ABSTRACT INTRODUCTION SARS-CoV-2 infection can produce endothelial injury and microvascular damage, one cause of the multiorgan failure associated with COVID-19. Cerebrovascular endothelial damage increases the risk of stroke in COVID-19 patients, which makes prompt diagnosis important. Endothelial dysfunction can be evaluated by using transcranial Doppler ultrasound to study cerebral hemodynamic reserve, but there are few of these studies in patients with COVID-19, and the technique is not included in COVID-19 action and follow-up guidelines nationally or internationally.
OBJECTIVE Estimate baseline cerebral hemodynamic patterns, cerebral hemodynamic reserve, and breath-holding index in recovered COVID-19 patients.
METHOD We conducted an exploratory study in 51 people; 27 men and 24 women 20–78 years of age, divided into two groups. One group comprised 25 recovered COVID-19 patients, following clinical and epidemiological discharge, who suffered differing degrees of disease severity, and who had no neurological symptoms or disease at the time they were incorporated into the study. The second group comprised 26 people who had not been diagnosed with COVID-19 and who tested negative by RT-PCR at the time of study enrollment. Recovered patients were further divided into two groups: those who had been asymptomatic or had mild disease, and those who had severe or critical disease. We performed transcranial Doppler ultrasounds to obtain baseline and post-apnea tests of cerebral hemodynamic patterns to evaluate cerebral hemodynamic reserve and breath-holding indices. We characterized the recovered patient group and the control group through simple descriptive statistics (means and standard deviations).
RESULTS There were no measurable differences in baseline cerebral hemodynamics between the groups. However, cerebral hemodynamic reserve and breath-holding index were lower in those who had COVID-19 than among control participants (19.9% vs. 36.8% and 0.7 vs. 1.2 respectively). These variables were similar for patients who had asymptomatic or mild disease (19.9% vs.19.8%) and for those who had severe or critical disease (0.7 vs. 0.7).
CONCLUSIONS Patients recovered from SARS-CoV-2 infection showed decreased cerebral hemodynamic reserve and breath-holding index regardless of the disease’s clinical severity or presence of neurological symptoms. These abnormalities may be associated with endothelial damage caused by COVID-19. It would be useful to include transcranial Doppler ultrasound in evaluation and follow-up protocols for patients with COVID-19.
ABSTRACT INTRODUCTIONSARS-CoV-2 infection can produce endothelial injury and microvascular damage, one cause of the multiorgan failure associated with COVID-19. Cerebrovascular endothelial damage increases the risk of stroke in COVID-19 patients, which makes prompt diagnosis important. Endothelial dysfunction can be evaluated by using transcranial Doppler ultrasound to study cerebral hemodynamic reserve, but there are few of these studies in patients with COVID-19, and the technique is not included in COVID-19 action and follow-up guidelines nationally or internationally.
OBJECTIVEEstimate baseline cerebral hemodynamic patterns, cerebral hemodynamic reserve, and breath-holding index in recovered COVID-19 patients.
METHODWe conducted an exploratory study in 51 people; 27 men and 24 women 20–78 years of age, divided into two groups. One group comprised 25 recovered COVID-19 patients, following clinical and epidemiological discharge, who suffered differing degrees of disease severity, and who had no neurological symptoms or disease at the time they were incorporated into the study. The second group comprised 26 people who had not been diagnosed with COVID-19 and who tested negative by RT-PCR at the time of study enrollment. Recovered patients were further divided into two groups: those who had been asymptomatic or had mild disease, and those who had severe or critical disease. We performed transcranial Doppler ultrasounds to obtain baseline and post-apnea tests of cerebral hemodynamic patterns to evaluate cerebral hemodynamic reserve and breath-holding indices. We characterized the recovered patient group and the control group through simple descriptive statistics (means and standard deviations).
RESULTSThere were no measurable differences in baseline cerebral hemodynamics between the groups. However, cerebral hemodynamic reserve and breath-holding index were lower in those who had COVID-19 than among control participants (19.9% vs. 36.8% and 0.7 vs. 1.2 respectively). These variables were similar for patients who had asymptomatic or mild disease (19.9% vs.19.8%) and for those who had severeor critical disease (0.7 vs. 0.7).
CONCLUSIONSPatients recovered from SARS-CoV-2 infection showed decreased cerebral hemodynamic reserve and breath-holding index regardless of the disease’s clinical severity or presence of neurological symptoms. These abnormalities may be associated with endothelial damage caused by COVID-19. It would be useful to include transcranial Doppler ultrasound in evaluation and follow-up protocols for patients with COVID-19.
INTRODUCTION SARS-CoV-2 infects humans by binding its spike protein to angiotensin-converting enzyme 2 (ACE2) receptors expressed in lung, heart, kidney and intestinal cells, and in the vascular tree’s endothelial cells. Direct or immune-mediated viral infection results in endothelial and microvascular dysfunction, one cause of multiple organ involvement in COVID-19.[1‒2]
SARS-CoV-2 spreads via systemic circulation or by passing through the cribriform plate of the ethmoid bone,[3] which can affect brain tissue and result in neurological signs and symptoms.[4,5]
IMPORTANCE Cerebral hemodynamic reserve, an expression of endothelial involvement, is altered in recovered COVID-19 patients. This alteration, which increases stroke risk, can be detected via transcranial Doppler ultrasound.
Varga described multifocal microvascular lesions in the brain and olfactory bulbs in patients who died of COVID-19, but did not find direct viral infection of the brain tissue, so infection or inflammation of the endothelium itself seems to be important.[1]
The cerebral microcirculatory damage that causes endotheliitis in SARS-CoV-2 infection can be diagnosed at a patient’s bedside by evaluating cerebral hemodynamic reserve (CHR) through transcranial Doppler ultrasound. However, the technique is not included in international or domestic action guidelines for addressing acute SARS-CoV-2 infection or recovery, and research on the matter is limited.
Transcranial Doppler ultrasound approximates cerebral hemodynamic study by evaluating flow velocities circle of Willis arteries.[6] The technique has proved a useful diagnostic tool for patients with microvascular disease of different etiologies, in which the cerebral hemodynamic reserve may be abnormal even though the cerebral hemodynamic pattern is within normal ranges. CHR is defined as the ability of arterioles and capillaries to dilate in response to increased neuronal activity or to a metabolic or vasodilator stimulus,[7] which can include CO2 inhalation, acetazolamide administration, and the breath-holding test (BHT). BHT consists of a period of voluntary apnea that causes cerebral vasodilation by secondary increase of CO2 levels.[8,9] The result represents the percentage change of cerebral blood flow velocity from baseline to maximum values. The inclusion of apnea time with BHT more closely approximates CHR, defined as breath-holding index (BHI).[8,10] The decrease in CHR has been linked to greater probability of stroke.[8,11,12]
Considering that abnormalities in cerebral microcirculation can be diagnosed with transcranial Doppler ultrasound, we propose estimating baseline cerebral hemodynamic pattern, CHR and BHI in recovered COVID-19 patients.
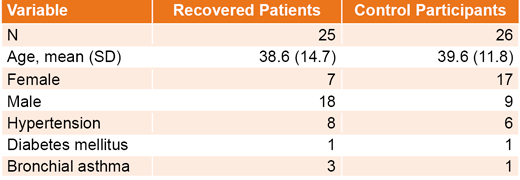
METHODS General study design and sample screening The study universe comprised 51 people, 27 men and 24 women aged 20–78 years, divided into two groups. The first group included 25 participants recovered from COVID-19, who had had different degrees of disease severity and no neurological symptoms or disease at the time of study enrollment. The second group included 26 healthy people with no history of COVID-19, and with negative SARS-CoV-2 real-time polymerase chain reaction (RT-PCR) tests at study enrollment; participants in this group were recruited from the medical and nursing staff of Havana’s Medical Surgical Research Center (CIMEQ).
We enrolled the group of recovered COVID-19 patients from those who came in for follow-up visits, from Februrary through May 2021, two weeks through one month following hospital visits. Patients were admitted to a medical center during their illness with different degrees of COVID-19 clinical severity, as defined by WHO,[13] and were treated according to the Cuban protocol.[14] Participating patients were stratified into two groups: one included asymptomatic patients and those who had mild forms of the disease, and the other included those who had severe forms of the disease.
Of the patients who had recovered from COVID-19, 14 had asymptomatic infections (56%, 14/25), 7 had mild forms of the disease (28%, 7/25), 2 had severe, and 2 had critical forms (16%, 4/25). Of the patients, 3 had experienced headache (12%, 3/25), 2 a decreased sense of smell (8%, 2/25), and 1 loss of taste (4%, 1/25). All were asymptomatic at the time the study was conducted.
The ages, distribution by sex, and comorbidities of the recovered patients and control group are shown in Table 1.
Data acquisition and collection Transcranial Doppler ultrasound (Doppler-Box X1, DWL, Germany) was performed to determine baseline cerebral hemodynamic patterns and estimate cerebral hemodynamic reserve through a BHT following completion of a baseline exam. All studies were conducted by the same evaluator, who has more than 10 years’experience in the technique.
Table 1: Study group demographics and medical history
Baseline recordings and BHTs were performed while the person was lying in a supine position. Vessels were examined using a 2 MHz pulsed-wave Doppler transducer (DWL, Germany). Sample volume of the studied vessel, and gain and selected power were kept constant during the recording. We studied the right and left middle cerebral arteries (MCA) through both temporal windows, at depths of 45–55 mm. The values acquired in the MCAs were used once a bilateral symmetrical pattern was confirmed. MCA blood flow velocities were considered asymmetrical if the difference was greater than 20%. Arterial flow (velocity and spectral waveform) remained constant for at least 30 seconds before recording study variable values.
We evaluated peak systolic velocity (PSV), end diastolic velocity (EDV) and mean velocity (MV) in the baseline hemodynamic pattern.
Once a baseline pattern reading was established, participants were instructed to stop breathing for 30 seconds after taking a normal breath (to avoid a Valsalva maneuver). In the next 5–10 seconds, we obtained the maximum values of the same hemodynamic variables used in the baseline studies. If the participant could not hold his or her breath for 30 seconds, the shortened breath-holding time was recorded.
CHR evaluated by BHT was defined as the percentage increase of post-apnea rMCAMV, and was calculated as the increased percentage of rMCAMV in apnea over baseline rMCAMV. There are no national studies to provide reference values, so we used a control group. Normal reported values differ in the international literature because individual pCO2 varies based on the condition of the person being evaluated.[15]
BHI was calculated by dividing rMCAMV’s increased percentage, averaged out in the time after breath-holding, by seconds of apnea according to the following formula:
BHI = [(apnea rMCAMV – baseline rMCAMV) / (baseline rMCAMV)] x 100] / 30 seconds (or seconds of apnea achieved).
Normal BHI value was established at 1.2 (SD 0.6).[10]
Statistical analysis We estimated the arithmetic means and standard deviations (SD) of quantitative variables, and calculated percentages for the qualitative variables.
Ethics We obtained written informed consent from participants. We maintained patient confidentiality, following the Declaration of Helsinki guidelines on research involving human subjects. Ethics protocols were approved by the scientific and ethical advisory board at the Medical–Surgical Research Center (CIMEQ) in Havana, Cuba.
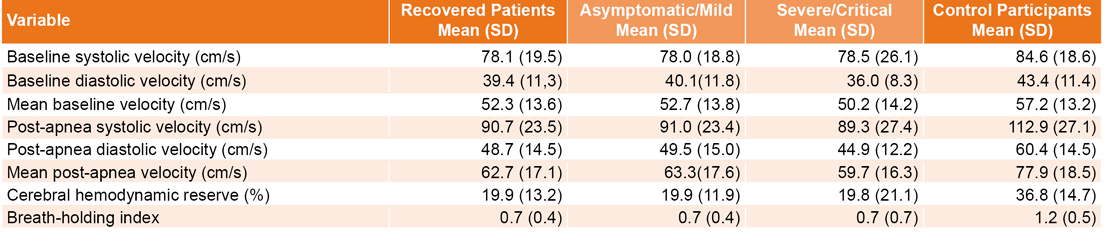
RESULTS Baseline hemodynamic variable means were similar between recovered COVID-19 patients and the control group. The post-apnea hemodynamic pattern variables were lower in the recovered patient group, with lower systolic, diastolic and mean velocities. Mean CHR and mean BHI were lower in recovered patients (Table 2).
Table 2: Baseline and post-apnea cerebral hemodynamic pattern, cerebral hemodynamic reserve and breath-holding index, by study group
Baseline cerebral hemodynamic pattern, post-apnea hemodynamic pattern variables, CHR and BHI were similar in all recovered patients, degree of disease severity notwithstanding (Table 2).
DISCUSSION The endothelium corresponds with cerebral hemodynamic vasoreactivity since the endothelium produces constricting and relaxing factors, based on its integrity. Cerebral hemodynamic reserve may be a marker of endothelial function in cerebral arteries.[16,17]
Hypertensive patients <60 years of age, with no neurological signs or symptoms, with mild white matter conditions diagnosed by MRI, and in whom CHR was decreased, had a progressively higher risk of symptomatic stroke and lacunar infarct chronic vascular lesions than hypertensive patients of the same age with normal CHR.[18]
The endothelium has been called ‘the Achilles’ heel’ of patients with COVID-19.[19] Cytokines and proinflammatory mediators shift endothelial functions from homeostasis to defense,[20] and microvascular lesions found in the brain and olfactory bulbs in patients who died from COVID-19 show that the virus infects brain vessel endothelia and can cause abnormalities in vasoreactivity.[1]
Sonkaya[21] evaluated cerebral hemodynamics in 20 patients hospitalized with COVID-19 who had neurological symptoms (headache, seizures, stroke, alterations in consciousness, ageusia, anosmia) and compared them with control participants. Patients had higher mean MCA velocity and lower CHR—evaluated by BHI with transcranial Doppler ultrasound—than control participants. These results are consistent with ours, the difference being that participants in our study had recovered and did not have neurological symptoms.
Marcic[22] studied cerebral hemodynamics through color-coded transcranial duplex ultrasound and estimated BHI in 25 patients who had recovered from mild COVID-19 (according to WHO classification), who were not hospitalized, and who came in for a neurology visit due to neurological symptoms 28–50 days after a negative SARS-CoV-2 RT-PCR. Patients had lower mean MCA velocities and lower mean BHI values (related to CHR abnormalities), compared with a healthy control group, which is also consistent with our results.
Unlike other studies, ours included patients from the entire range of COVID-19’s clinical forms, several days after hospital discharge, who had no neurological or cardiorespiratory symptoms during CHR and BHI recordings. Therefore, the decrease in these variables indicates that vascular abnormalities remained after the acute phase of the disease had passed, that they continued to exist even though the patients had no neurological manifestations, and that these endothelial abnormalities occurred even with minor damage caused by COVID-19.
As of this writing, there has been no report that the decline in CHR and BHI in asymptomatic recovered patients or patients who had recovered from mild forms of the disease is similar to the rates in those with severe or critical forms of the disease. This is why the findings reported in the previous paragraph are important and constitute one of the main contributions of this research.
It is interesting to note the difference in baseline hemodynamic patterns reported in other research with different study populations.[21,22] In our research, the baseline hemodynamic pattern was normal, and the abnormality was found by evaluating CHR. This finding is consistent with cerebral microvasculature damage that exists in different diseases, including COVID-19.[1,23]
CHR decline is an expression of the endothelial damage that characterizes SARS-CoV-2 infection and is a warning sign of stroke risk[8,11,12] even if patients were absent any neurological signs and symptoms during the disease’s initial clinical presentation or during their recovery period, regardless of COVID-19’s clinical severity.
Convenience sampling did not allow for an equal distribution of patients by sex. Due to the epidemiological situation related to COVID-19, we did not invite healthy individuals who would have to come to the hospital center, possibly putting themselves at risk, to participate in the study. Regarding sex and its influence on CHR, some authors report that CHR is lower in women in response to hypercapnia.[24,25]
Additional studies are needed to confirm these results, but the limited research we do have suggests transcranial Doppler ultrasound should be included for non-invasive neurological monitoring in COVID-19 action protocols and patient studies.
CONCLUSION Patients who have recovered from COVID-19 have CHR and BHI impairment, regardless of initial infection severity and absence of neurological symptoms. This impairment can be attributed to the endothelial damage caused by the viral infection. We recommend including transcranial Doppler ultrasound in treatment protocols for recovering COVID-19 patients to alert providers to patients with elevated risk of stroke.
Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020 May 2;395(10234):1417–8. DOI: 10.1016/S0140-6736(20)30937-5
Mosleh W, Chen K, Pfau SE, Vashist A. Endotheliitis and endothelial dysfunction in patients with COVID-19: its role in thrombosis and adverse outcomes. J Clin Med. 2020 Jun 15;9(6):1862. DOI: 10.3390/jcm9061862
Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem Neurosci. 2020 Apr 1;11(7):995–8. DOI: 10.1021/acschemneuro.0c00122
Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic manifestations of hospitalized patients with Coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020 Jun 1;77(6):683–90. DOI: 10.1001/jamaneurol.2020.1127
Collantes MEV, Espiritu AI, Sy MCC, Anlacan VMM, Jamora RDG. Neurological manifestations in COVID-19 infection: a systematic review and meta-analysis. Can J Neurol Sci. 2021 Jan;48(1):66–76. DOI: 10.1017/cjn.2020.146
Blanco P, Abdo-Cuza A. Transcranial Doppler ultrasound in neurocritical care. J Ultrasound. 2018 Mar;21(1):1–16. DOI: 10.1007/s40477-018-0282-9
Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. 2019 Jul;18(7):684–96. DOI: 10.1016/S1474-4422(19)30079-1
Markus HS, Harrison MJ. Estimation of cerebrovascular reactivity using transcranial Doppler, including the use of breath-holding as the vasodilatory stimulus. Stroke. 1992 May;23(5):668–73. DOI: 10.1161/01.str.23.5.668
Fierstra J, Sobczyk O, Battisti-Charbonney A, Mandell DM, Poublanc J, Crawley AP, et al. Measuring cerebrovascular reactivity: what stimulus to use? J Physiol. 2013 Dec 1;591(23):5809–21. DOI: 10.1113/jphysiol.2013.259150
Marinho CG, Melo HA, Salvatori R, Nunes MAP, Oliveira CRP, Campos VC, et al. Cerebral vasoreactivity, a surrogate marker of cerebrovascular disease, is not impaired in subjects with lifetime, untreated, congenital isolated GH deficiency. Endocrine. 2020 Nov;70(2):388–95. DOI: 10.1007/s12020-020-02415-0
Ju K, Zhong L, Ni X, Cao H, Cheng G, Ding L. Cerebral vasomotor reactivity predicts the development of acute stroke in patients with internal carotid artery stenosis. Neurol Neurochir Pol. 2018 May–Jun;52(3):374–8. DOI: 10.1016/j.pjnns.2017.12.015
Gaba K, Bulbulia R. Identifying asymptomatic patients at high-risk for stroke. J Cardiovasc Surg (Torino). 2019 Jun;60(3):332–44. DOI: 10.23736/S0021-9509.19.10912-3
Settakis G, Lengyel A, Molnár C, Bereczki D, Csiba L, Fülesdi B. Transcranial Doppler study of the cerebral hemodynamic changes during breath-holding and hyperventilation tests. J Neuroimaging. 2002 Jul;12(3):252–8.
Staszewski J, Skrobowska E, Piusińska-Macoch R, Brodacki B, Stępień A. Cerebral and extracerebral vasoreactivity in patients with different clinical manifestations of cerebral small-vessel disease: data from the significance of hemodynamic and hemostatic factors in the course of different manifestations of cerebral small-vessel disease study. J Ultrasound Med. 2019 Apr;38(4):975–87. DOI: 10.1002/jum.14782
Lavi S, Gaitini D, Milloul V, Jacob G. Impaired cerebral CO2 vasoreactivity: association with endothelial dysfunction. Am J Physiol Heart Circ Physiol. 2006 Oct;291(4):H1856–61. DOI: 10.1152/ajpheart.00014.2006
Kozera GM, Dubaniewicz M, Zdrojewski T, Madej-Dmochowska A, Mielczarek M, Wojczal J, et al. Cerebral vasomotor reactivity and extent of white matter lesions in middle-aged men with arterial hypertension: a pilot study. Am J Hypertens. 2010 Nov;23(11):1198–203. DOI: 10.1038/ajh.2010.152
Gladka MM, Maack C. The endothelium as Achilles’ heel in COVID-19 patients. Cardiovasc Res. 2020 Dec 1;116(14):e195–e7. DOI: 10.1093/cvr/cvaa327
Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease. Eur Heart J. 2020 Sep 1;41(32):3038–44. DOI: 10.1093/eurheartj/ehaa623
Sonkaya AR, Öztrk B, Karadaş Ö. Cerebral hemodynamic alterations in patients with Covid-19. Turk J Med Sci. 2021 Apr 30;51(2):435–9. DOI: 10.3906/sag-2006-203
Marcic M, Marcic L, Marcic B, Capkun V, Vukojevic K. Cerebral vasoreactivity evaluated by transcranial color Doppler and breath-holding test in patients after SARS-CoV-2 infection. J Pers Med. 2021 May 6;11(5):379. DOI: 10.3390/jpm11050379
Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. 2019 Jul;18(7):684–96. DOI: 10.1016/S1474-4422(19)30079-1
Tallon CM, Barker AR, Nowak-Flück D, Ainslie PN, McManus AM. The influence of age and sex on cerebrovascular reactivity and ventilatory response to hypercapnia in children and adults. Exp Physiol. 2020 Jul 1;105(7):1090–1101. DOI: 10.1113/EP088293
Mousavi SA, Khourvash F, Asadi B, Karkheiran F. Evaluation of vasomotor reactivity by transcranial Doppler sonography: age and sex related differences in breath holding index in Iranian population. J Res Medical Sci. 2005 Mar;10(2):93–6.
THE AUTHORS
Anselmo Antonio Abdo-Cuza (Corresponding author: aaabdo@infomed.sld.cu) physician with dual specialties in emergency medicine and intensive care, a master’s degree in emergency medicine, and a doctorate in medical sciences. Medical–Surgical Research Center (CIMEQ), Havana, Cuba. https://orcid.org/0000-0001-5573-7382
Charles Hall-Smith, internist with master’s degrees in atherosclerosis and emergency medicine, CIMEQ, Havana, Cuba. https://orcid.org/0000-0002-9198-7167
Roberto Castellanos-Gutiérrez, physician with dual specialties in emergency medicine and intensive care, and a master’s degree in emergency medicine, CIMEQ, Havana, Cuba. https://orcid.org/0000-0001-6778-6042
Rafael Machado-Martínez, physician with dual specialties in emergency medicine and intensive care, CIMEQ, Havana, Cuba. http://orcid.org/0000-0003-0367-082X
Jonathan Pi-Ávila, physician with dual specialties in emergency medicine and intensive care, CIMEQ, Havana, Cuba. https://orcid.org/0000-0002-1123-1846
Francisco Gómez-Peire, physician with dual specialties in emergency medicine and intensive care, CIMEQ, Havana, Cuba. https://orcid.org/0000-0002-0821-0649
Namibia Espinosa-Nodarse, physician with dual specialties in emergency medicine and intensive care, and a master’s degree in emergency medicine, CIMEQ, Havana, Cuba. https://orcid.org/0000-0003-4455-7639
Juan Carlos López-González, physician with dual specialties in emergency medicine and intensive care, and a master’s degree in emergency medicine, CIMEQ, Havana, Cuba. https://orcid.org/0000-0001-6584-6574
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.