INTRODUCTION In November 2021, omicron—a new SARS-CoV-2 variant—was identified in South Africa and almost immediately, WHO declared it a ‘variant of concern’. In view of its rapid worldwide spread and its imminent introduction in Cuba, genomic surveillance was strengthened.
OBJECTIVES Describe cases during the first eight epidemiological weeks (epiweeks) of SARS-CoV-2 infection attributable to omicron variant in Cuba by clinical and epidemiological variables.
METHODSFrom epiweek 48, 2021 to epiweek 4, 2022, 288 nasopharyngeal swabs were processed for sequencing of a 1836 bp fragment of the S gene. Variants were identified according to GISAID database and confirmed by phylogenetic analysis. Variants’ association with clinical and epidemiological outcomes was assessed.
RESULTS The first cases of omicron variant were imported, mostly from African countries and the United States. During the period studied, omicron was detected in 83.0% (239/288) of cases processed, while the delta variant was found in 17.0% (49/288). Most persons infected with omicron were symptomatic (63.2%; 151/239) and fully vaccinated (65.3%; 156/239); severe cases and deaths occurred mainly among patients aged ≥65 years (92.9%; 13/14), and 12 of these deaths occurred in fully vaccinated persons (92.3%; 12/13). Omicron spread rapidly throughout the country (from 10% of cases in epiweek 48, 2021, to 100% by epiweek 4, 2022), displacing the formerly predominant delta variant.
CONCLUSIONS Omicron’s rapid expansion in Cuba was associated with increased incidence but not with a higher case fatality rate. The relatively milder disease in those infected with this variant could be influenced by the high vaccination coverage, along with the natural immunity acquired as a consequence of previous virus infection.
ABSTRACT INTRODUCTION In November 2021, omicron—a new SARS-CoV-2 variant—was identified in South Africa and almost immediately, WHO declared it a ‘variant of concern’. In view of its rapid worldwide spread and its imminent introduction in Cuba, genomic surveillance was strengthened.
OBJECTIVEDescribe cases during the first eight epidemiological weeks (epiweeks) of SARS-CoV-2 infection attributable to omicron variant in Cuba by clinical and epidemiological variables.
METHODS From epiweek 48, 2021 to epiweek 4, 2022, 288 nasopharyngeal swabs were processed for sequencing of a 1836 bp fragment of the S gene. Variants were identified according to GISAID database and confirmed by phylogenetic analysis. Variants’ association with clinical and epidemiological outcomes was assessed.
RESULTS The first cases of omicron variant were imported, mostly from African countries and the United States. During the period studied, omicron was detected in 83.0% (239/288) of cases processed, while the delta variant was found in 17.0% (49/288). Most persons infected with omicron were symptomatic (63.2%; 151/239) and fully vaccinated (65.3%; 156/239); severe cases and deaths occurred mainly among patients aged ≥65 years (92.9%; 13/14), and 12 of these deaths occurred in fully vaccinated persons (92.3%; 12/13). Omicron spread rapidly throughout the country (from 10% of cases in epiweek 48, 2021, to 100% by epiweek 4, 2022), displacing the formerly predominant delta variant.
CONCLUSIONS Omicron’s rapid expansion in Cuba was associated with increased incidence but not with a higher case fatality rate. The relatively milder disease in those infected with this variant could be influenced by the high vaccination coverage, along with the natural immunity acquired as a consequence of previous virus infection.
INTRODUCTION Several SARS-CoV-2 variants have circulated worldwide. On May 31, 2021, WHO introduced labels for SARS-CoV-2 variants of concern (VOC) and variants of interest (VOI) to be used with the scientific nomenclature. WHO updates the existing and emergent variants according to their detection frequency, transmissibility, severity or immune response.[1]
On November 24, 2021, South Africa reported detection of a new SARS-CoV-2 variant, designated as B.1.1.529. Two days later, WHO recognized this variant as a new VOC, named omicron.[2] Omicron has numerous mutations that could increase transmissibility, confer resistance to therapeutics, or partially escape from infection or vaccine-induced immunity.[3‒5] Preliminary evidence suggested that infection with the omicron VOC might have a milder clinical presentation compared to delta. However, further analysis showed that clinical evolution was more influenced by previously achieved immunity levels, rather than the intrinsic characteristics of the SARS-CoV-2 variant.[6,7] More recently, different omicron subvariants have been described, such as BA.1, BA.1.1, BA.2, BA.3, BA.4 and BA.5, according to WHO.[8]
IMPORTANCE This is the first description of SARS-CoV-2 infection by the omicron variant in Cuba, including the variant’s association with epidemiological and clinical variables during the first omicron surge, December 2021‒January 2022.
In Cuba, genetic surveillance of SARS-CoV-2 was started at the beginning of the Cuban epidemic, in March 2020. Circulation of 18 variants was detected in 2021 including: the Wuhan virus (Clade L), D164G (Clade G); the VOCs alpha, beta, gamma and delta; one VOI (lambda); and two previous VOIs (A.2.5.1 and Zeta/P.2). However, beta (34.8%), delta (24.9%) and D614G (19%) variants were the most frequently detected in 2021. Co-circulation of different predominant variants was observed in all epidemic waves; however, delta increased from 1.4% in May 2021 to 27.1% by June, 70.1% in July and 94.1% in August. By September, 100% of the studied samples were classified as delta, displacing the other variants circulating in the country; this suggested that delta had genetic advantages over other previously circulating variants.[9‒11]
Immediately after detection of omicron in South Africa, Cuba’s Ministry of Public Health (MINSAP) intensified genetic surveillance of SARS-CoV-2.[12,13] This study aims to summarize the characteristics of the first SARS-CoV-2 cases in Cuba attributable to the omicron variant, detected during epidemiological weeks (epiweeks) 48, 2021–4, 2022.
METHODS Study design This is a cross-sectional study, with viral genome analysis of nasopharyngeal swabs obtained from patients confirmed with infection by SARS-CoV-2 from epiweek 48, 2021 to epiweek 4, 2022. Samples included travelers from various countries and all Cuban provinces. Samples were collected at different points in the period studied, from patients exhibiting differences in clinical severity, from within areas with a significant increase of cases, and from diverse age groups (Table 1). Samples were sent to the Reference Laboratory for Influenza and Respiratory Viruses, in the Virology Department of the Pedro Kourí Tropical Medicine Institute (IPK), in Havana, Cuba, where genomic analysis was performed. As not all samples fulfilled the required quality attributes for amplification or sequencing, the number of samples with valid sequences varied by week.
Sequencing and variant designation Total RNA was extracted using the QIAcube Automated DNA/RNA Purification System and the QIAamp Viral RNA mini Kit (QIAGEN, Germany), following manufacturer’s instructions. cDNA synthesis and amplification of a 1836 bp fragment of the S gene (positions 21,976 to 23,812) was performed using the commercial kit One Step RT-PCR (QIAGEN, Germany), following manufacturer’s instructions. Primers for RT-PCR were those described in Protocols for SARS-CoV-2 Sequencing by the US Centers for Disease Control (CDC, Atlanta, USA).[14] The Dye Terminator Cycle Sequencing (DTCS) Quick Start commercial kit (Beckman Coulter, USA) was used for the sequencing reaction, with four primers spanning the entire amplified fragment of the S gene (positions 21,976 to 23,812).
Sequencing products were purified also according to the DTCS Quick Star Master Mix kit (Beckman Coulter, USA) and analyzed in a Beckman Coulter automatic sequencer model CEQTM8800 using the raw data analysis procedure for PCR products. Obtained sequences were assembled and edited using the Sequencher program (Sequence Analysis Software, Version 4.10.1, Gene Codes Corporation, USA). The complete Wuhan-Hu-1 sequence (NC_045512.2) was used as the reference nucleotide sequence. Mutations were identified using the CoVsurver interpretation algorithm: Mutation Analysis of hCoV-19, from the GISAID database (https://www.gisaid.org/epiflu-applications/covsurver-mutations-app). Cuban variants were named according to the mutational profile described in the GISAID database,[15] and confirmed by phylogenetic analysis, using the bioinformatics tool NGPhylogeny (https://ngphylogeny.fr).
Statistical analysis Descriptive statistics and graphics were obtained using Microsoft Office Excel 2010.
Ethics IPK’s Ethics Committee approved the study protocol. Epidemiological and clinical information was obtained from the case registry of MINSAP’s surveillance system fully protecting patient identities. WHO guidelines for clinical management of COVID-19[16] were used as criteria for clinical classification of asymptomatic and symptomatic (mild and severe) patients.
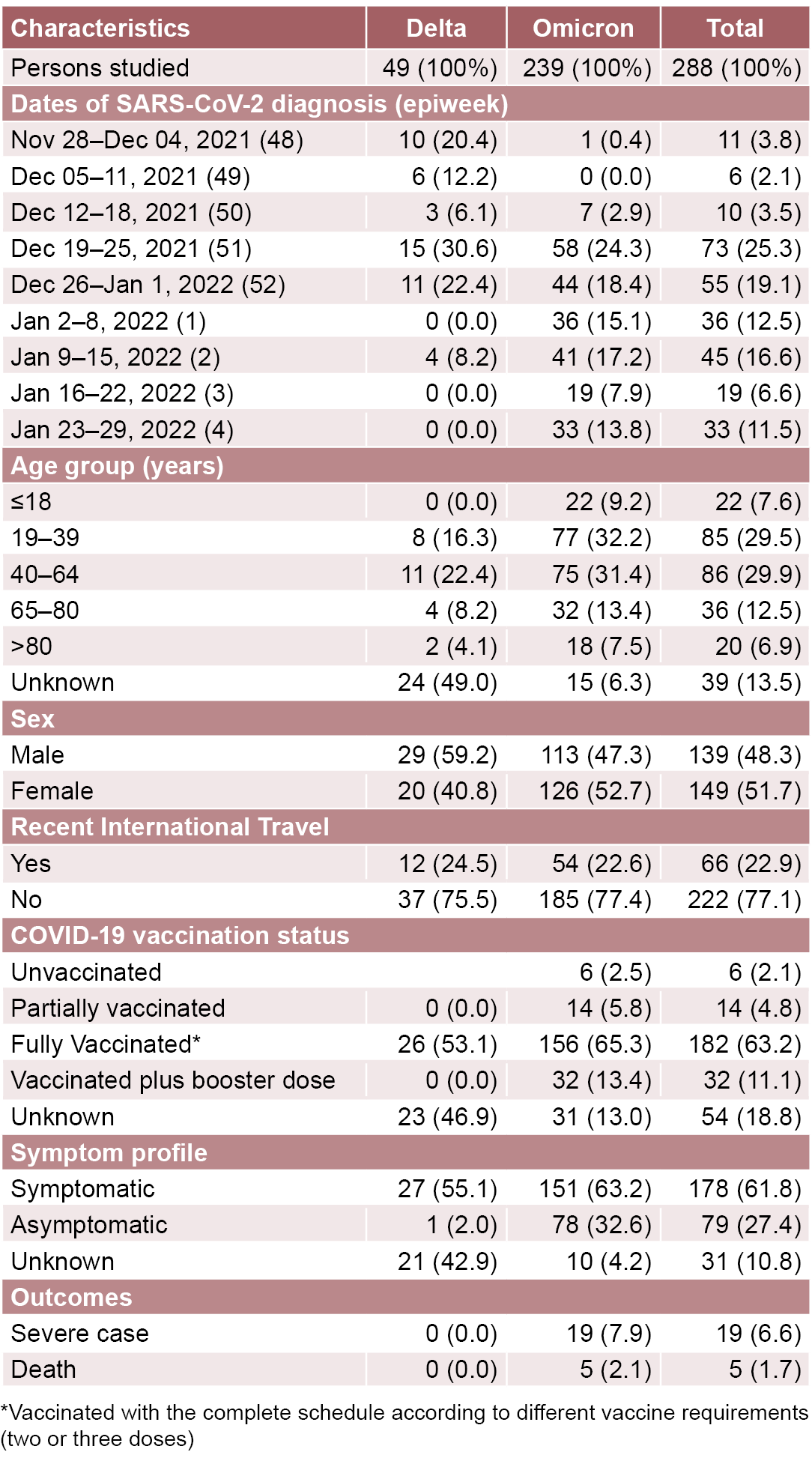
RESULTS During the study period, 288 nasopharyngeal swab specimens from persons with confirmed SARS-CoV-2 infection were sequenced. Table 1 describes the epidemiological and clinical characteristics of these first omicron cases detected in Cuba, during epiweeks 48, 2021–4, 2022.
Table 1: Demographic and clinical characteristics of persons studied, by SARS-CoV-2 variant: Cuba, epiweeks 48, 2021–4, 2022
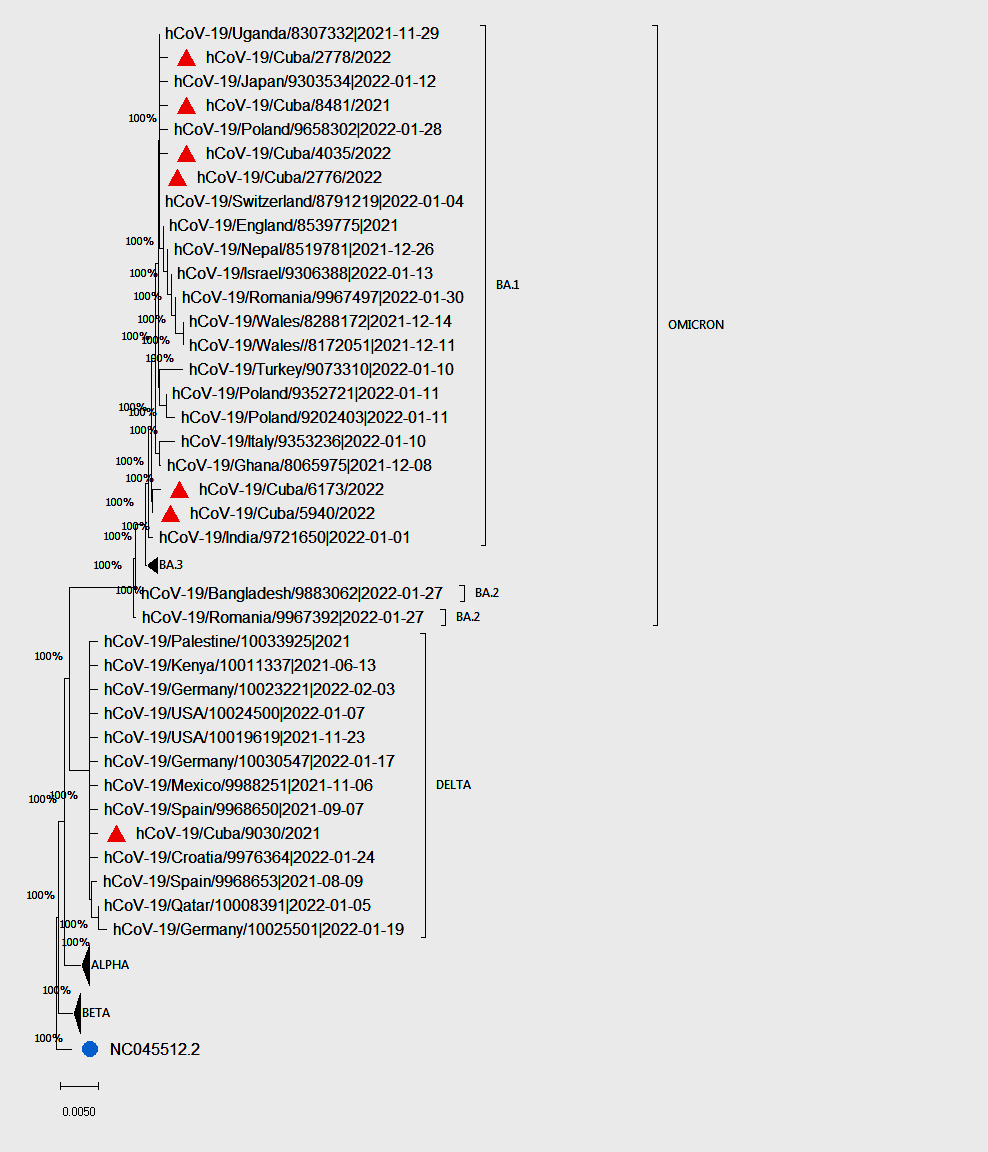
Figure 1: Phylogenetic tree with SARS-CoV-2 partial nucleotide S gene sequences of omicron and delta variants
Analysis included 50 reference nucleotide sequences of the S gene, and 7 Cuban sequences from the present study (1836 bp). Duplicate sequences were removed using the elimdupes tool (https://www.hiv.lanl.gov/content/sequence/elimdupesv2/elimdupes.html). Sequences were aligned using the Mega version 11.0.11 and the bioinformatics tool NGPhylogeny (https://ngphylogeny.fr/). The evolutionary history was inferred using the NJ method (https://ngphylogeny.fr). The consensus tree, inferred from 10,000 replicates, was used to represent the evolutionary history of the analyzed sequences. Our study samples are labeled with a red triangle. Sequences of alpha and beta variants are labeled with a black triangle. A blue circle shows the Wuhan-Hu-1 sequence, that was used as the outgroup.
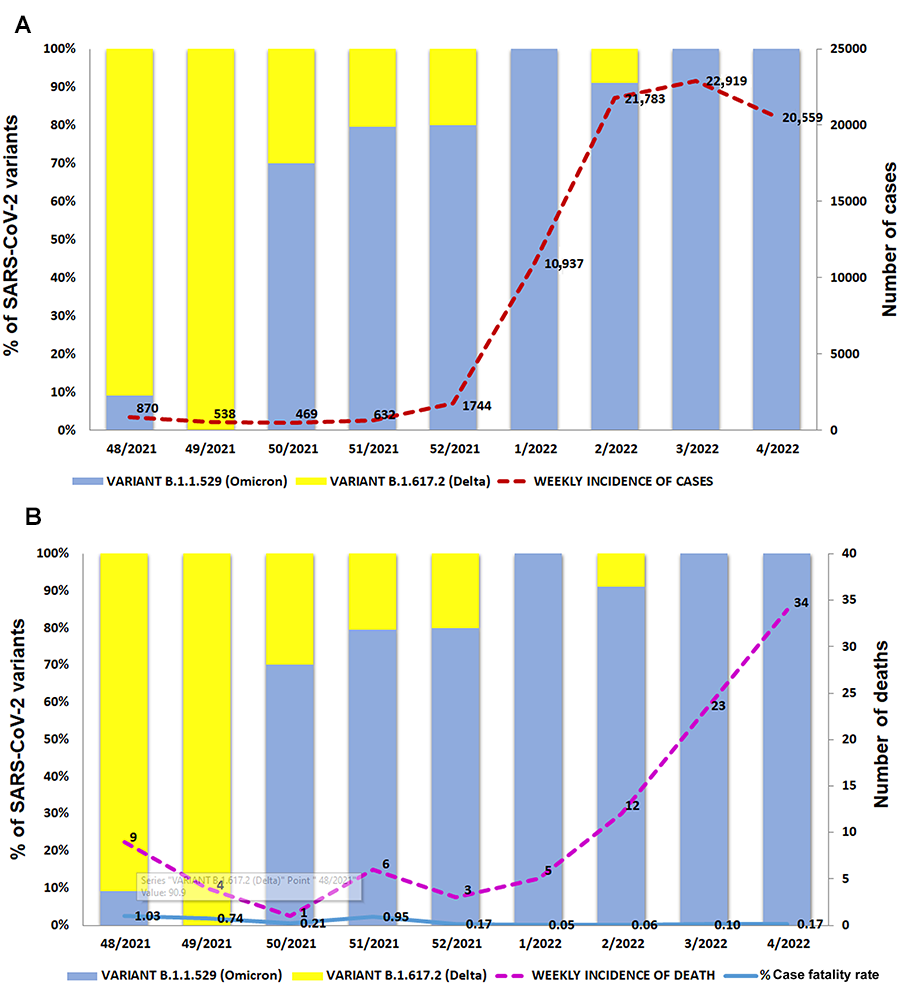
Figure 2: SARS-CoV-2 delta and omicron variants in Cuba, per number of cases and deaths, by epidemiological weeks
On December 1, 2021 (epiweek 48), the first case of COVID-19 attributable to omicron variant was identified in a Cuban traveler from Mozambique. This variant expanded rapidly, replacing delta, which had been predominant since July 2021.[13] By January 29, 2022, 239 omicron samples had been reported through genomic surveillance, all classified as omicron BA.1 subvariant (Figure 1). The rapid extension of the omicron variant was accompanied by an increase in case numbers (Figure 2A). However, case fatality rates (CFR) did not increase significantly (Table 1, Figure 2B).
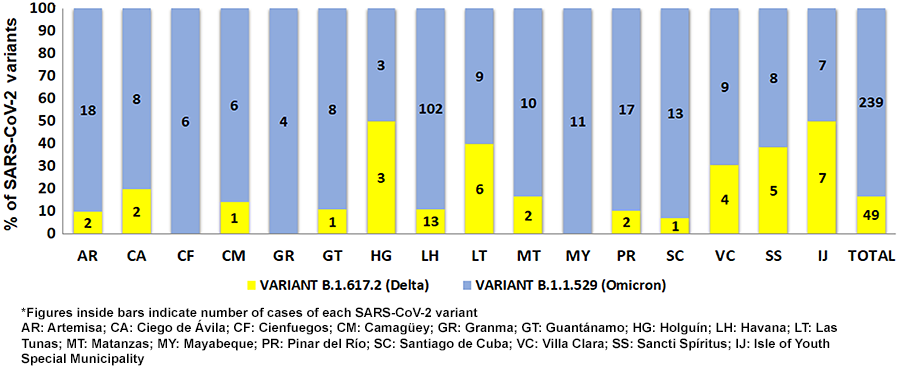
By the first epiweek of 2022, all sequenced samples were omicron, with the exception of four from the Isle of Youth Special Municipality, where the delta variant was still circulating. As of epiweek 3, 2022, all Cuban provinces had identified at least one omicron autochthonous case (Figures 2 and 3).
Most of the persons studied were aged 19‒64 years (59.4%; 171/288), with no differences for those infected with delta and omicron variants; in children (≤18 years, 7.6%; 22/288), only the omicron variant was detected (Table 1).
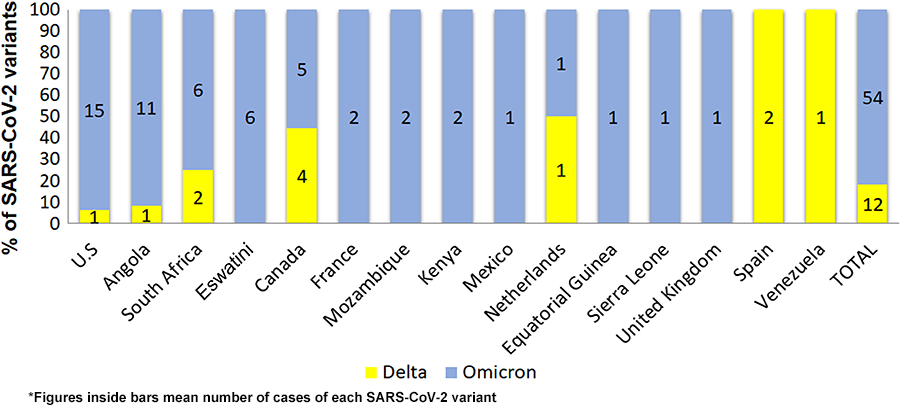
Sixty six recently arrived international travelers were positive for SARS-CoV-2 infection and classified as imported cases (Table 1). Fifty-four of them (81.8%; 54/66) carried omicron variant. Countries most represented in the introduction of this variant were the United States (15), Angola (11), South Africa and Eswatini (6 each), and Canada (5) (Figure 4).
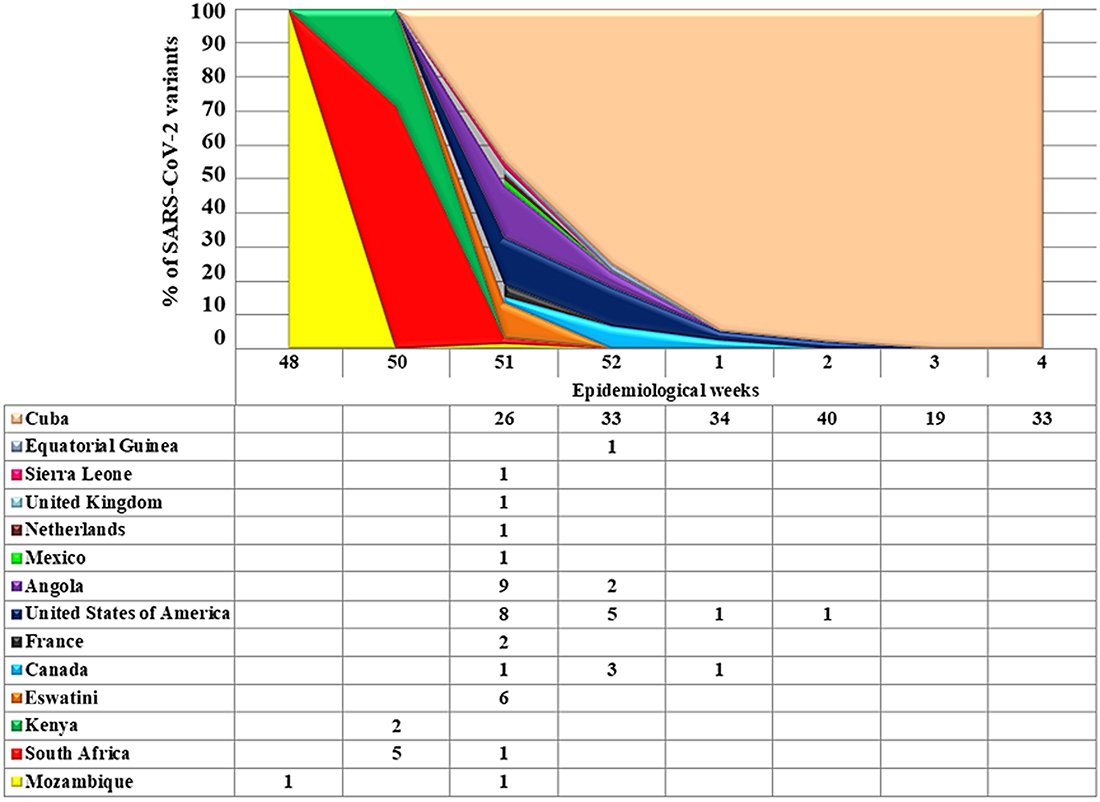
Omicron imported cases were predominant in epiweeks 48‒52, 2021 (51/54); autochthonous cases increased rapidly starting in epiweek 51, 2021 (Figure 5).
One hundred and eighty two (63.2%; 182/288) persons infected had completed the full 3-dose COVID-19 vaccination schedule, mainly with the Cuban vaccine Abdala, and 32 (11.1%; 32/288) had received additional booster doses; 17 of 22 children had been fully vaccinated, the remaining 5 were aged <2 years and therefore not eligible for vaccination, since the Cuban regulatory agency had only provided emergency use authorization for the Cuban vaccines beginning at 2 years old.[17] Vaccination status could not be determined in 54 individuals (18.7%; 54/288), most of whom were imported cases (Table 1).
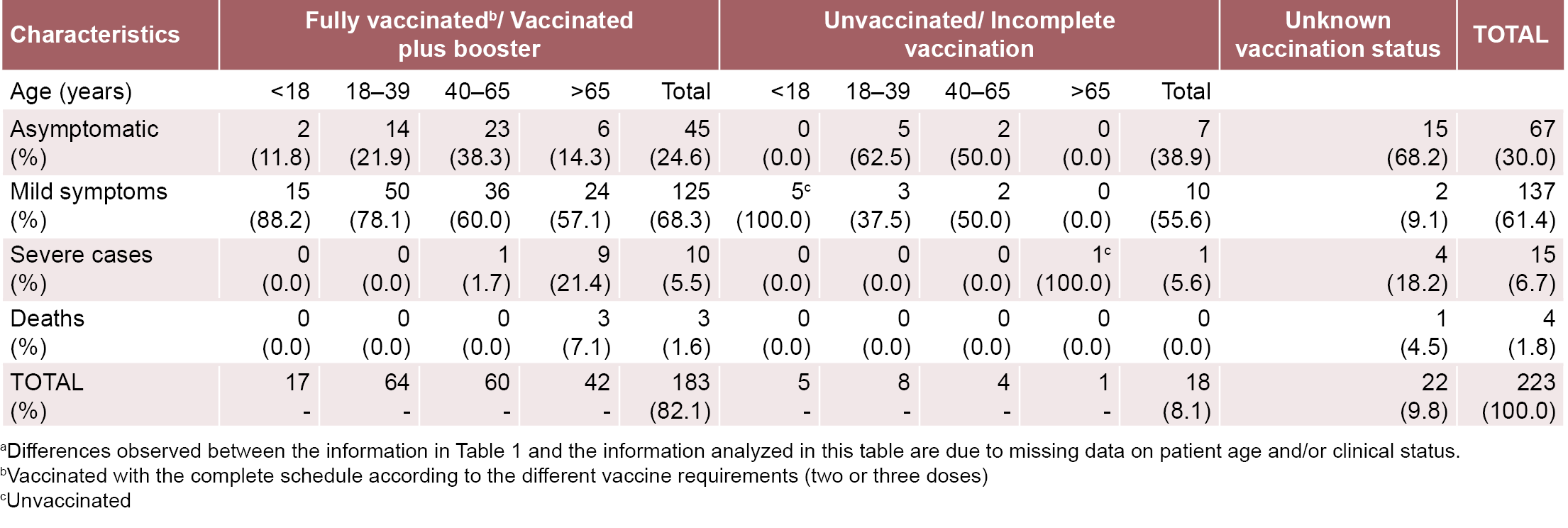
Overall, 178 (61.8%) patients presented with symptoms and 79 (27.4%) were asymptomatic. In those infected with the omicron variant, the percentage of symptomatic cases was slightly higher (63.2%; 151/239). Information on symptoms was lacking in a high proportion of those infected with the delta variant (46.9%; 23/49) (Table 1); 24 patients infected with the omicron variant developed severe disease and five of them died (Table 1). As described in Table 2, most severe or fatal cases (13/14, 92.9%) with documented age, were aged ≥65 years, and 12 of them had completed the vaccination schedule (Table 2).
DISCUSSION By epiweek 10, 2022, 446,987,500 COVID-19 cases and 6,022,374 deaths had been reported worldwide since the beginning of the pandemic; Cuba had reported 1,072,560 cases and 8500 deaths.[18]
Figure 3: SARS-CoV-2 delta and omicron variants in Cuba by province, epidemiological weeks 48, 2021‒4, 2022*
Figure 4: SARS-CoV-2 delta and omicron variants introduced in Cuba, by percentage and country of origin, November, 28 2021‒January 29, 2022*
Figure 5: Distribution of omicron cases in Cuba by country of origin, stratified by epidemiological week of detection (epiweeks 48, 2021-4, 2022)
The first case of COVID-19 attributed to the omicron variant was detected in Cuba during epiweek 48, 2021, only a few days after WHO declared this variant a VOC.[2,19] Initially, this variant was detected in travelers, arriving mainly from African countries (29 cases) or the USA (15 cases) where this variant had already been reported.[20,21] All Cuban isolates were classified as BA.1, as had been reported for most of the sequences worldwide.[8]
As in other countries, omicron emerged in Cuba when delta was the predominant circulating variant and rapidly displaced it, due to its higher transmission rate, infectivity and evasion of vaccine-induced immunity.[22,23] At the time, Cuba was in a favorable epidemiological context with low numbers of new cases (7-day moving average of daily new cases: 67, in epiweek 50, 2021) and extremely low number of deaths (7-day moving average of daily deaths: 0 on epiweek 50, 2021), principally due to high levels of immunity achieved—attributable to high vaccination coverage—including pediatric immunization (2‒18 years), and to the natural immunity acquired as a consequence of previous infection during the delta wave. When omicron was detected in Cuba (epiweek 48, 2021) 10,192,588 (91.1%) persons in Cuba had received at least one dose of the Cuban vaccines Abdala or Soberana and 83% of them had completed the 3-dose vaccination schedule. Only 3.9% had received a fourth (booster) dose.[24]
Emergence of the omicron variant in Cuba was accompanied by an increase in case numbers, but not higher CFR. By March 7, 2022, number of new cases had dropped to <600 cases per day (7-day moving average of daily new cases: 520).
Omicron’s first-wave peak in Cuba took place in epiweeks 2–4, 2022. The Cuban wave was less intense compared to other countries, including those with high vaccination coverage. As of January 29, 2022, Cuba reported 268.08 new COVID-19 cases per million population (pmp), while the UK, USA and Germany reported 1307.72, 1589.32 and 1740.56 cases pmp, respectively.[25] European countries with higher vaccination rates were better prepared for the autumn 2021 wave, despite the emergence of the more transmissible SARS-CoV-2 delta and omicron variants.[6]
A relatively high number of omicron-infected individuals were asymptomatic, as reported in other countries,[4,23,26] which has been attributed to a preferential infection of the upper respiratory tract.[27] Cuba’s high immunization coverage also may have facilitated the mild disease occurrence observed during the first omicron wave.[24] In fact, it has been argued that a milder clinical evolution in omicron cases may be associated with acquired immunity due to virus circulation or vaccination, rather than to intrinsic characteristics of this SARS-CoV-2 variant.[7]
Nevertheless, severe disease and even fatal outcomes have been reported globally from the omicron variant, mainly in older adults and those with various comorbidities.[28] Coinciding with previous reports, most severe cases and deaths observed in our study occurred in elders, probably associated to a less robust vaccine immune response, and a shorter durability of omicron-neutralizing antibodies due to immunosenescence.[29]
This study has some limitations. The number of samples studied was determined by the laboratory sequencing capacity. A number of samples positive for SARS-CoV-2 proportional to the number of cases in the country was selected each week; nevertheless, not all resulted in the required quality either during amplification or sequencing; in consequence, the number of samples sequenced was not homogeneous each week.
Although whole-genome sequencing was not performed, the sequences obtained covering the S gene from positions 21,976 to 23,812 permitted identification of SARS-CoV-2 variants circulating in Cuba.
Table 2: Demographic and clinical characteristics of persons infected by omicron, by COVID-19 vaccination status: Cuba, epiweeks 48, 2021–4, 2022a
CONCLUSION Beginning in late 2021 and into early 2022, the omicron BA.1 subvariant of SARS-CoV-2 rapidly replaced delta the variant in Cuba. Although the case numbers also increased, case fatality rates did not increase proportionally. The relatively milder form of the disease in individuals infected with this variant could be influenced by the high vaccination coverage achieved, including childhood immunization beginning at two years of age, along with the natural immunity acquired as a consequence of previous infection during the earlier delta wave.
ACKNOWLEDGMENTS The authors thank Drs Eva Harris, University of California, Berkeley, USA; Kevin Arien, Institute of Tropical Medicine, Belgium; and Leticia Franco and Jairo Mendez, PAHO-WHO. The authors also thank the PAHO-WHO permanent representation in Cuba and the Cuban network of molecular diagnostic laboratories for their support in sample collection.
World Health Organization [Internet]. Geneva: World Health Organization; c2022. Activities. Tracking SARS-CoV-2 variants; 2022 [updated 2022 Jul 7; cited 2022 Feb 26]; [about 5 p.]. Available at: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
Fernandes Q, Inchakalody VP, Merhi M, Mestiri S, Taib N, Moustafa Abo El-Ella D, et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann Med. 2022;54(1):524–40. https://doi.org/10.1080/07853890.2022.2031274
Mohapatra RK, Tiwari R. Omicron (B.1.1.529) variant of SARS-CoV-2: concerns, challenges, and recent updates. J Med Virol. 2022 Jun;94(6):2336–42. https://doi.org/10.1002/jmv.27633
Sikora D, Rzymski P. COVID-19 vaccination and rates of infections, hospitalizations, ICU admissions, and deaths in the European economic area during autumn 2021 wave of SARS-CoV-2. Vaccines (Basel). 2022 Mar 12;10(3):437. https://doi.org/10.3390/vaccines10030437
Bhattacharyya RP, Hanage WP. Challenges in inferring intrinsic severity of the SARS-CoV-2 Omicron variant. N Engl J Med. 2022 Jun 17;386(7):e14. https://doi.org/10.1056/nejmp2119682
Portal Miranda JA. Health intervention with vaccine candidates as a temporary strategy to confront COVID-19, Cuba, 2021. Rev Cubana Salud Pública [Internet]. 2021 Jan 5 [cited 2022 Feb 23];48(1):e3513. Available at: http://www.revsaludpublica.sld.cu/index.php/spu/article/view/3513. Spanish.
Global Initiative on Sharing All Influenza Data (GISAID) [Internet]. Munich: Global Initiative on Sharing All Influenza Data (GISAID); c2008–2022. CoVsurver: Mutation Analysis of hCoV-19; 2021 [cited 2022 Jan 20]. Available at: https://www.gisaid.org/epiflu-applications/covsurver-mutations-app/
World Health Organization [Internet]. Geneva: World Health Organization; c2022. Publications. Overview. Living guidance for clinical management of COVID-19; 2021 Nov 23 [cited 2022 Feb 23]; [2.4 MB]. Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2
Reported Cases and Deaths by Country or Territory [Internet]. [place unknown]: Worldometers; 2022 [cited 2022 March 7]; [about 10 p.]. Available at: www.worldometers.info/coronavirus/#countries
Fall A, Eldesouki RE, Sachithanandham J, Paul Morris C, Norton JM, Gaston DC, et al. A quick displacement of the SARS-CoV-2 variant Delta with Omicron: unprecedented spike in COVID-19 cases associated with fewer admissions and comparable upper respiratory viral loads. medRxiv [Preprint]. 2022 Jan 28. 2022.01.26.22269927. https://doi.org/10.1101/2022.01.26.22269927
Mohapatra RK, Tiwari R. Twin combination of Omicron and Delta variants triggering a tsunami wave of ever high surges in COVID-19 cases: a challenging global threat with a special focus on the Indian subcontinent. J Med Virol. 2022 May;94(5):1761–5. https://doi.org/10.1002/jmv.27585
Our World in Data [Internet]. Oxford: Global Change Data Lab; c2022. Coronavirus. Vaccinations. Coronavirus (COVID-19) Vaccinations; [cited 2022 May 30]; [about 10 p.]. Available at: https://ourworldindata.org/covid-vaccinations
Garrett N, Tapley A, Andriesen J, Seocharan I, Fisher LH, Bunts L, et al. High rate of asymptomatic carriage associated with variant strain Omicron. medRxiv [Preprint]. 2022 Jan 14;2021.12.20.21268130. https://doi.org/10.1101/2021.12.20.21268130
Piersiala K, Kakabas L, Bruckova A, Starkhammar M, Cardell LO. Acute odynophagia – a new symptom of COVID-19 during the SARS-CoV-2 Omicron variant wave in Sweden. J Intern Med. 2022 Jul;292(1):154–61. https://doi.org/10.1111/joim.13470
Kahn F, Bonander C, Moghaddassi M, Rasmussen M, Malmqvist U, Inghammar M, et al. Risk of severe COVID-19 from the Delta and Omicron variants in relation to vaccination status, sex, age and comorbidities – surveillance results from southern Sweden, July 2021 to January 2022. Euro Surveill. 2022 Mar;27(9):2200121. https://doi.org/10.2807/1560-7917.es.2022.27.9.2200121
Vanshylla K, Tober-Lau P, Gruell H, Münn F, Eggeling R, Pfeifer N, et al. Durability of omicron-neutralising serum activity after mRNA booster immunisation in older adults. Lancet Infect Dis. 2022 Apr;22(4):445–6. https://doi.org/10.1016/s1473-3099(22)00135-9
THE AUTHORS
Lissette Pérez-Santosa, microbiologist with a master’s degree in virology and a doctorate in health sciences. Associate professor and senior researcher, Virology Department, Pedro Kourí Tropical Medicine Institute (IPK), Havana, Cuba. https://orcid.org/0000-0002-5127-2167
Vivian Kourí-Cardelláa(Corresponding author: vkouri@ipk.sld.cu), physician specializing in microbiology, with a master’s degree in virology and infectious diseases, a doctorate in virology and an advanced doctorate in sciences. Senior professor and researcher, Virology Department, IPK. Havana. Cuba. https://orcid.org/0000-0001-7878-7542
Yahisel Tejero-Suárez, healthcare technologist, with a master’s degree in virology. Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-4781-6088
Dailyn Medero-Díaz, microbiologist with a master´s degree in virology. Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-3169-9972
Yenisleidys Martínez-Montesino, healthcare technologist with a master’s degree in virology. Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0001-8183-3685
Yanaris López-Almaguer, physician with dual specialties in hygiene and epidemiology, and family medicine, with a master’s degree in public health. Associate professor and researcher, IPK, Havana, Cuba. https://orcid.org/0000-0003-2472-644X
José Raúl de Armas-Fernández, physician specializing in hygiene and epidemiology, with a master’s degree in public health. Ministry of Public Health, Havana, Cuba. https://orcid.org/0000-0002-7351-7006
José Angel Portal-Miranda, physician with dual specialties in family medicine and health organization and administration, with a master’s degree in satisfactory longevity and a doctorate in health sciences. Full professor and senior researcher, National School of Public Health and Ministry of Public Health, Havana, Cuba. https://orcid.org/0000-0002-9532-4483
María Guadalupe Guzmán-Tiradoa(Corresponding author: lupe@ipk.sld.cu), physician specializing in microbiology with a master’s degree in virology, a doctorate in virology and an advanced doctorate in sciences. Full professor and senior researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0003-3927-0844
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.