The COVID-19 pandemic has caused notable changes in all areas of our lives. Pandemic-coping strategies include attention and care at various levels, for different people and in various scenarios. Death is one of the most feared consequences of COVID-19 for both patients and their families; for the latter, the grief and adaptation processes to loss require that care for grievers be an important part of the public health response to the COVID-19 pandemic.
Grief from losses due to COVID-19 has distinctive features: it is not anticipatory (with virtually no time or progressive stages to facilitate adaptation to loss); closure or goodbyes are not possible (in-person social support decreases due to distancing to minimize risk of infection); it may affect various close relationships (a relevant predictor of complicated grief); it may imply stigmatization by peers, friends and neighbors; it is preceded by a period of absence of fluid and in-person communication between family members and the hospitalized patient; and those who break the news of the death are often professionals in red zones who are stressed and do not always have the skills or the ability to properly communicate bad news.
The death of a family member from COVID-19 generally causes an unexpected crisis in the family, which is already affected by the pandemic and its daily consequences. This has prompted an analysis of COVID-19 loss on family life and how best to mitigate its consequences.
During the COVID-19 pandemic, care and monitoring of the grief of family members and those who were close to the deceased require psychological action within a framework of comprehensive care, which demands preparation of healthcare professionals. Experiences described are taken from some actions developed in Cuba.
KEYWORDS Grief, psychology, death, attitude to death, COVID-19, SARS-CoV-2, Cuba
ABSTRACT The COVID-19 pandemic has caused notable changes in all areas of our lives. Pandemic-coping strategies include attention and care at various levels, for different people and in various scenarios. Death is one of the most feared consequences of COVID-19 for both patients and their families; for the latter, the grief and adaptation processes to loss require that care for grievers be an important part of the public health response to the COVID-19 pandemic.
Grief from losses due to COVID-19 has distinctive features: it is not anticipatory (with virtually no time or progressive stages to facilitate adaptation to loss); closure or goodbyes are not possible (in-person social support decreases due to distancing to minimize risk of infection); it may affect various close relationships (a relevant predictor of complicated grief); it may imply stigmatization by peers, friends and neighbors; it is preceded by a period of absence of fluid and in-person communication between family members and the hospitalized patient; and those who break the news of the death are often professionals in red zones who are stressed and do not always have the skills or the ability to properly communicate bad news.
The death of a family member from COVID-19 generally causes an unexpected crisis in the family, which is already affected by the pandemic and its daily consequences. This has prompted an analysis of COVID-19 loss on family life and how best to mitigate its consequences.
During the COVID-19 pandemic, care and monitoring of the grief of family members and those who were close to the deceased require psychological action within a framework of comprehensive care, which demands preparation of healthcare professionals. Experiences described are taken from some actions developed in Cuba.
KEYWORDSGrief, psychology, death, attitude to death, COVID-19, SARS-CoV-2, Cuba
INTRODUCTION The pandemic caused by SARS-CoV-2 has led to changes in all areas of our lives, with important consequences that require development of various adaptation strategies, including those that help us grapple with the emotional and psychological repercussions. Perhaps the most terrifying personal aspect of the pandemic—besides our own death—is the loss of family members and other loved ones. By the time of this writing—end of October 2021—244 million people had suffered from the coronavirus worldwide, of whom nearly 5 million had died, and both cases and deaths were on the rise.[1]
On the individual level, COVID-19 has caused substantial changes at one of the most difficult times in any life: saying goodbye to a loved one. The special circumstances surrounding the adaptation processes to these losses may become a risk factor hindering a normal grieving process, and must therefore be examined and prioritized. This is not a simple task; it demands extreme delicacy and competence. It requires training, communications skills and willingness on the part of health professionals, to support readjustments to family life. At the same time, it is increasingly becoming a real public health problem. There are no known long-term studies that determine the proportion of normal grief or complicated grief due to COVID-19.
IMPORTANCE Grief monitoring and management for people who lost a loved one to COVID-19 is a public health problem that is now of particular importance. This paper describes grief manifestations and the care recommended in the pandemic context. Some Cuban experiences in this field are described. It also comments on the need to prepare health professionals for such urgent patient care, to which psychologists can and should be important contributors.
This paper presents our understanding of grief among people who have lost family members to COVID-19, with recommendations for managing their care, including evaluation, monitoring, support and counseling as part of a comprehensive approach to therapy. Experiences in Cuba serve as point of reference, including initial actions taken to address grief-stricken families and loved ones.
DEVELOPMENT Grief as a loss adaptation process and distinctive features of COVID-19 grief The process that ensues after a significant loss, aimed at restructuring life around acceptance of that loss, is known as ‘grief.’[2,3] During the COVID-19 pandemic, losses may be of a diverse nature; some may be temporary; others permanent. Many of us have experienced the most painful loss: the death of a family member, friend or other close relationship.
In general, loss of a loved one engenders a normal adaptive process with a beginning and an end; it is often long and painful, which involves undoing, little by little, ties with the loved one, while keeping his or her image present in our inner world.[2−4]
There are three main components of grief: 1) feelings of sorrow, suffering and internal pain, without which grief cannot be resolved; 2) longing and nostalgia due to the physical absence
of the deceased person; and 3) expressive behaviors of loss (i.e. mourning, the forms of which have changed throughout history and depend on cultures and personal characteristics).[2−6]
The latest glossaries for classifying mental disorders define grief as disposed to receiving medical attention, as it may cause symptoms similar to depression and other conditions.[7] That is, while there is consensus that grief is not an illness, if it progresses to ‘complicated grief,’ it becomes a risk factor for illness. Obviously, the line differentiating normal grief from complicated grief requires clear diagnosis criteria that allow for timely decision-making and intervention.[3,8]
Prevalence estimates for complicated grief vary among different populations and can be influenced by culture, age and other factors (involving such situations as death of a close relative, prevalence of certain chronic conditions in the close space a given country or territory, personal capacity to make sense of the loss, attitudes and beliefs concerning death, critical scenario competencies and personal ability to handle emotions, degree of self-care, sentiments of guilt, unresolved mourning from past losses, etc.).[8]
For example, Jacobs estimated complicated grief at 10%−20% of grievers;[9] Bonnano and Kaltman, 15%;[10] and Maercker found a prevalence of just 7.4% in older persons.[11] Thus, according to these and other classic studies, grief follows a normal course in >70% of cases, requiring only monitoring and support. In <30% of cases it becomes complicated grief, when it lasts many years and the griever is incapable of social reintegration, or when the griever acquires pathological characteristics, with extreme nervous strain, excessive identification with the deceased, drug addiction or risk of suicide, all conditions requiring therapeutic management.[3,5,6,8,12]
There are no reliable estimates regarding the relative frequency of normal and complicated processes in grievers due to COVID-19. If each deceased person left an average of five grieving individuals, and of these, 15% had complicated grief, by the end of October 2021, there would be millions of people experiencing complicated grief worldwide, with their numbers increasing over time.
Certain vulnerability factors are linked to the risk of complicated grief: the bereaved’s connection with the death (intensity, ambivalence, emotional dependence); emotions and their expressions (anger, blame, inability to express emotions); the illness and its characteristics (speed of progression, delay in diagnosis, knowledge of the family member’s prognosis, duration of care); uncontrolled symptoms such as anxiety, chest pain, nausea, rage, emotional lability, dysthymia or other depressive states; personal medical history; unresolved previous grief; financial problems; presence of children and/or disabled individuals in the family; and lack of family support.
There are also protective factors that comprise a resilient or ‘hardy’ personality that include self-control mechanisms (such as meditation, deep-breathing exercises), ability to handle emotions, perception of stressors as challenges rather than catastrophes, positive attitude towards life and the world, and marked spirituality, among others. Protective factors can also be influenced by interpretations and beliefs (religious beliefs, confidence in recovery, ability to find meaning in what happened, sense of purpose in the care of the patient); and attitudes and skills in managing various situations (ability to plan in the face of difficulties and consider alternatives, ability to communicate and carry out self-care, ability to feel positive emotions and plan enjoyable activities).[3,8] These factors play a large part in the grieving process, its duration and prospects for recovery.
Various studies indicate that any grief passes through stages lasting between one and two years, but there is no consensus in this regard. Most people go through an ‘early’ stage that lasts 3–6 months and then a ‘late’ stage that lasts up to 12–18 months. In general, there are four stages: 1) a first phase of bewilderment, numbness and denial, which may last a few hours (it can’t be true…); 2) a second, more prolonged phase of yearning and nostalgia, where the person misses the deceased and tries to compensate for the loss (I miss him/her so much…); 3) a third phase, characterized by disorganization and desperation when trying to continue living (a piece of me is missing…), and 4) a last phase of reorganization and recovery, always positive, where the person begins to use various skills to compensate for their loss, starts to feel the will to continue living, embraces help and the company of others, and can reminisce without as much pain (I am more calm, I should try to rebuild my life…).[3,6]
People often misunderstand the meaning of ‘grief resolution.’ This does not mean disloyal forgetting. Physical presence ends, but not the emotional relationship, which continues to change, continues to ‘restructure;’ the griever does not ‘give up’ the deceased, but rather tries to find an appropriate place for the deceased in the griever’s inner life, leaving space for new actions and life experiences.[3,6,13]
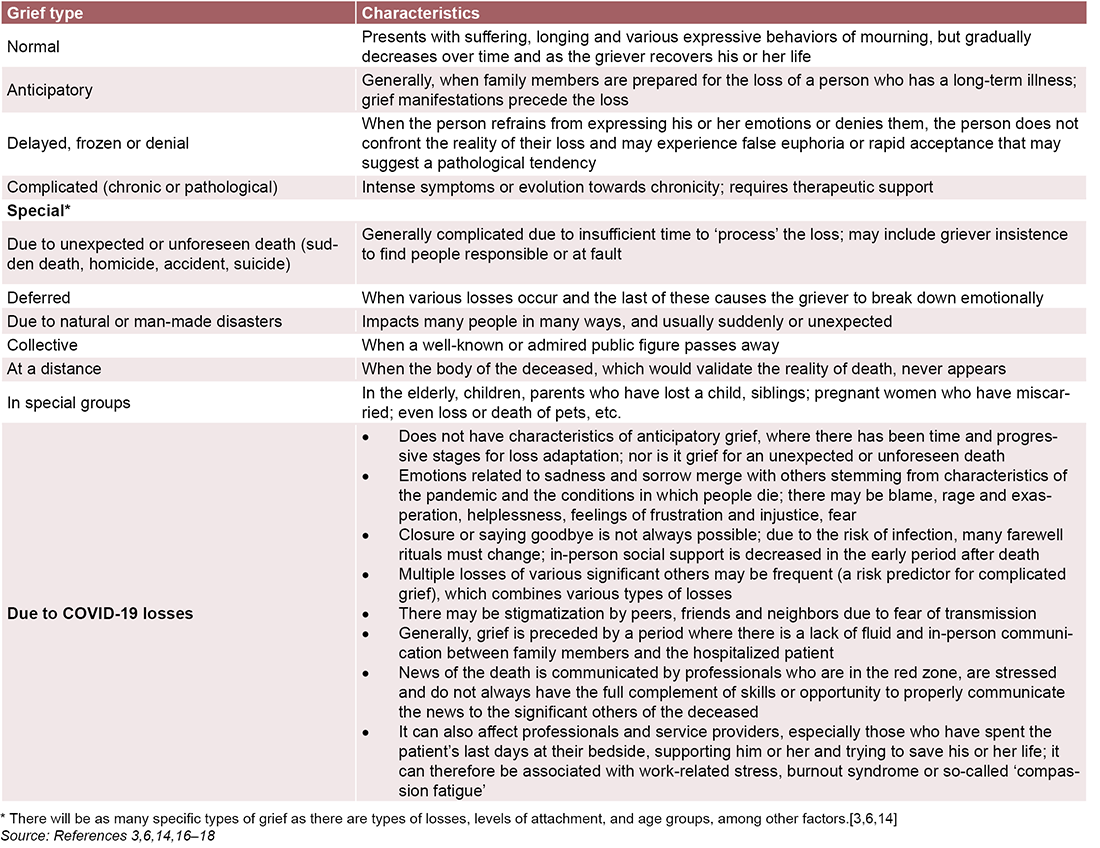
Table 1 summarizes grief types and their characteristics.[3,6,14,16‒18]
Specificities of COVID-19 loss and grief COVID-19 pandemic has brought about losses that affect practically all spheres of life: freedom of movement (defined by lockdown restrictions); affectionate connection through physical contact and in-person social relationships (especially among adolescents and youths); work and opportunities; in-person studies; family finances, etc. All of these imply a complex adaptive process in multiple dimensions. This global impact inherent to COVID-19, along with grief specificities, present a challenge for professionals who must assist and monitor the grief process.[14,15] Main specificities of grief from losses due to COVID-19 are summarized in Table 1.
Professionals assisting grievers should understand that family members and even health professionals may experience a great variety of mixed emotions and confusion due to the physical and psychological exhaustion accompanying the situation; even though these are normal reactions, they may be long-lasting. It is common for there to be many questions with no clear answers regarding what has happened. In addition to losing a family member, there are other special circumstances surrounding the loss of a loved one from COVID-19, such as not being able to take care of or accompany the family members or say goodbye during their last moments. This increases the risk of inadequate physical and psychological regulation associated with this immediate situation (palpitations, feeling of precordial chest pressure, or a knot in the throat or stomach, headaches, dry mouth, dizziness, mood changes, impatience, difficulty concentrating, etc.).[14−16]
Table 1: Grief types and their characteristics
Recommended guidelines for care of families who have lost members to COVID-19 It is difficult to identify a single protocol for grief care that is equally applicable to everyone. Generally, guidelines or recommendations must be accepted in a flexible and time-sensitive way for each grieving individual or family. We are dealing with a pandemic that we experience as continuous alarm. We should not be overly demanding of ourselves or grievers, as many of the current circumstances are out of our control. The aim is to strengthen grievers by patiently setting them on a continuous path towards acceptance and recovery.[13]
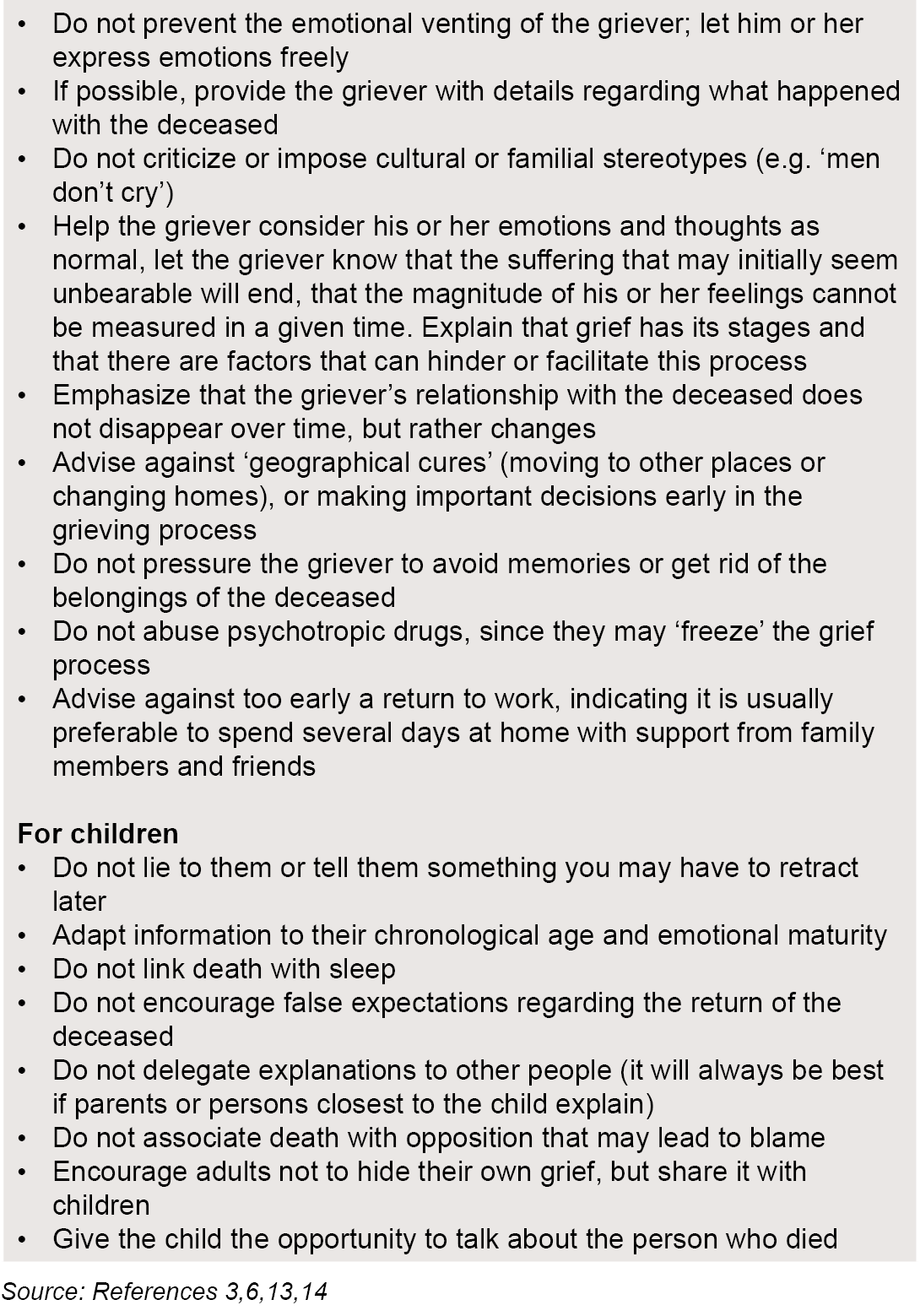
In general, the recommended measures for any grief are applicable in the face of losses due to COVID-19 (Table 2).[5,7−10,13]
Children require special management that is dependent on their concept of death, related to developmental growth (generally children acquire a concept of death similar to adults after 10 years of age); prior experiences with death in the family or outside of it; the family’s emotional stability and their relationships with other adults; the opportunity to share emotions and feelings; their relationship with the deceased; the environment surrounding the child at home and elsewhere; and the cause of the loss. In the case of COVID-19, it may be associated with prior feelings of threat due to the child’s excessive exposure to information from the media surrounding the pandemic.[13−18]
Over our 30 years of clinical practice, we have been approached multiple times by families seeking guidance on how to manage grief, not only in adults, but also in children. Not knowing how to tell a child about the death of a close family member (parent, grandparent, sibling) is a source of insecurity that sometimes leads to quick ‘solutions’ that include lying, avoidance, or using mystical explanations that complicate the normal course of grieving for the child later on. In Cuba, since family doctor-and-nurse offices are close by, embedded in every neighborhood, family members often seek orientation from either the family physician or the psychologist assigned to the office, sometimes before the death actually occurs. This guidance facilitates handling the grieving process with children in particular.
In the case of COVID-19 losses and children, a number of suggestions for support adapted from the broader spectrum of grief counseling can be applicable (Table 2).[13−18] Professional advice centers on not separating children from the reality that adults are experiencing, since they notice what is happening and it affects them if the news is not shared with them. While it is painful and difficult, it is usually preferable to tell them what happened as soon as possible, in the proper time and place using simple and sincere words (Something very sad has happened; Grandpa will no longer be with us, he is no longer alive), making the explanation as brief as possible (you know that he has been sick), and using age-appropriate language.
Table 2: Recommended general measures to treat all grief types, applicable to COVID-19 losses
For the family as a whole, upon learning of the person’s death, it is common for grievers to feel that they should do ‘something’, such as participate in a ritual of mourning. Rituals are symbolic acts that help express feelings in the face of loss, establish a certain order for life events, and allow the social construction of shared meanings. They also open the door to awareness of the grieving process. Some may be longer or shorter in terms of time: it is not the same to write a letter as it is to start a diary or create a permanent altar. What is important is that they help integrate what has happened and the way in which the loss is experienced. These rituals can be in-person or remote.[14−18]
It is generally preferred that in-person farewell rituals are more private events, or that only those with whom the person was closest are present; each person’s manner and personal space should be respected. Any variant can be performed, informing the people around them, always mindful of accompanying and caring for the closest loved ones. Depending on the situation, some mourning rituals may be held immediately, or others postponed. It is usually good to prepare something in writing for when it is possible for all the deceased’s loved ones to gather and make a small in-person tribute, or to record a video and share it with others via social media. Narrative therapy techniques are useful: writing a letter to the deceased, to a specific emotion (sadness, rage), to God, to life, to other people…it is healthy to write poems and messages with positive content (something that you would say to the person if they were present), to express memories and feelings of appreciation and forgiveness.
In remote farewell rituals, it may be advisable to schedule a meeting after consulting with family members, where everyone shares and expresses what they might like to do in a virtual ceremony. It may also be useful to post on social media, as a tribute, referring to aspects of the person’s legacy through words, music or images.
Grief guides with specific orientation for children and adolescents and people with cognitive disabilities, as well as for healthcare professionals, insist that euphemisms not be used (he is gone; he has left us; she has gone to sleep forever). It is preferable to speak about death naturally, attuned to the griever’s emotional reaction.[14−18] Children, the elderly and people with cognitive disabilities should not be excluded from these rituals, but rather participate in all ways their condition and age allow. Each person needs to feel loved and give love, be cared for and care, feel safe and provide safety, feel validated, strengthened, understood, respected, and accompanied in their life processes; therefore, it is also necessary that each one be able to reciprocate what they receive. This involves building social networks rather than walls.[16] We agree with Bucay; this is not easy, but it is possible—and it takes time.[13]
On the personal front, grievers may find solace in compiling works by authors with whom they identify, starting a diary or a series of drawings to express their feelings. A corner of a room can be set aside for remembrance, displaying a photo of the deceased or an object that symbolizes the relationship with that person, decorating it with flowers and candles, to pray, to express what is felt, and to call up memories.
Any normal grief (or uncomplicated grief) requires monitoring with support, accompaniment, and counseling, but not necessarily therapy.[3,14] However, psychiatric evaluation and treatment should be considered when grief manifests in a severe way, especially with suicidal ideation or suicidality or an increase of addictive substance use, when symptoms are severe and/or persistent and do not resolve with support interventions and counseling, or when there is other evidence of complication risk. In such cases, anxiolytic or antidepressant medications may be necessary for a short time, but these are not always needed, and their dose should be decreased progressively as soon as possible. The goal is not for the psychotropic drugs to ‘freeze’ the grieving process, which can lead to its chronic progression (a chronic grieving process).[19]
In cases of complicated grief, people often turn to specialized professionals who attempt to direct the process towards a normal evolution. Different models, methods and techniques have been used successfully for this, including problem solving, positive reevaluation, balance in emotion-focused coping, seeking out social and general support, encouraging spiritual values, even third-generation cognitive therapies such as mindfulness and acceptance and commitment therapy (ACT).[20−22] What is important is the timely detection of complicated grief, which can be done with a brief interview or questionnaires that may even be completed by telephone.[5,14]
Repercussions of COVID-19 loss on family life Family represents the social group with the greatest significance for most people. The first life lessons and fundamental learning in the process of personality formation usually take place in the family. For that reason, relationships established in the family and events within it can be sources of satisfaction, wellbeing and positive feelings, or alternatively, pain, frustration and despair.
The loss of a family member inexorably gives rise to a family crisis, which may be normative (related to the expected family life cycle) or para-normative (unexpected loss), but it is a high-impact event in family life, regardless. Death of a close relative from COVID-19 is a para-normative and unexpected event that occurs in a family that has already been affected—as have nearly all families—by the crisis generated by the pandemic and its impact on daily life.
Many family-related variables determine the response to the loss of a family member, such as communication, cohesion, family structure, roles, coping resources, lifestyle characteristics and belief systems, among others. Among the risk factors for complicated grief that should be considered when deciding whether professional interventions are necessary are: a) relational (age of the deceased and relationships of dependency, conflict or ambivalence); b) circumstantial (conditions in which the death occurred, uncertain death); c) personal (age of the survivor, poor stress management, comorbidities, previous grief); and d) social (isolation, socioeconomic difficulties, childcare, stigmas).[23]
During the pandemic, these processes are influenced by other conditions that add to the complexities surrounding the loss. Intra-family transmission of the virus (quite common) may cause feelings of guilt that add to those that death commonly produces in family members. Having thoughts such as: If I had protected myself better or required him or her to protect him or herself better; if I hadn’t left the house; if I had taken him or her to the hospital earlier, may hinder the normal course of grief. The inability to accompany family members during their hospitalization and to be present in critical moments, including at the time of death, greatly impedes or limits communication precisely when, in other circumstances, farewells, forgiveness, resolution of pending problems and satisfaction of last wishes would take place. This impossibility causes anguish in the family. The uncertainty regarding the way in which the family member died also contributes to these states of anxiety.
A review of research on the impact of grief on families during the pandemic[24] shows the primary need expressed by families is to be nearer to their loved one during the process of dying, and the impossibility of doing so becomes traumatic. Additional traumatic events include the feeling of loneliness during end-of-life care and lack of counseling for the family by healthcare personnel, as well as insufficient information or contradictory information provided by such personnel. These results confirm the urgent need for further preparation of healthcare personnel to more effectively support families facing loss.
If supporting a grieving person at any time is difficult, doing so while adhering to COVID-19 measures presents a bigger challenge. When in-person gatherings are not possible, it is important to find a virtual way to organize a collective farewell with the main grievers. It is important to show understanding; the situation is difficult, and the family may be overwhelmed or even difficult to contact at first try.[14−18] Yet, it is also helpful to stay in touch with them via telephone and social media to offer support (I just want to know how you are, and I want you to know that I am available if you want to talk. If you need to talk, you can call me, etc.). Active and empathetic listening is always preferable to trite expressions of sympathy (avoiding phrases such as: Be strong; cheer up; do it for your kids; don’t cry anymore, you are torturing yourself; life goes on.) The main message is always I want you to know that I am here, and I am thinking of you, and self-care should be encouraged and supported.
Experience in Cuba Cuba has conditions that favor family accompaniment during the grieving process and therapeutic follow-up as needed. In particular, its potential includes a universal health system that ensures equitable and free access to its citizens, a social orientation that prioritizes psychosocial problems, and availability of psychologists throughout the health system. Psychologists also work at the primary care level with family doctors and nurses, an ideal setting to offer follow-up care, help modify attitudes (in terms of their cognitive, emotional and behavioral components) and assist in charting a course towards a renewed positive sense of life among the grieving.[25‒28]
Given the peculiarities of the COVID-19 situation, the first task undertaken by the Ministry of Public Health and the National Psychology Group was to institute further training of professionals in the field. Scientific articles were widely distributed, accompanied by a newly-developed manual on providing support to the population, and precise orientation was provided via videoconferencing to the chairs of provincial chapters of the Cuban Society of Health Psychology and heads of provincial psychology services, to be shared with colleagues in each territory, along with the experiences accumulated.[27,28]
These guidelines were reinforced throughout the pandemic through various academic activities carried out face-to-face or remotely. The theme has been the subject of various manuscripts submitted for publication and in presentations at several international conferences. On a more personal level, psychologists and psychiatrists serving in the red zones also joined in mourning there, which even brought together other health professionals mourning the loss of their own family members.
Grief management was also a recurring theme in social communication throughout the country, considering the delicacy needed to address it, with care not to transmit hopelessness or reinforce fears created by the situation, and at the same time, to legitimize the difficult conditions for handling grief, as well as ways to satisfy the needs for emotional release and farewell rituals. Thus, the theme was the subject of various special television programs and spots.[29,30]
Psychological orientation for addressing grief was in constant demand during the epidemic in Cuba, especially in 2021 at the height of cases and deaths. Hence, the psychology and psychiatry services that remained open offered consults through video and WhatsApp groups. A hotline for psychological support that functioned 24 hours a day throughout the country also responded to calls seeking orientation on the grieving process. Due to the magnitude of the pandemic, and its effect on the entire population, there is obviously much work and follow-up still to be done. Thus, it is a priority, both for care and for continuing research on the subject.
At this stage in the pandemic, another factor influencing grief is the exhaustion of family members, with dwindling resources to address the crisis, and they may simply be at risk of burnout. This can have health implications for all family members, especially the most vulnerable, and may affect the completion of important family functions such as protection and care.
The greater extent of losses during the pandemic—of family members, friends, neighbors, coworkers and other acquaintances—has brought the notion of death closer to home, adding additional pain and fear for the health of the family’s remaining members and for oneself. Such specific conditions created by the spread of COVID-19 must be kept in mind when conducting preventive measures, family support or psychotherapeutic care in the ensuing period.
FINAL CONSIDERATIONS Grief management demands urgently needed comprehensive care for family members of the deceased. Even though this is a normal adaptive process necessary to restructure life after loss, which passes through several phases with variable duration, in the case of losses due to COVID-19, it takes on a special character: the absence of an acceptable farewell, as well as other specific characteristics, determine the forms grievers may use to adapt to the loss of their family member. Managing the process, according to specific guidelines, is beneficial not only for the griever closest to the deceased, but also for the entire family, for friends, people who were close to the deceased, and even for other health professionals.
It must not be forgotten that grief is a part of life and that, while difficult and painful, it is necessary to continue personal and family development. As Viktor Frankl said: “If you can no longer change a situation that causes you pain, you can always choose the attitude with which to confront the suffering,”[25] or, in the words of Jorge Bucay: “tears are, therefore, welcome…they mean we are on the road.”[13]
We believe that care for the general population during and post-pandemic will be incomplete if it does not entail attention to family members and significant others of the deceased. It is important that we are all prepared to participate in this care, particularly health professionals, with a special role for psychologists and psychiatrists.[29]
Ritchie H, Mathieu E, Rodés-Guirao L, Appel C, Giattino C, Ortiz-Ospina E, et al. Coronavirus Pandemic (COVID-19) [Internet]. Oxford: OurWorldInData.org; [cited 2021 Oct 23]. Available at: https://ourworldindata.org/coronavirus
Neimeyer RA. Aprender de la pérdida. Barcelona: Bolsillo Paidós; 2007. Spanish.
Grau J, Victoria CR, Vargas E. Perder, sufrir y seguir: el proceso de duelo. 1st ed. Guadalajara: UNIDAPSA; 2015. Spanish.
Victoria CR, Infante O, Grau J. Duelo y proceso salud-enfermedad en la atención primaria como escenario para su atención. Rev Cub Med Gen Integr. 2014 Mar;30(1):121−31. Spanish.
Batista MC. Evaluación del riesgo de duelo complicado de cónyuges de enfermos fallecidos por cáncer después de recibir Cuidados Paliativos en Gran Canaria y en La Habana [thesis]. [Gran Canaria]: Hospital Universitario “Dr. Negrín”/Universidad de Las Palmas de Gran Canaria, España; 2016. Spanish.
Gómez Sancho M. La pérdida de un ser querido. El duelo y el luto. 2nd ed. Madrid: Arán; 2007. Spanish.
American Psychiatric Association/APA. DSM-IV-TR. Manual diagnóstico y estadístico de los trastornos mentales. Texto revisado. Barcelona: Masson S.A.; 2001. Spanish.
Barreto P, Yi P, Soler C. Predictores del duelo complicado. Psicooncología. 2008;5(2−3):383−400. Spanish.
Bonanno GA, Kaltman S. The varieties of grief experience. Clin Psychol Rev. 2001 Jul;21(5):705−34.
Maercker A, Forstmeier S, Enzler A, Krüsi G, Hörler E, Maier C, et al. Adjustment disorders, posttraumatic stress disorder, and depressive disorders in old age: findings from a community survey. Comprehensive Psychiat. 2008;49(2):113‒20. https://doi.org/10.1016/j.comppsych.2007.07.002
Worden JW. El tratamiento del duelo: asesoramiento psicológico y terapia. Barcelona: Paidós; 1991–1997. Spanish.
Bucay J. El camino de las lágrimas. 5th ed. Buenos Aires: Océano; 2020. Spanish.
Infante Pedreira OE. Mochila Covid-19. Manuales para Apoyo Psicológico frente a la Pandemia [Internet]. Havana: Ministry of Public Health (CU); 2020 May 24 [cited 2021 Jul 20]. Available at: https://instituciones.sld.cu/psicologiadelasalud/mochila-covid-19/. Spanish.
Pan American Health Organization. Consideraciones psicosociales y de salud mental durante el brote de COVID-19 (Guía). Washington, D.C.: Pan American Health Organization; 2020. p. 1−7. Spanish.
Gallo M, Llaca C, Adamé MJ. Duelo por COVID. Porque no todas las despedidas son iguales [Internet]. Mexico City: Latin American Network of Child and Adolescent Psychology; Mexico Pediatric Hospital Medical Association; 2020 [cited 2020 Jul 15]. 27 p. Available at: https://cuidadospaliativos.org/blog/wp-content/uploads/2020/04/Duelo-por-Covid-19.pdf. Spanish.
Alarcón E, Prieto P, Cabrera CE, Rey P, García N, Robles M, et al. Guía para las personas que sufren una pérdida en tiempos del coronavirus (COVID-19) [Internet]. Barcelona: EQUIPO KOMOREBI, Especialistas en Pérdidas y Duelo; 2020 [cited 2021 Jul 20]. 37 p. Available at: http://www.ipirduelo.com/wp-content/uploads/GUI%CC%81A-DUELO-COVID19-2020.pdf. Spanish.
Sanfelices MP. Recomendaciones y guía de acompañamiento frente a duelos por COVID 19. Material preparado por la Mesa Social de Salud Mental y Bienestar Psicosocial. Un aporte de las Universidades del país frente a la pandemia del COVID-19. Santiago de Chile: MIDAP-CUIDA, Escuela de Psicología, Universidad Central de Chile; 2020 May 15 [cited 2021 Jul 20]. 28 p. Available at: http://www.psicologia.uc.cl/wp-content/uploads/2020/05/20200518_GUIAS-DE-ACOMPAN%CC%83AMIENTO-Y-DUELO-COVID-2.pdf. Spanish.
Kaplan H, Sadock B. Duelo, luto y el sentimiento de pérdida. In: Kaplan H, Sadock B, editors. Si-nopsis de Psiquiatría; Ciencias de la Conducta – Psiquiatría Clínica. 8th ed. Madrid: Editorial Médica Panamericana, S.A.; 1999. p. 78−83. Spanish.
Larrota-Castillo R, Méndez-Ferreira AF, Mora-Jaimes C, Córdoba Castañeda MC, Duque-Moreno J. Pérdida, duelo y salud mental en tiempos de pandemia. Rev Univ Industrial Santander, Salud UIS. 2020 Apr−Jun;52(2). Spanish.
Payás A. Las tareas del duelo. Psicoterapia del duelo desde un modelo integrativo-relacional. Madrid: Paidós; 2010. Spanish.
Cruz Gaitán JI, Reyes Ortega MA, Corona Chávez ZI. Duelo. Tratamiento basado en la terapia de aceptación y compromiso (ACT). México: Manual Moderno; 2017. Spanish.
Castillejo R. Duelo en tiempos de COVID.19. Claves para la evaluación de intervención de familiares. Conferencia al Congreso Internacional Virtual de Psicología. Barcelona: Higher Institute of Psychological Studies; 2021 Jul 22 [cited 2021 Jul 23]. Available at: https://www.youtube.com/watch?v=L6yQW3TUjew. Spanish.
Araujo M, García S, García B. Abordaje del duelo y de la muerte en familiares de pacientes con COVID-19: Revisión narrativa. Enf Clín. 2021;3:S112−S6. Spanish.
Frankl V. El hombre en busca del sentido. Barcelona: Herder, S.L.; 2004. Spanish.
Grau J, Infante O, Hernández L, Cobián A. La Psicología ante la COVID-19. Avances Médicos [Internet]. 2020 Jun15‒7 [cited 2020 Jun 20]. Available at: https://www.prensa-latina.cu. Spanish.
Infante O, Grau J (Comps). La Psicología de la Salud en el enfrentamiento a la COVID-19 en América Latina [Internet]. Havana: Pan American Health Organization; ALAPSA; CEDEM; 2021 [cited 2021 Jun 13]:150–84. Available at: https://alapsa.net/wp_content/uploads/2021/02/alapsa2021a.pdf. Spanish.
Infante O. Impacto de la pandemia por COVID-19 en la salud mental en Cuba. Revista Temas. 2020 Apr‒Sep;102‒3. Spanish.
Grau J. El manejo de las pérdidas en tiempos de COVID. Comparecencia televisiva en espacio de información a la población por el Dr. Durán. Cubavisión Internacional, conducido por Gisela García. 2021, agosto 25. Available at: https://de-de.facebook.com/HacemosCuba/videos/521546995800634/. Spanish.
Jorge Amado Grau-Abalo (Corresponding author: psico@infomed.sld.cu), clinical psychologist with a doctorate in the psychological sciences. Full professor and senior researcher. Medical University of Havana, Cuba. Head, National Psychology Group, Cuban Ministry of Public Health. Founder and vice-president, Latin American Psychology Association (ALAPSA). https://orcid.org/0000-0002-0044-3712
Olga Esther Infante-Pedreira, psychologist with a master’s degree in health psychology. Associate professor and associate researcher. Medical University of Havana, Cuba. Secretary, National Psychology Group, Cuban Ministry of Public Health. President, ALAPSA. https://orcid.org/0000-0002-6422-0016
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.