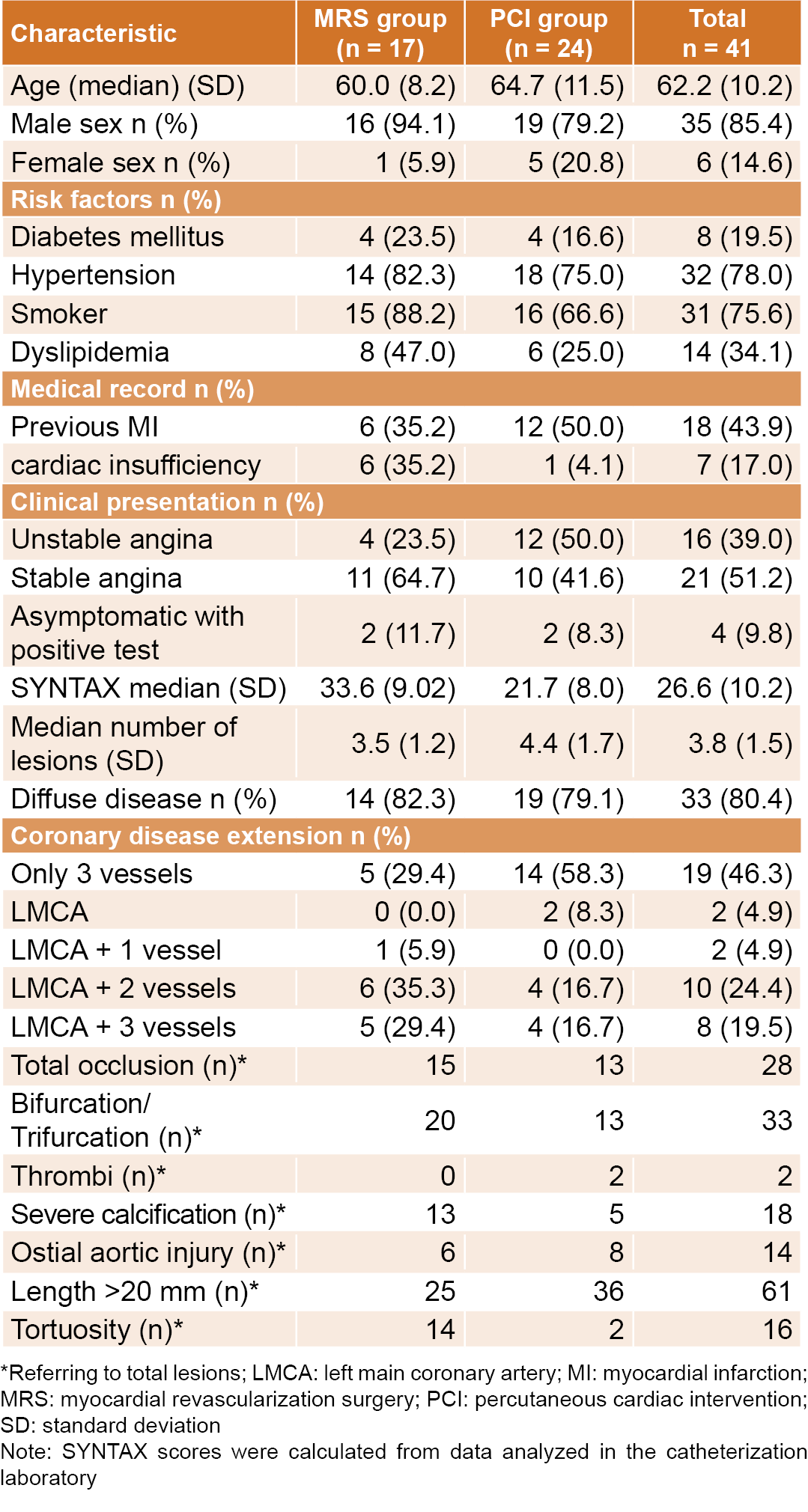
RESULTS Participants’ mean age was 62.2 years; 15% of patients were older than 75. Heart failure prior to revascularization was the only clinical variable that demonstrated a clear association with the chosen procedure. The angiographic variables showing notable differences between groups were total occlusions, bifurcation/trifurcation, severe calcification and tortuosity. The SYNTAX scores were higher in patients with coronary artery bypass grafting (MRS) (Table 1).
Most complex injuries (64.7%) included LMCA plus two or three additional vessels (Table 1).
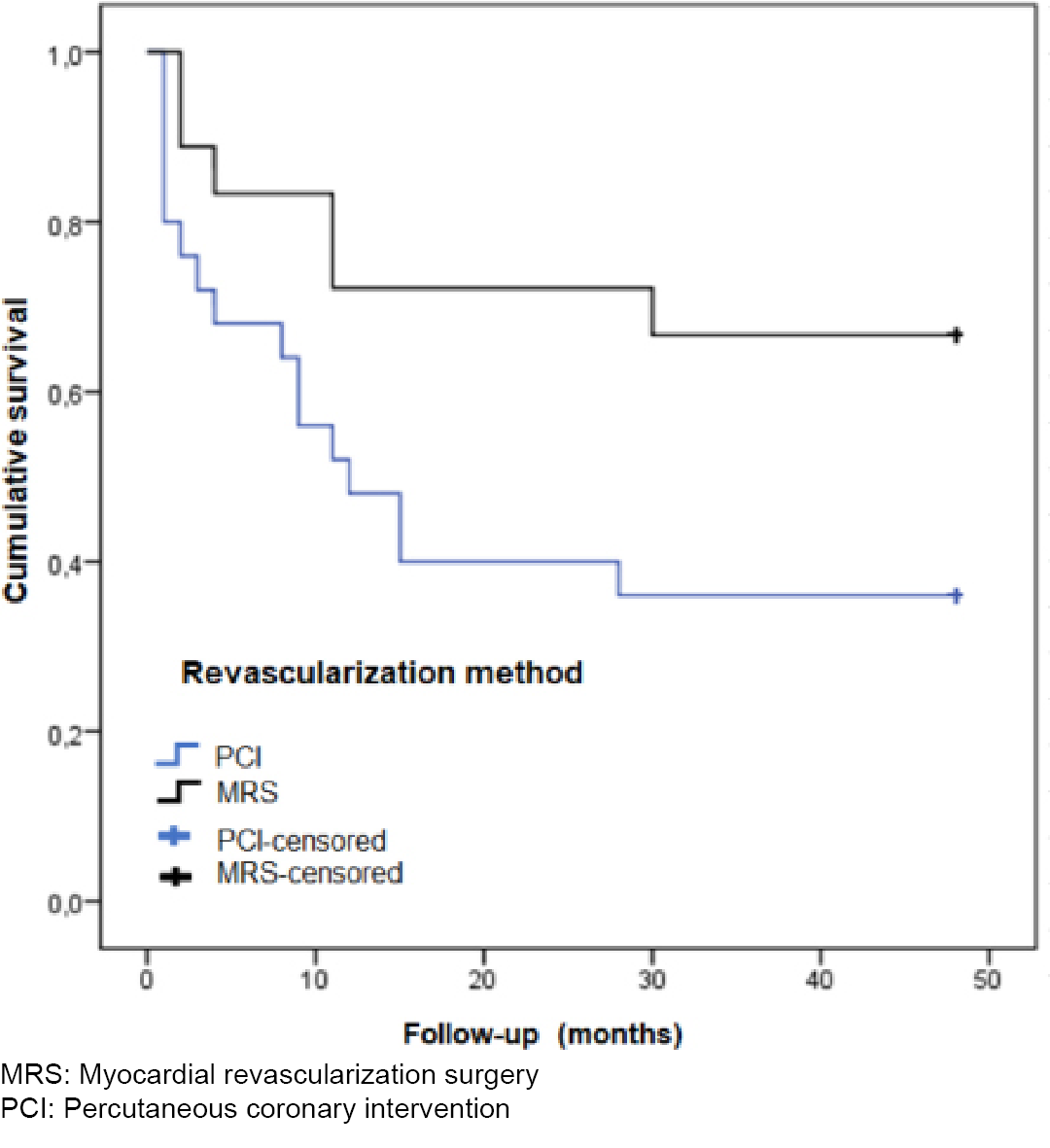
Median followup was 30 months (with an interquartile range of 4–48 months). At the end of the 4-year study period, there were 20 MACE; 75% (15/20) in PCI patients and 25% (5/20) in MRS patients. The probability of survival at the end of the followup period was 70.6% in MRS patients and 37.5% in PCI patients.
In the survival analysis, HR = 1.58 (95% CI: 0.987–2.530) (Figure 1).
Table 1: Baseline clinical and angiographic patient characteristics
In PCI patients, MACE included the need for repeat revascularization (60%; 9/15), death from any cause (26.7%; 4/15) and MI (13.3%; 2/15). In MRS, MACE included death from any cause (40%; 2/5), cerebrovascular disease (40%; 2/5), and the need for repeat revascularization (20%; 1/5).
DISCUSSION Although there are protocols and resources guiding these procedures in high-income countries, there have been no studies in Cuba evaluating long-term results of the two revascularization methods. Accordingly, this study—although limited to Cuba—could prove useful to low- and middle-income countries where PCI has been more accessible.
Since the publication of the SYNTAX study in 2009, attempts have been made to relate pre-existing clinical and angiographic variables to revascularization methods.[5] In the present study, we found an association with age and heart failure. Left ventricular ejection fraction deterioration has been reported as a good independent predictor of death and other major adverse events after revascularization, and particularly surgery. It is common to include this variable in predictive models.[6] In a meta-analysis comparing revascularization methods, Hlatky found age and diabetes mellitus to be associated with the choice of revascularization method.[7]
Figure 1: Myocardial revascularization surgery and percutaneous coronary intervention patient survival
In several studies, angiographic variables showed stronger associations with the revascularization methods than clinical variables.[5,7] Among the angiographic variables associated with revascularization, lesion lengths >20 mm were an exception, which may be due to the fact that this variable is imprecise and exhibits high interobserver variability, as reported by Mohr.[8] These variables seem to have a greater influence on patients treated with PCI, likely related to greater anatomical complexity.
A SYNTAX study with a 5-year followup showed a higher MACE incidence in the PCI group than the MRS group (37.5% vs. 24.2%, p <0.001). Death/acute stroke/MI were higher in the PCI group (22% vs. 15.0% in MRS, p <0.001), with significant differences in all causes of death and in occurrence of angina during followup. The need for repeat revascularization was higher among PCI patients.[9]
The SYNTAX study was the first to evaluate survival after PCI with drug-eluting stents, as compared with MRS. After a 10-year followup period, proportions of all-cause deaths between PCI and MRS were similar. Subgroup analyses showed MRS had significantly fewer all-cause deaths in patients with three-vessel artery disease, but not in patients with LMCA disease.[10]
Occurrence of MACE was less frequent after MRS, mainly due to the need for repeat revascularization in PCI patients, and there were no differences in the categories of MI, death from any cause, or cerebrovascular disease. The difference in the need for repeat revascularization could be due to the type of stent used in PCI, but we did not include this variable in our analysis. A randomized prospective longitudinal study of 318 patients—159 assigned conventional stents and 159 assigned paclitaxel-eluting stents—with a followup of 3 years, concluded that although patients who received paclitaxel-eluting stents had a greater probability of survival, “they evolved similarly in terms of MI incidence, death from any cause, and stent thrombosis.”[11]
The only Cuban study that compares the two strategies in 178 patients (87 PCI and 91 MRS), after a 2-year followup, found higher rates of cardiac mortality and MI in MRS and greater need to repeat revascularization in PCI, and concluded that there were no differences in survival between the two strategies.[12] However, the researchers did not perform a log-rank test for this variable, and the periods of followup and intervention for the two strategies were not simultaneous and this is a potential source of bias.
The main limitation of this study is its quasi-experimental design and the fact that it is based on a retrospective cohort. The typical random assignment of clinical trials is not feasible in this type of study. Other limitations include the lack of stratification by cause of death (as this information was not available), which also limited more rigorous control of confounding variables. We also did not compare the use of conventional stents and drug-eluting stents in PCI patients.
CONCLUSIONS Patients with multivessel coronary artery disease or ischemia of the left main coronary artery have a better chance of survival if they undergo myocardial revascularization surgery than if they undergo percutaneous coronary intervention. The number of major adverse cardio-cerebrovascular events is greater in patients with coronary interventionism, relating to the need for repeat revascularization.
Lee PH, Park H, Lee JS, Lee SW, Lee CW. Meta-analysis comparing the risk of myocardial infarction following coronary artery bypass grafting versus percutaneous coronary intervention in patients with multivessel or left main coronary artery disease. Am J Cardiol [Internet]. 2019 Sep 15 [cited 2021 Jul 3];124(6):842–50. Available at: https://www.ajconline.org/article/S0002-9149(19)30709-X/fulltext
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J [Internet]. 2019 Jan 14 [cited 2021 Jul 6];40(3):237–69. Available at: https://doi.org/10.1093/eurheartj/ehy462
Naranjo-Domínguez N, Aroche Aportela R, Hernández Navas M, Aldama L, Valdés Martín AV, Vitón Castillo AA. Utilidad pronóstica del puntaje SYNTAX en pacientes con enfermedad coronaria multiarterial. Seguimiento de 4 años. Rev Cubana Cardiol Cir Cardiovasc [Internet]. 2021 Jul 1 [cited 2021 Jul 6];27(3):1234. Available at: http://www.revcardiologia.sld.cu/index.php/revcardiologia/article/view/1234. Spanish.
Serruys PW, Morice M-C, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med [Internet]. 2009 Mar 5 [cited 2021 Apr 15];360(10):961–72. Available at: https://doi.org/10.1056/NEJMoa0804626
Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernández AF, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol [Internet]. 2017 Nov 14–21 [cited 2021 Jul 6];70(20):2476–86. Available at: https://www.sciencedirect.com/science/article/pii/S0735109717397619
Hlatky MA, Boothroyd DB, Bravata DM, Boersma E, Booth J, Brooks MM, et al. Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet [Internet]. 2009 Apr 6 [cited 2021 Apr 16];373(9670):1190–7. Available at: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)60552-3/
Mohr FW, Morice M-C, Kappetein AP, Feldman TE, Ståhle E, Colombo A, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year followup of the randomised, clinical SYNTAX trial. Lancet [Internet]. 2013 Feb 23–Mar 1 [cited 2021 Apr 15];381(9867):629–38. Available at: https://www.sciencedirect.com/science/article/pii/S0140673613601415
Naranjo-Domínguez A, Aroche Aportela R, Hernández M, Obregón A, Aldama L. Variabilidad interobservador del Score SYNTAX en pacientes con diagnóstico de enfermedad arterial coronaria multivaso. Rev Cubana Cardiol Cir Cardiovasc [Internet]. 2018 Jun 4 [cited 2021 Jul 6];24(2):141–54. Available at: http://www.revcardiologia.sld.cu/index.php/revcardiologia/article/view/761. Spanish.
Thuijs DJFM, Kappetein AP, Serruys PW, Mohr F-W, Morice M-C, Mack MJ, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year followup of the multicentre randomised controlled SYNTAX trial. Lancet [Internet]. 2019 Oct 12 [cited 2021 Jul 6];394(10206):1325–34. Available at: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)31997-X/fulltext
Aroche Aportela R, Navarro Rodríguez AY, García Orcid RA, Hernández Nava M, Obregón Santos AG, Aldama Pérez L. Efectividad de la intervención coronaria percutánea con stent liberador de paclitaxel frente a stent convencional. Rev Cubana Cardiol Cir Cardiovasc [Internet]. 2020 Jul 1 [cited 2021 Jul 3];26(3):1011. Available at: http://www.revcardiologia.sld.cu/index.php/revcardiologia/article/view/1011. Spanish.
López Ramírez M, Nafeh Abi-Resk M, Leyva Quert A, Gutiérrez Lípez A, Tamargo Barbeito TO, López Ramírez D, et al. Intervencionismo coronario frente a cirugía de revascularización miocárdica en pacientes con enfermedad multivaso. Rev Cubana Cardiol Cir Cardiovasc [Internet]. 2017 Oct 27 [cited 2021 Jul 4];23(3):361–70. Available at: http://revcardiologia.sld.cu/index.php/revcardiologia/article/view/700. Spanish.
THE AUTHORS
Adrián Naranjo-Domínguez (Corresponding author: anaranjod90@gmail.com), cardiologist with a master’s degree in atherosclerosis, Cardiology and Cardiovascular Surgery Institute, Havana, Cuba. https://orcid.org/0000-0003-3852-1218
Ronald Aroche-Aportela, physician with dual specialties in cardiology and family medicine and a doctorate in medical sciences. Associate professor and senior researcher, Medical–Surgical Research Center (CIMEQ), Havana, Cuba. https://orcid.org/0000-0002-8416-7945
Lázaro Isralys Aldama-Pérez, cardiologist with a doctorate in medical sciences. Associate professor and associate researcher, CIMEQ, Havana, Cuba. https://orcid.org/0000-0001-5811-8368
Ricardo Amador García-Hernández, cardiologist with a doctorate in medical sciences. Associate professor and associate researcher, CIMEQ, Havana, Cuba. https://orcid.org/0000-0001-9980-5447
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.