INTRODUCTION Urinary tract infection is the second-leading reason for consults in primary health care. Bacterial urinary tract infections are the most common, of which Escherichia coli is the main etiologic agent. Antimicrobial resistance and multidrug resistance complicate effective community treatment, especially if resistance is caused by extended-spectrum beta-lactamase production. WHO recommends that antimicrobial susceptibility be evaluated in different regions of the world at different times. Community-acquired E. coli’s susceptibility to colistin has not yet been studied in Cuba, and mcr-1 gene screening is necessary.
OBJECTIVE Evaluate community-acquired uropathogenic E. coli isolates’ susceptibility to antibiotics, including colistin, and identify extended-spectrum beta-lactamase–producing bacteria.
METHODS We conducted a descriptive cross-sectional study that included 281 community-acquired uropathogenic E. coli isolates (153 from the Isle of Youth Special Municipality’s Hygiene, Epidemiology, and Microbiology Center and 128 from Microbiology Laboratories of 7 institutions in Havana) from June 2016 through July 2018. We used the disk diffusion method to determine susceptibility to ampicillin, ampicillin/sulbactam, cefazolin, trimethoprim/sulfamethoxazole, ciprofloxacin, nitrofurantoin and fosfomycin. The disk elution method was used to determine susceptibility to colistin. The combined disk method was used to identify extended-spectrum beta-lactamases. Estimates were made regarding the frequency and percentages of antimicrobial susceptibility and resistance, as well as multidrug-resistance patterns.
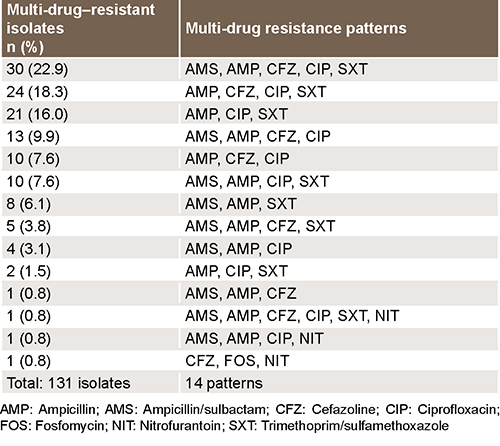
RESULTS Of the 281 isolates, 68.3% (192/281) were resistant to ampicillin, 54.8% (154/281) were resistant to ciprofloxacin, and 49.5% (139/281) were resistant to trimethoprim/sulfamethoxazole. Resistance to colistin was not detected. On the other hand, 14.2% (40/281) were susceptible to the 8 antibiotics we evaluated, 22.1% (62/281) showed resistance to only 1 antibiotic, and 63.7% (179/281) were resistant to 2 or more antibiotics. In the extended-spectrum beta-lactamase determination, 34.5% (97/281) had inhibition zones ≤14 mm with cefazolin. Of those with inhibition zones, 64.9% (63/97) were positive in the phenotype test, and 35.1% (34/97) were negative. In extended-spectrum beta-lactamase–producing bacteria, 1.6% (1/63) were resistant to fosfomycin, and 3.2% (2/63) were resistant to nitrofurantoin. The most common multidrug-resistance pattern (22.9%; 30/131) was to ampicillin/sulbactam, ampicillin, cefazolin, ciprofloxacin, and trimethoprim/sulfamethoxazole.
CONCLUSIONS Uropathogenic E. coli resistance to the antibiotics most frequently used in community medical practice is quite common, and extended-spectrum beta-lactamase–producing bacteria is the mechanism for beta-lactam antibiotic resistance. Multidrug-resistance patterns include resistance to the antibiotics most used in community-acquired infections. Fosfomycin and nitrofurantoin are the most active in extended-spectrum beta-lactamase producing bacteria. All the isolates were susceptible to colistin.
ABSTRACT INTRODUCTION Urinary tract infection is the second-leading reason for consults in primary health care. Bacterial urinary tract infections are the most common, of which Escherichia coli is the main etiologic agent. Antimicrobial resistance and multidrug resistance complicate effective community treatment, especially if resistance is caused by extended-spectrum beta-lactamase production. WHO recommends that antimicrobial susceptibility be evaluated in different regions of the world at different times. Community-acquired E. coli’s susceptibility to colistin has not yet been studied in Cuba, and mcr-1 gene screening is necessary.
OBJECTIVE Evaluate community-acquired uropathogenic E. coli isolates’ susceptibility to antibiotics, including colistin, and identify extended-spectrum beta-lactamase–producing bacteria.
METHODS We conducted a descriptive cross-sectional study that included 281 community-acquired uropathogenic E. coli isolates (153 from the Isle of Youth Special Municipality’s Hygiene, Epidemiology, and Microbiology Center and 128 from Microbiology Laboratories of 7 institutions in Havana) from June 2016 through July 2018. We used the disk diffusion method to determine susceptibility to ampicillin, ampicillin/sulbactam, cefazolin, trimethoprim/sulfamethoxazole, ciprofloxacin, nitrofurantoin and fosfomycin. The disk elution method was used to determine susceptibility to colistin. The combined disk method was used to identify extended-spectrum beta-lactamases. Estimates were made regarding the frequency and percentages of antimicrobial susceptibility and resistance, as well as multidrug-resistance patterns.
RESULTS Of the 281 isolates, 68.3% (192/281) were resistant to ampicillin, 54.8% (154/281) were resistant to ciprofloxacin, and 49.5% (139/281) were resistant to trimethoprim/sulfamethoxazole. Resistance to colistin was not detected. On the other hand, 14.2% (40/281) were susceptible to the 8 antibiotics we evaluated, 22.1% (62/281) showed resistance to only 1 antibiotic, and 63.7% (179/281) were resistant to 2 or more antibiotics. In the extended-spectrum beta-lactamase determination, 34.5% (97/281) had inhibition zones ≤14 mm with cefazolin. Of those with inhibition zones, 64.9% (63/97) were positive in the phenotype test, and 35.1% (34/97) were negative. In extended-spectrum beta-lactamase–producing bacteria, 1.6% (1/63) were resistant to fosfomycin, and 3.2% (2/63) were resistant to nitrofurantoin. The most common multidrug-resistance pattern (22.9%; 30/131) was to ampicillin/sulbactam, ampicillin, cefazolin, ciprofloxacin, and trimethoprim/sulfamethoxazole.
CONCLUSIONS Uropathogenic E. coli resistance to the antibiotics most frequently used in community medical practice is quite common, and extended-spectrum beta-lactamase–producing bacteria is the mechanism for beta-lactam antibiotic resistance. Multidrug-resistance patterns include resistance to the antibiotics most used in community-acquired infections. Fosfomycin and nitrofurantoin are the most active in extended-spectrum beta-lactamase producing bacteria. All the isolates were susceptible to colistin.
INTRODUCTION Urinary tract infections (UTIs) are one of the leading reasons for consults in primary health care. The US Centers for Disease Control and Prevention defines UTIs as common infections occurring when bacteria, often from the skin or rectum, enter the urethra and infect the urinary tract.[1]
The most common UTI cause is bacterial infection, and according to microbiology studies, Escherichia coli is the enterobacteria responsible for ≥80% of cases.[2] Sometimes symptoms do not disappear after treatment, possibly due to patient risk factors, the microorganism’s virulence and pathogenicity, or bacteria’s growing resistance to the antibiotics most often used in treatment.[3]
IMPORTANCE This work highlights the need to conduct sensitivity tests before treating urinary tract infections caused by E. coli, due to increasing antimicrobial resistance in Cuba.
The most common practice for treating community-acquired UTIs is prescribing treatment without prior microbial identification. However, due to increasing antibiotic resistance, this approach is not very effective.[4] Extended-spectrum beta-lactamase (ESBL) production is the mechanism most often associated with multidrug resistance in gram-negative bacilli, especially in E. coli,[3] and increased incidence in community isolates has been reported.[4]
The prevalence of multidrug-resistant uropathogenic E. coli varies by geographic region.[5] Monitoring its susceptibility to antibiotics helps detect variations in usual susceptibility patterns and assists in properly treating UTIs by decreasing treatment failures due to antibiotic resistance.[3]
In 2015, a mechanism for transferable colistin resistance was first detected—mediated by the mcr-1 gene in E. coli and Klebsiella pneumoniae isolates collected from hospitalized patients, animals and raw meat.[6] For this reason, WHO recommends screening for this resistance mechanism, and the Latin American and Caribbean Network for Antimicrobial Resistance proposes evaluating country-specific E. coli community isolates’ susceptibility to colistin.[7,8]
In Cuba, studies show a high prevalence of UTI-causing E. coli that are resistant to the most common antibiotics used in medical practice and community circulation of ESBL-producing isolates.[9,10] However, research including different health institutions and geographic areas in the country is lacking. Furthermore, there are no reports about uropathogenic E. coli’s susceptibility to colistin in community isolates as a preliminary step to mcr-1 gene screening.
The purpose of this research was to evaluate uropathogenic E. coli’s susceptibility to antibiotics (including colistin) in community-acquired isolates, and to identify ESBL-producing bacteria.
METHODS Design and sample We performed a descriptive cross-sectional study including 281 community-acquired UTI-causing E. coli isolates; 153 were collected by the Isle of Youth Special Municipality’s Center for Hygiene, Epidemiology, and Microbiology, and 128 were collected from microbiology laboratories in several Havana hospitals from outpatients with community-acquired infections (namely the Calixto García, Manuel Fajardo, Enrique Cabrera, Ramón González Coro, William Soler and Freyre Andrade hospitals, and the Pedro Kourí Tropical Medicine Institute’s [IPK] Clinical Microbiology Laboratory). Samples were collected from June 2016 through July 2018 and were studied in the National Reference Laboratory for antimicrobial resistance surveillance in infection-related pathogens associated with health care, at IPK in Havana.
Antimicrobial susceptibility Antimicrobial susceptibility was determined using the Kirby-Bauer technique in Mueller-Hinton agar,[11] except for susceptibility to colistin, which was studied using the colistin disk elution method in cation-adjusted Mueller-Hinton broth, according to the protocol recommended by the National Infectious Disease Institute at Dr. Carlos G. Malbrán National Laboratory and Health Institute Administration (INEI-ANLIS), Argentina, in 2017,[12] and susceptibility to fosfomycin, which was studied using Müeller-Hinton agar supplemented with glucose-6-phosphate.[13] The antibiotics studied were ampicillin/sulbactam (gradient strips 0.016–256 μg/L), ampicillin (0.016–256 μg/L), cefazolin (30 μg), ciprofloxacin (gradient strips 0.0032–32 μg/L), fosfomycin (200 μg), nitrofurantoin (30 μg), trimethoprim/sulfamethoxazole (1.25/23.75 μg) and colistin (10 μg). Disks and concentration gradient strips were sourced from Liofilchem (Italy). Results were interpreted according to the Clinical and Laboratory Standards Institute’s (CLSI) 2019 standards,[14] USA, except for colistin results, which were interpreted according to the Antimicrobial Resistance Surveillance Network’s (WHONET-Argentina) protocol.[7]
E. coli isolates’ microbial susceptibility were rated as follows: ‘sensitive’ (antimicrobial activity level is associated with a high probability of therapeutic success); ‘intermediate’ (a high probability of therapeutic success because exposure to the agent is increased by either dosage or concentration at the site of infection); or ‘resistant’ (antimicrobial activity level is associated with a high probability of therapeutic failure).[7,14]
ESBL detection Cefazolin disks were used as predictors of susceptibility to oral cephalosporins based on the WHONET’s 2017 protocol.[7] For all isolates with inhibition zones ≤14 mm for this antibiotic, the ESBL-producer phenotype was confirmed using the combined disk method: 1) ceftazidime (30 µg) and ceftazidime/clavulanic acid (30/10 µg), and 2) cefotaxime (30 µg) and cefotaxime/clavulanic acid (30/10 µg) (Liofilchem, Italy).[14] The K. pneumoniae ATCC 700603 strain was used as a positive control, and the E. coli ATCC 25922 strain was used as a negative control.
Statistical analysis Descriptive statistical measures (frequencies and percentages) were used to analyze isolates’ antimicrobial susceptibility profiles, multidrug-resistance patterns and ESBL production.
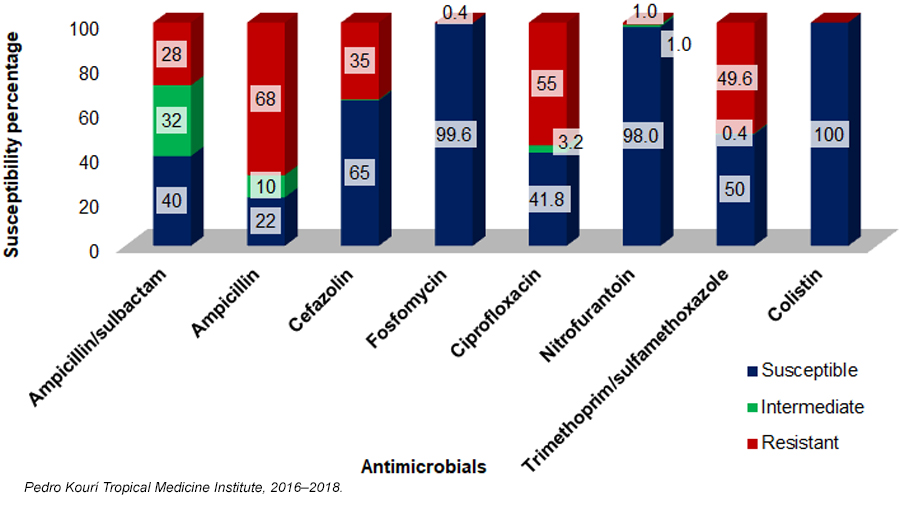
RESULTS Of the 281 uropathogenic E. coli isolates, 68.3% (192/281) were resistant to ampicillin, 54.8% (154/281) to ciprofloxacin and 49.5% (139/281) to trimethoprim/sulfamethoxazole. The percentages of isolates resistant to cefazolin (34.5%; 97/281) and to the ampicillin/sulbactam combination (28.1%; 79/281) were considered high, as they were above 20%. Figure 1 shows susceptibility and resistance percentages based on whether they were susceptible, intermediate or resistant.
Figure 1: Susceptibility to antimicrobials of Escherichia coli isolates causing community-acquired urinary tract infections (n = 281)
The percentages of fosfomycin-resistant isolates and nitrofurantoin-resistant isolates were low (Figure 1). Resistance to colistin was not found, even though colistin was only evaluated in order to start mcr-1 gene screening (Figure 1). Percentages of resistant isolates were quite similar between Havana and the Isle of Youth (Table 1).
Of the isolates, 14.2% (40/281) were susceptible to the 8 antibiotics evaluated, 22.1% (62/281) were resistant to only 1 antibiotic, and 63.7% (179/281) were resistant to 2 or more antibiotics. Resistant isolates had 24 different antibiotypes, 10 of which include 1 or 2 antibiotic classes, and 14 include ≥3 classes. They were therefore considered multidrug-resistant (MDR) patterns.
Table 1: Percentage of uropathogenic Escherichia coli-resistant isolates, by geographic area
Of the MDR patterns, 4 were found in a single isolate, and 6 were repeated in 2 or more isolates. Most MDR patterns demonstrate resistance to ampicillin, ciprofloxacin and trimethoprim/sulfamethoxazole (Table 2).
In the ESBL determination, 34.5% (97/281) of isolates had inhibition zones ≤14 mm for cefazolin. Of those with inhibition zones, 64.9% (63/97) were positive in the phenotype test and 35.1% (34/97) were negative. All (63/63) of the positive ESBLs were resistant to cefazolin and ampicillin, 44.4% (28/63) were resistant to the ampicillin/sulbactam combination, 47.6% (30/63) to ciprofloxacin, and 42.9% (27/63) to trimethoprim/sulfamethoxazole. Fosfomycin and nitrofurantoin had the best in vitro activity in ESBL-positive uropathogenic E. coli isolates; 1.6% (1/63) of the isolates were resistant to fosfomycin, and 3.2% (2/63) to nitrofurantoin. We subdivided the susceptibility and resistance percentages based on whether they were susceptible, intermediate or resistant (Figure 2).
DISCUSSION Physicians have historically prescribed antibiotics for UTIs without conducting microbiology studies to identify the causal bacteria, but emerging antibiotic resistance is increasingly limiting this practice.
UTI treatment guidelines advise refraining from antibiotic use without susceptibility studies if the local resistance rate is greater than 20%.[5] For this reason, data on bacterial resistance patterns to antibiotics commonly used to treat UTIs should be frequently updated. These patterns vary by geographic region and may even change over time in a single area or within a single country.[15]
High rates of ampicillin resistance in uropathogenic E. coli isolates have been reported worldwide.[16,17] Several authors have reported ampicillin to be the antibiotic most affected by resistance in Cuba.[16–20] Poor in vitro efficacy and high resistance indicates that the use of ampicillin in the treatment of uncomplicated UTI without prior microbial identification should be avoided.[5]
Ciprofloxacin and trimethoprim/sulfamethoxazole are the most-commonly prescribed antibiotics in primary health care appointments in Cuba because of their recognized efficacy in treating UTIs, their availability on the market and their low cost, but indiscriminate use or misuse of both antibiotics has caused a decrease in bacterial susceptibility percentages in hospital-acquired and community-acquired infections.[21]
González[22] and more recently Cabrera[3] reported that >30% of community-acquired UTI-causing uropathogenic E. coli were resistant to ciprofloxacin in the province of Havana and to trimethoprim/sulfamethoxazole in the province of Mayabeque. In different parts of the world, this pathogen’s resistance rates to both antibiotics exceeds 20%.[4,16]
Figure 2: Susceptibility of ESBL-producing Escherichia coli isolates causing community-acquired urinary tract infections to antimicrobials (n = 63)
ST131, an emerging hyperepidemic clone of UTI-causing E. coli—resistant to fluoroquinolones and co-resistant to other antibiotic classes—is often resistant to ciprofloxacin and can be found worldwide.[5] In Cuba, this clone was found in E. coli clinical isolates, so it could be responsible for the multidrug resistance in this study’s isolates.[10]
Due to bacterial resistance to fluoroquinolone and to trimethoprim/sulfamethoxazole, using these antibiotics in community-acquired infections is not advised, and cephalosporin resistance limits treatment options. Using these antibiotics without previous susceptibility tests delays appropriate therapy, causes therapeutic failure and increases treatment costs.[5]
Although cefazolin (cephalosporin for parenteral use) is a very good predictor of susceptibility to oral cephalosporins in resistance studies, its use for susceptibility estimates is not recommended. Instead, susceptibility or resistance to oral cephalosporins available in the local health area should be studied, because there is no oral presentation for cefazolin.[7]
In this study, less than 20% of isolates were resistant to cefazolin, consistent with what Marrero reported in the eastern province of Holguín;[19] therefore, oral cephalosporins are not recommended in treating community-acquired UTIs.
The combination of penicillins and beta-lactamase inhibitors, such as clavulanic acid, tazobactam and sulbactam, strengthens the action of these drugs by restoring their antimicrobial activity against bacteria that are resistant because of plasmid-mediated beta-lactamase production.[20] However, in this study, we found high frequencies of uropathogenic E. coli resistance to the ampicillin/sulbactam combination. This coincides with results of various studies in Cuba and other countries.[5,9,16,20] Therefore, use of this combination is limited in severe community-acquired infections where its in vitro efficacy has not been demonstrated.
Because of bacterial resistance, antibiotics that were used for a long time as first-line UTI treatment stopped being used without first performing susceptibility tests, and nitrofurantoin and fosfomycin were adopted to treat community-acquired UTIs.[23] Nitrofurantoin is a good option for treating uncomplicated community-acquired UTI because it achieves good concentrations in urine, has low resistance, and has been prescribed in Cuba and elsewhere as a urinary bacteriostatic agent for many years.[3,22] Fosfomycin has bactericidal action, is broad-spectrum, achieves high concentrations in urinary tracts, has low toxicity, and can be effective as a single dose for uncomplicated UTI treatment.[24]
Our results show good in vitro nitrofurantoin and fosfomycin activity against this pathogen. Previous studies in Cuba have shown uropathogenic E. coli susceptibility levels to both antibiotics at >90%.[3,22] However, nitrofurantoin’s wide range of side effects (nausea, vomiting, abdominal pain, decreased appetite) leads to low treatment adherence, and in Cuba the oral presentation of fosfomycin trometamol is not available, so treating UTIs with those antibiotics in Cuban communities is unfeasible.
We did not find resistance to colistin, which could be because its use is limited to treating severe infections caused by gram-negative, multidrug-resistant bacilli. This reaffirms the need to continue using it appropriately.[8] Because community-acquired E. coli expressing the transferable colistin-resistant mcr-1 gene is circulating in the world, Cuba’s microbiology laboratory network needs to actively screen for resistance to colistin in enterobacteria collected from community-acquired infections.
Evaluating community isolates’ susceptibility to colistin has epidemiologic value in researching the mcr-1 gene and its variants, if one considers that WHO has issued an epidemiological alert notifying mcr-1 gene detection in E. coli community isolates in several countries, and has called on countries to implement and maintain the capacity for detecting, preventing and controlling transmission of microorganisms with transferable colistin resistance.[8]
Resistance patterns vary over time and by geographic region; therefore, it is advisable to maintain active local surveillance to update treatment guidelines as needed.[15] In this study, however, we did not find major differences between resistance profiles of isolates from Havana and those from the Isle of Youth.
MDR patterns coincide with the observations by Expósito,[18] who reported five MDR patterns in community-acquired UTI-causing E. coli isolates in Cuba’s Guantánamo province, where most common resistance was to trimethoprim/sulfamethoxazole, ciprofloxacin, tetracycline and ampicillin. Guzmán reported higher resistance to ampicillin, cephalosporins, trimethoprim/sulfamethoxazole and ciprofloxacin in Venezuela.[16]
ESBL detection is used as a relevant clinical and epidemiological marker for reducing morbidity and mortality caused by ESBL-producing bacteria.[9] In the last few years, a growing number of reports show these microorganisms in community isolates.[15] It is important to determine their national, local and even institutional incidence in order to adjust antibiotic therapies, and to avoid treatment failures and increased resistance levels.
Cefazolin disks, a good ESBL predictor in antimicrobial susceptibility testing, helped detect isolates whose phenotypes included the ESBL mechanism. On these grounds, cefazolin disks are recommended for inclusion in Cuba’s Microbiology Laboratory Network for researching community-acquired isolates, since ESBL-producing bacteria have been reported in Cuban communities.[9,10,20]
Multidrug-resistance in ESBL-producing bacteria is a significant health problem because these enzymes confer resistance to penicillins, cephalosporins and aztreonam; and 30% to 60% are resistant to beta-lactam antibiotics associated in their formulation with beta-lactamase inhibitors. ESBLs are coded in plasmids that carry resistance genes for other antibiotic classes, including quinolones, aminoglycosides and trimethoprim/sulfamethoxazole,[25] which were observed in the ESBL-positive strains isolated in our research.
It is a challenge to select antibiotic regimens for ESBL-producing bacteria because these must be adjusted to possible causative agents, and during selection, doctors must consider local epidemiology, which differs from hospital to hospital and from city to city.[26]
García[27] suggests the primary measures for preventing ESBL-producing bacteria are frequent handwashing, disinfecting surfaces that may serve as vectors, and reducing inappropriate antibiotic use—especially that of cephalosporins and quinolones. According to García, nitrofurantoin and fosfomycin have good activity in ESBLs, so they appear the best treatment options for uncomplicated UTIs caused by ESBL-producing microorganisms.[27] The results of this study reaffirm this proposal and coincide with reports by other authors who say that most community-acquired UTI-causing ESBL-producing E. coli are susceptible to these two antibiotics.[4,26,28] This could be due to the infrequent use of nitrofurantoin and fosfomycin trometamol in recent years, considering that the latter is not available in Cuba. However, due to bacterial capacity for mutation and continued adaptation to the environment, resistance surveillance and rational antibiotic use should be maintained.[15]
This research is limited by the fact that we did not know the patients’ clinical characteristics, which kept us from classifying the type of urinary infection, and because we did not study the susceptibility pattern of all bacterial uropathogens that caused UTIs; our study was limited to E. coli. However, guidelines for urinary tract infection treatment are based on the susceptibility of E. coli, the most commonly-isolated bacteria.
Another limitation of the study is that colistin susceptibility was only evaluated as a preliminary step in screening for the mcr-1 gene; we did not perform molecular studies to confirm whether any of the studied isolates carried this gene or its variants.
Considering the high resistance to ciprofloxacin and known circulation of the high-risk clone ST-131 in community isolates in Cuba, we recommend performing molecular epidemiology studies of isolates to help determine whether they belong to this clone.
CONCLUSIONS There is a high frequency of resistance of uropathogenic E. coli to antibiotics most commonly used in medical practice, with extended-spectrum beta-lactamase–producing bacteria as the mechanism for resistance. Multidrug-resistance patterns include three or more of the antibiotic classes most commonly used for community infections. Fosfomycin and nitrofurantoin are the most active antibiotics in extended-spectrum beta-lactamase–producing bacteria. All isolates were susceptible to colistin.
Gonzáles Rodríguez AO, Barrón Pastor HJ, Gutiérrez Villafuerte CA, Llimpe Mitma de Barrón YL, Huerta Canales de Miranda DV, Suárez S. Clasificación filogenética de Escherichia coli uropatógena y respuesta inmunometabólica en adultos mayores con infección urinaria en casas de reposo. Arch Med [Internet]. 2019 Jul 24; 19(2):238–46. https://doi.org/10.30554/archmed.19.2.3334.2019. Spanish.
Cabrera Rodríguez LE, Díaz Rigau L, Miralles Suárez AI, Ones Roque R, Torres Herrera Y, Pantaleón Hernández M. Efectividad in vitro de la amikacina y fosfomicina en cepas de Escherichia coli uropatógena multidrogorresistentes. CCM [Internet]. 2019 Jul 23 [cited 2022 Jan 15];23(4). Available at: http://www.revcocmed.sld.cu/index.php/cocmed/article/view/3253/1686. Spanish.
Galindo Méndez M. Caracterización molecular y patrón de susceptibilidad antimicrobiana de Escherichia coli productora de β-lactamasas de espectro extendido en infección del tracto urinario adquirida en la comunidad. Rev Chilena Infectol [Internet]. 2018 [cited 2022 Jan 15];35(1):29–35. https://dx.doi.org/10.4067/s0716-10182018000100029. Spanish.
Navarro NM, Euan BOG, Bolado ME, Moreno IGM, Castillón CLG, Robles ZRE. Dos años de vigilancia de la resistencia a los antibióticos de Escherichia coli uropatógena en una clínica de medicina familiar. Enf Inf Microbiol. 2017 Apr–Jun;37(2):40–4. Spanish.
Liu YY, Wang Y, Walsh TR, Yi LX, Zhang R, Spencer J, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis [Internet]. 2016 Feb 1 [cited 2020 Mar 13];16(2):161–8. http://dx.doi.org/10.1016/S1473-3099(15)00424-7. Spanish.
Servicio Antimicrobianos del INEI-ANLIS “Dr. Carlos G. Malbrán”. Alerta epidemiológica: MCR-1 en Argentina. Emergencia de resistencia plasmídica (transferible) a colistin/polimixina [Internet]. Buenos Aires: Servicio Antimicrobianos del INEI-ANLIS “Dr. Carlos G. Malbrán”; 2016 Feb [cited 2020 Mar 13]. 9 p. Available at: http://antimicrobianos.com.ar/ATB/wp-content/uploads/2016/02/Alerta-epidemiol%C3%B3gico.pdf. Spanish.
Argüez de Paz AR, Rodríguez Chávez A, Rojas Hernández N. Klebsiella pneumoniae y Escherichia coli productoras de betalactamasas en pacientes con infección del tracto urinario. Rev Cub Med Int Emerg. 2015 Sep 8;14(4):16–29.
Quiñones D, Soe Aung M, Carmona Y, Pereda Novales N, Kobayashi N. Molecular epidemiology and prevalence of extended-spectrum betalactamase and carbapenemase genes of extraintestinal pathogenic Escherichia coli in Cuba. Proceedings of the 29th ECCMID Congress; 2019 Apr 13–16; Amsterdam, Netherlands, 2019.
Velasco J, Araque MC, Araujo E, Longa A, Nieves B, Ramírez AC, et al. Manual práctico de bacteriología clínica. Práctica 2: Prueba de susceptibilidad antimicrobiana. 1st digital ed [Internet]. Mérida (VE): Universidad de Los Andes; 2011. p. 25–9. Available at: https://docplayer.es/16647412-Manual-practico-de-bacteriologia-clinica.html. Spanish.
Vieira Franco de Godoy Carvalhaes CH, Gales AC. Manual de Mecanismos de Resistencia a Antibióticos. Fosfomicina. Curso online iberoamericano: Interpretación del antibiograma en la práctica clínica diaria [Internet]. Stockholm: European Committee on Antimicrobial Susceptibility Testing (EUCAST); 2016 [cited 2020 Mar 13]. 14 p. Available at: https://dokumen.tips/documents/manual-de-mecanismos-de-resistencia-a-antibio-este-complejo-se-une-a-sitios.html. Spanish.
Clinical and Laboratory Standars Institute (CLSI). Performance Standars for Antimicrobial disk susceptibility tests. M100 29th ed [Internet]. Pennsylvania: Clinical and Laboratory Standars Institute (CSLI); 2019 [cited 2020 Mar 13]. 25 p. Available at: https://clsi.org/media/2663/m100ed29_sample.pdf
Guzmán M, Salazar E, Cordero V, Castro A, Villanueva A, Rodulfo H, et al. Multidrug resistance and risk factors associated with community-acquired urinary tract infections caused by Escherichia coli in Venezuela. Biomédica. 2018 Apr 9; 39(Suppl 1):96–106. https://doi.org/10.7705/biomedica.v39i2.4030
Garza Montúfar ME, Treviño Valdez PD, De la Garza Salinas LH. Resistencia bacteriana y comorbilidades presentes en pacientes urológicos ambulatorios con urocultivos positivos. Rev Med Inst Mex Seguro Soc [Internet]. 2018 May [cited 2020 Mar 15];56(4):347–53. Available at: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=84101. Spanish.
Expósito Boue LM, Bermellón Sánchez S, Lescaille Garbey L, Delgado Rondón N, Aliaga Castellanos I. Resistencia antimicrobiana de la Escherichia coli en pacientes con infección del tracto urinario. Rev Inf Cient [Internet]. 2019 Nov–Dec [cited 2021 Dec 16];98(6):755–64. Available at: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-99332019000600755&lng=es. Epub 2019 Dec 18. Spanish.
Marrero Escalona JL, Leyva Toppes M, Castellanos Heredia JE. Infección del tracto urinario y resistencia antimicrobiana en la comunidad. Rev Cubana Med Gen Integr. 2015 Jan–Mar;31(1):78–84. Spanish.
Suárez Trueba B, Milián Samper Y, Espinosa Rivera F, Hart Casares M, Llanes Rodríguez N, Martínez Batista ML. Susceptibilidad antimicrobiana y mecanismos de resistencia de Escherichia coli aisladas a partir de urocultivos en un hospital de tercer nivel. Rev Cubana Med. 2014 Jan–Mar;53(1):3–13. Spanish.
Muiños Torres JC, Alvarez Varela E, Caravia Pubillones I, Peña Brito I. Resistencia a antibióticos en aislamientos de Escherichia coli en infecciones del tracto urinario inferior adquiridas en la comunidad: diferencias en relación con la edad. Revista CENIC Cienc Biol [Internet]. 2008 Sep–Dec [cited 2021 Dec 16];39(3). Available at: https://revista.cnic.edu.cu/index.php/RevBiol/article/download/686/564/1485. Spanish.
González Colón Y, Duquesne Alderete A, Ruiz Turcás M. Caracterización epidemiológica y microbiológica de las infecciones del tracto urinario en el Hospital Ortopédico Docente Fructuoso Rodríguez. Año 2015. Panorama Cuba y Salud [Internet]. 2018 May 18 [cited 2021 Dec 16];13(2):11–7. Available at: http://www.revpanorama.sld.cu/index.php/panorama/article/view/11-17. Spanish.
Huttner A, Kowalczyk A, Turjeman A, Babich T, Brossier C, Eliakim-Raz N, et al. Effect of 5-day Nitrofurantoin vs single-dose Fosfomycin on clinical resolution of uncomplicated lower urinary tract infection in women. A randomized clinical trial. JAMA [Internet]. 2018 May 1 [cited 2021 Dec 16];319(17):1781–9. Available at: https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2018.3627. https://doi.org/10.1001/jama.2018.3627
Hernández MS, García JA, Muñoz JL. Actividad in vitro de fosfomicina frente a enterobacterias de origen urinario productoras de betalactamasas de espectro extendido. Rev Esp Quimioter [Internet]. 2009 Mar [cited 2021 Dec 16];22(1):25–9. Available at: https://pesquisa.bvsalud.org/portal/resource/pt/ibc-77644. Spanish.
Losada I, Barbeito G, García-Garrote F, Fernández-Pérez B, Malvar A, Hervada X, et al. Estudio de sensibilidad de Escherichia coli productores de infecciones del tracto urinario comunitarias en Galicia. Período: 2016-2017. Atención Primaria [Internet]. 2020 Aug–Sep;52(7):462–8. Available at: https://www.sciencedirect.com/science/article/pii/S0212656718304748?via%3Dihub. https://doi.org/10.1016/j.aprim.2019.06.007. Spanish.
THE AUTHORS
Yenisel Carmona-Cartaya (Corresponding author: yeniselc@ipk.sld.cu), physician specializing in microbiology with a master’s degree in bacteriology and mycology. Instructor, Pedro Kourí Tropical Medicine Institute (IPK), Havana, Cuba. https://orcid.org/0000-0003-1241-5302
Mercedes Hidalgo-Benito, physician specializing in microbiology. Héroes de Baire Hospital, Isle of Youth Special Municipality, Cuba. https://orcid.org/0000-0002-1907-1947
Niurka Pereda-Novales, healthcare technologist, with a master’s degree in parasitology. Assistant professor, IPK, Havana, Cuba. https://orcid.org/0000-0002-4408-7721
Dianelys Quiñones-Pérez, physician specializing in microbiology, with a master’s degree in microbiology and a doctorate in medical sciences. Full professor and senior researcher, IPK, Havana, Cuba. https://orcid.org/0000-0003-4506-6890
Submitted: September 03, 2021 Approved: April 04, 2022 Disclosures: None
Carmona-Cartaya Y, Hidalgo-Benito M, Borges-Mateus LM, Pereda-Novales N, González-Molina MK, Quiñones-Pérez D. Community acquired uropathogenic Escherichia coli, antimicrobial susceptibility, and extended spectrum beta-lactamase detection. MEDICC Rev. 2022 Apr;24(2):20–25. https://doi.org/10.37757/mr2022.v24.n2.2
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.