INTRODUCTION The percentage of asymptomatic COVID-19 cases worldwide is estimated at 18–50%; 53% in Cuba specifically, and 58% in Havana, the Cuban capital and the 2020 epicenter of the country’s COVID-19 epidemic. These figures, however, do not represent the transmission capacity or behavior of asymptomatic cases. Understanding asymptomatic transmission’s contribution to SARS-CoV-2 spread is of great importance to disease control and prevention.
OBJECTIVE Identify the epidemiological implications of asymptomatic SARS-CoV-2 infection in Havana, Cuba, during the first wave of the epidemic in 2020.
METHODS We carried out a cross-sectional study of all confirmed COVID-19 cases diagnosed in Havana, Cuba, from March 16 through June 30, 2020. The information was obtained through review of the standardized form for investigation of suspected and confirmed cases. Examined variables included age, sex, occupation, case type and source of infection. Cases were divided into asymptomatic and symptomatic groups, and transmission was characterized through the creation of a contact matrix. Analysis was carried out in Epidat and R.
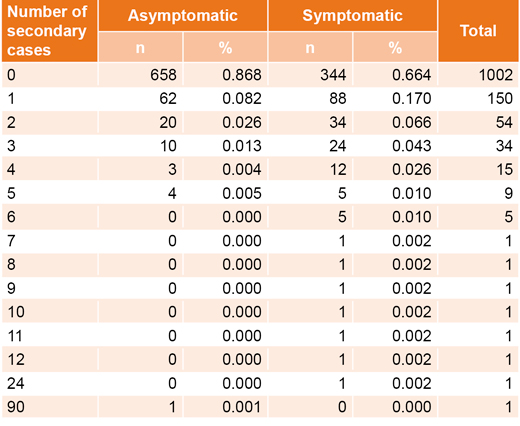
RESULTS We studied 1287 confirmed cases, of which 57.7% (743) were asymptomatic, and 42.3% (544) were symptomatic. Symptomatic presentation was the most common for both imported and introduced cases, while asymptomatic presentation was more common in autochthonic cases and infections from an undetermined source. Asymptomatic infection was more common in groups aged <20 and 20–59 years, while symptomatic infection was more common in those aged >60 years. In the contact matrix, 34.6% of cases (445/1287) were not tied to other cases, and 65.4% (842/1287) were infectious–infected dyads, with symptomatic–symptomatic being the most common combination. The majority of primary cases (78.5%; 1002/1276) did not generate secondary cases, and 85.6% (658/743) of asymptomatic cases did not lead to other cases (although one asymptomatic superspreader led to 90 cases in a single event). However, 63.2% (344/544) of symptomatic primary cases generated secondary cases, and 11 symptomatic superspreaders spawned 100 secondary cases in different events.
CONCLUSIONS Asymptomatic SARS-CoV-2 infection was the most common form of COVID-19 in Havana during the study period, but its capacity for contagion was lower than that of symptomatic individuals. Superspreader events under specific conditions played an important role in sustaining the epidemic.
KEYWORDS COVID-19, SARS-CoV-2, pandemics, asymptomatic infection, Cuba
ABSTRACT INTRODUCTION The percentage of asymptomatic COVID-19 cases worldwide is estimated at 18–50%; 53% in Cuba specifically, and 58% in Havana, the Cuban capital and the 2020 epicenter of the country’s COVID-19 epidemic. These figures, however, do not represent the transmission capacity or behavior of asymptomatic cases. Understanding asymptomatic transmission’s contribution to SARS-CoV-2 spread is of great importance to disease control and prevention.
OBJECTIVEIdentify the epidemiological implications of asymptomatic SARS-CoV-2 infection in Havana, Cuba, during the first wave of the epidemic in 2020.
METHODSWe carried out a cross-sectional study of all confirmed COVID-19 cases diagnosed in Havana, Cuba, from March 16 through June 30, 2020. The information was obtained through review of the standardized form for investigation of suspected and confirmed cases. Examined variables included age, sex, occupation, case type and source of infection. Cases were divided into asymptomatic and symptomatic groups, and transmission was characterized through the creation of a contact matrix. Analysis was carried out in Epidat and R.
RESULTSWe studied 1287 confirmed cases, of which 57.7% (743) were asymptomatic, and 42.3% (544) were symptomatic. Symptomatic presentation was the most common for both imported and introduced cases, while asymptomatic presentation was more common in autochthonic cases and infections from an undetermined source. Asymptomatic infection was more common in groups aged <20 and 20–59 years, while symptomatic infection was more common in those aged >60 years. In the contact matrix, 34.6% of cases (445/1287) were not tied to other cases, and 65.4% (842/1287) were infectious–infected dyads, with symptomatic–symptomatic being the most common combination. The majority of primary cases (78.5%; 1002/1276) did not generate secondary cases, and 85.6% (658/743) of asymptomatic cases did not lead to other cases (although one asymptomatic superspreader led to 90 cases in a single event). However, 63.2% (344/544) of symptomatic primary cases generated secondary cases, and 11 symptomatic superspreaders spawned 100 secondary cases in different events.
CONCLUSIONSAsymptomatic SARS-CoV-2 infection was the most common form of COVID-19 in Havana during the study period, but its capacity for contagion was lower than that of symptomatic individuals. Superspreader events under specific conditions played an important role in sustaining the epidemic.
KEYWORDSCOVID-19, SARS-CoV-2, pandemics, asymptomatic infection, Cuba
INTRODUCTION Research on COVID-19, the disease caused by the SARS-CoV-2 virus, is evolving, addressing questions like different transmission routes, the infectious dose (the amount of virus required for transmission), the characteristics of those most susceptible to infection, situations that facilitate contagion events, the proportion of individuals who remain asymptomatic throughout the course of infection, the specific factors that drive asymptomatic and pre-symptomatic transmission, as well as the proportion of infections transmitted by asymptomatic and pre-symptomatic individuals.[1]
The overall percentage of COVID-19 cases that are pre-symptomatic (infected individuals who are currently asymptomatic but will present with symptoms during a later stage of infection) or asymptomatic (individuals who will never present symptoms) is estimated at 18%–50% worldwide, although this figure has been much higher in certain contexts.[1–3] The data available in Cuba for the first three months of the epidemic (whose first case was officially reported on March 11, 2020) place the proportion at about 53% of all confirmed cases nationwide,[4] and about 58% of all cases diagnosed in Havana.[5]
IMPORTANCE Identification of asymptomatic SARS-CoV-2 infection and its role in COVID-19 spread and transmission contributed to the implementation of effective disease control measures in Havana, Cuba during the pandemic’s first wave in 2020.
The aforementioned data, however, represent the total proportion of asymptomatic or pre-symptomatic COVID-19 cases, and not the role of asymptomatic patients in SARS-CoV-2 transmission. According to a study by the University of Padua and the Imperial College of London, asymptomatic COVID-19 patients are about as infectious as symptomatic patients,[6] but there are still no reliable estimates of the contagiousness of asymptomatic individuals as compared with symptomatic individuals.
Due to its clinical importance, an understanding of the magnitude of the role asymptomatic transmission plays in the spread of SARS-CoV-2 is much needed. Additionally, it cannot be assumed that a lack of symptoms means there is no harm being done to the asymptomatic individual.[7] A thorough understanding of asymptomatic transmission is also important from an epidemiological point of view, as the diagnosis, confirmation and subsequent isolation of symptomatic cases (as established in Cuban national action protocols for case and contact management)[8]—if not accompanied by similar measures for asymptomatic cases—may have a limited effect in reducing overall community transmission.
The basic reproduction number R0 (the average number of secondary infections caused by a primary case in an epidemiologically naïve population) for SARS-CoV-2 person-to-person transmission was estimated at two to three cases, for the original wild-type virus circulating when this study was done. Fewer secondary cases have been reported in some countries than would have been expected with this R0, suggesting that not all primary cases cause secondary transmission.[9,10] Some literature suggests that 10%–20% of infected individuals are responsible for 80%–90% of all transmitted cases.[10,11]
All of this suggests the need for epidemiological studies estimating not only R0 for asymptomatic SARS-CoV-2–positive individuals (estimated as 1%; 95% CI: 0%−2%), but also other important parameters such as the k dispersion parameter, a measure of person-to-person transmission variation that is especially important in calculating superspreader events in which a single person infects tens or hundreds of others.[11,12]
Given the importance of this information for pandemic control, this article explores asymptomatic and presymptomatic transmission in the Havana pandemic epicenter during the first half of 2020, although the authors recognize that these epidemiological parameters have changed both in Cuba and worldwide with the appearance of new SARS-CoV-2 variants.
METHODS Study design and participants We carried out a descriptive cross-sectional study that included all confirmed SARS-CoV-2–positive cases in Havana, Cuba, from March 16 (following the declaration of the first cases in Cuba and the beginning of the Cuban epidemic) through June 30, 2020 (the end of the first wave of the Cuban epidemic).
Study variables The following sociodemographic variables were collected: age (≤20 years, 21–59 years, ≥60 years); sex (male or female); and occupation (health worker or other).
We also included the following clinical variables:
Asymptomatic case: a case manifesting no signs or symptoms of the disease at diagnosis.
Symptomatic case: a case manifesting signs and symptoms compatible with any of the five clinical forms recognized by WHO and included in the COVID-19 Cuban protocol (uncomplicated or mildly symptomatic disease, uncomplicated lower respiratory tract infection or mild pneumonia, acute respiratory distress syndrome, sepsis, or septic shock syndrome).[8]
Confirmed case: any patient who tested positive for SARS-CoV-2, with or without symptoms.
The epidemiological variables were:[8]
Case type: index case defined as the one that introduces an infection into a group or population; primary case, defined as the first case identified in an outbreak or event, capable of generating other cases, the recognition of which is generally retrospective; or secondary case, defined as any case infected by a primary or index case.
Number of secondary cases: secondary cases generated by primary cases; any primary case that generated ≥6 secondary cases was considered to be a superspreader.
Conditions facilitating contagion: places facilitating close contact (≤1 meter between persons), such as those with high concentrations of people, high social mobility, enclosed places with limited ventilation, and detention centers.
Source of infection: imported if the known source of infection occurred outside Cuba; introduced, if infection occurred through contact with travelers from abroad; autochthonous, when infection was acquired locally via contact with confirmed cases, or cases of unknown infectious sources, if no relationship to other cases was identified.
Country of origin: any country as a probable source of infection pertaining to cases included in the sample.
Procedures, data collection and management Sociodemographic, clinical, and epidemiological data were obtained through a document review of primary sources (the standard form specifically designed for investigation of suspected and confirmed COVID-19 cases, results of which are housed in Havana province’s database of confirmed cases at the Provincial Hygiene, Epidemiology and Microbiology Center, the quality and reliability of which was refined by, and compatible with, Cuba’s national database of confirmed cases, housed in the Ministry of Public Health, MINSAP).
We selected confirmed COVID-19 cases in Havana from the country’s database and established two study groups: symptomatic and asymptomatic. We recorded the symptom onset date for symptomatic cases, and the confirmation date for each patient, regardless of whether they were symptomatic or not.
We constructed a contact matrix or transmission tree for all cases to characterize both the groups and their transmission routes. To do this, we identified isolated cases, or primary–secondary contact pairs (infective–infected) in which both cases were symptomatic, both were asymptomatic, or only one patient was symptomatic. Contact matrices (epidemiological networks) were constructed with the index, primary and secondary cases forming part of either outbreaks (defined as ≤9 secondary cases) or events (≥10 generated cases); a few of which included superspreader cases.
We performed a percentage analysis of asymptomatic and symptomatic cases, according to age, sex, occupation and infection source, and bivariate analyses through calculation of prevalence ratios with 95% confidence intervals. The dispersion threshold was calculated using the 99th percentile of the Poisson distribution (λ = R0) where Pr (Z ≤ Z(99)|Z ~ Poisson(R0) = 0.01; where R0 is the baseline reproductive number and Z is the number of secondary cases derived from an infected person in a susceptible population.[12] Given that the value of R0 for COVID-19 (wild-type) has been estimated at 2–3,[7,9,10] the superspreader threshold was established at Z = 6 secondary cases. From this value, all subjects who generated six or more secondary cases were considered superspreaders.
For transmission chains, the effective reproduction number (R) was estimated from the negative binomial distribution’s mean adjusted to the distribution of observed secondary cases.[12] This was completed for all pairs within the matrix clusters and for purposes of comparison, was additionally completed for all chains started by symptomatic and asymptomatic cases.
Statistical analysis Data analysis was performed in EPIDAT 3.1 and R, version 3.4.0 (SERGAS, Spain, 2017) with 95% confidence intervals (CI).
Ethical considerations This study was approved by the Specialized Scientific Commission for Epidemiology and the Pedro Kourí Tropical Medicine Institute’s Ethics Committee, as well as Havana’s Provincial Hygiene, Epidemiology and Microbiology Center. Patient anonymity was guaranteed; informed consent was unnecessary, as only information excluding patient identity from the Ministry of Public Health’s database was utilized.
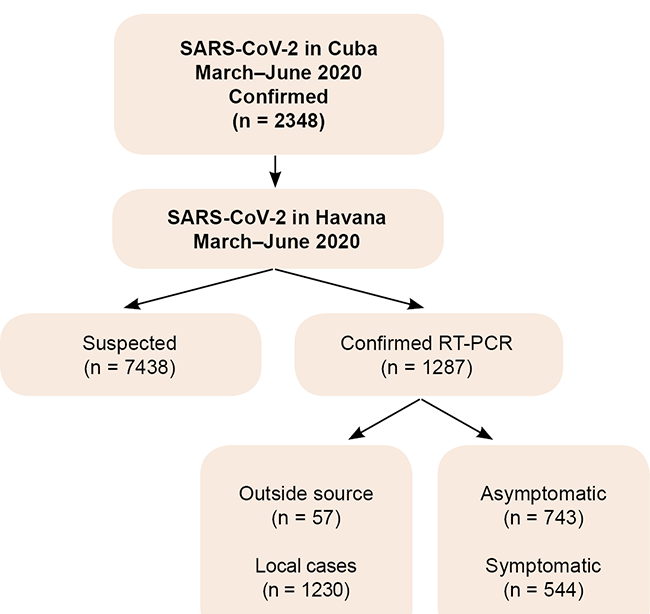
RESULTS As of June 30, 2020 (statistical week 27), 7438 suspected COVID-19 cases had been studied in Havana’s molecular biology laboratories, of which 1287 (17.3%) were confirmed positive by RT-PCR (real-time polymerase chain reaction). Of this total, 743 (57.7%) were asymptomatic, while 544 (42.3%) had various clinical symptoms (Figure 1).
Figure 1: Confirmed SARS-CoV-2 case distribution, according to presentation and infection source. Havana, Cuba, March–June, 2020
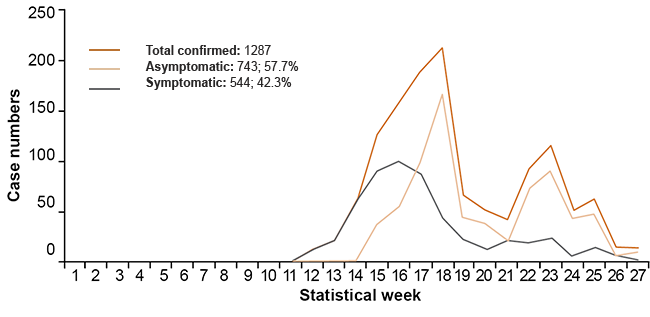
Symptomatic cases were the most common during the beginning of the epidemic, from the confirmation of the first case on March 16 (statistical week 12), until statistical week 16 (April 12–18.) After this period, asymptomatic cases were the most common. This pattern was maintained until the end of the study period (Figure 2).
Figure 2: Distribution of asymptomatic and symptomatic SARS-CoV-2 cases by statistical week. Havana, Cuba, March–June, 2020
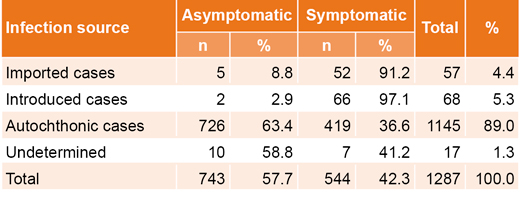
Autochthonous infection was predominant at 89.0% of all cases (1145/1287). In imported and introduced cases, symptomatic infection was the most prevalent, at 91.2% (52/57) and 97.1% (66/68), respectively, while autochthonous cases (63.4%; 726/1145) or cases without a specified infection source (58.8%; 10/17) were most commonly asymptomatic (Table 1).
Among the 15 countries that contributed imported cases, Spain was the most represented (22.8%; 13/57), followed in order of frequency by the USA (15.8%; 9/57), Mexico (12.3%; 7/57), France and Panama (both of which were 10.5%; 6/57of cases). Between one and three cases were identified for each of the other countries listed.
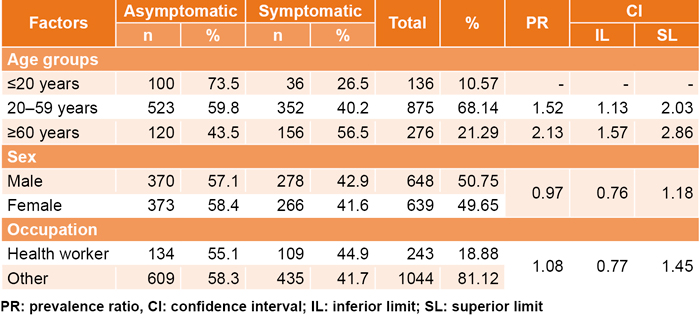
Confidence intervals for the prevalence ratios (PR) for sex and occupation in symptomatic cases contained the value 1, which is not the case for individuals ≥60 years of age, which have a remarkably higher likelihood (2.13) of being symptomatic than individuals aged ≤20 years. Asymptomatic infection was most common in individuals <60, while adults ≥60 were more likely to be symptomatic (Table 2).
The contact matrix allowed us to identify 445 isolated cases (34.6% of the total) and 842 interrelated cases (65.4%), for a total of 644 infector–infected dyads, among which symptomatic–symptomatic pairings were the most common (144/644; 22.4%).
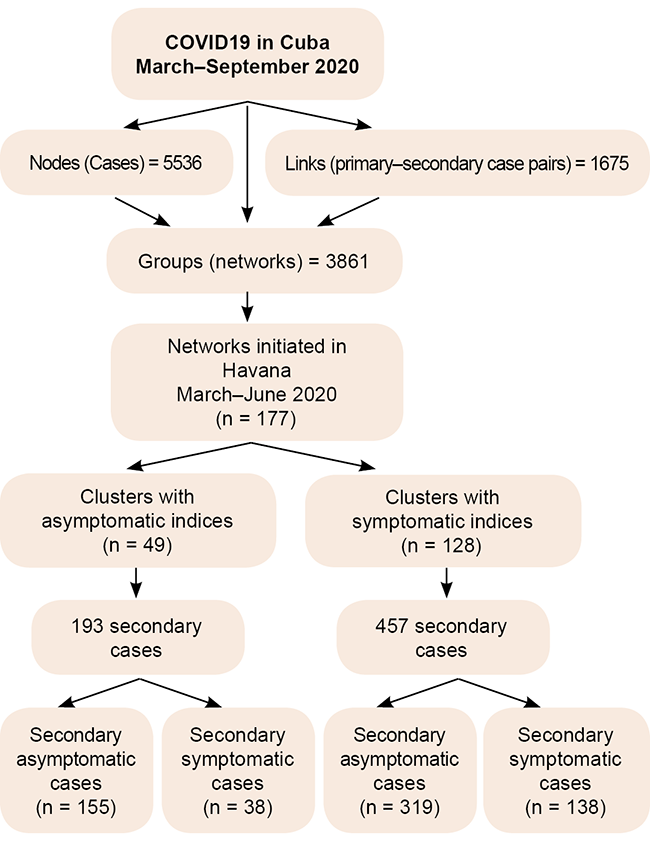
During the study period, 177 transmission chains or clusters began in Havana, 49 of which had an asymptomatic individual as the first case, while 128 were initiated by a symptomatic case (Figure 3). Clusters with asymptomatic primary cases generated a smaller number of secondary cases (193), of which 80.3% were asymptomatic (155/193). Clusters generated by symptomatic individuals resulted in 457 secondary cases, of which 69.8% were also asymptomatic (319/457).
Table 1: Asymptomatic and symptomatic case distribution, according to infection source
Table 2: Asymptomatic and symptomatic case distribution, according to age, sex and occupation; prevalence ratios and 95% confidence intervals
Among asymptomatic cases, a single individual was identified as a superspreader who generated 90 secondary cases in a single event (closed internment institution). Among symptomatic cases, 11 primary cases acted as superspreaders, leading to 100 secondary cases, related to either high social mobility, close contact between individuals in closed spaces with limited ventilation, or places with high concentrations of people (Table 3).
Figure 3: General contact matrix of confirmed SARS-CoV-2 cases. Havana, Cuba, March–June, 2020
We obtained a global value of the effective reproductive number (R = 0.51; 95% CI: 0.43–0.60), which was lower in the asymptomatic group (R = 0.34; 95% CI: 0.25–0.44) compared to the symptomatic group (R = 0.77; 95% CI: 0.65–0.91).
DISCUSSION Claims that asymptomatic and pre-symptomatic transmission represent the main source of the pandemic’s spread[13,14] are debatable, particularly given the emergence of new virus variants and new strategies to address them. What is not in doubt is the high proportion of asymptomatic individuals that are carriers of the virus in different contexts,[15–17] so research is essential to determine the true role of asymptomatic carriers in SARS-CoV-2 transmission.
The upward linear trend in asymptomatic case notification in Havana during the epidemic’s first wave was similar to that reported by other national[4,5,18] and international studies;[6,19,20] but differed from reports from researchers in Korea[21] and China.[22]
By the time this study was done, Cuba’s national strategy, contained in the country’s national action protocols for all phases and stages of the pandemic,[8] included extensive research at the primary care level: testing everyone who had either direct or indirect contact with a confirmed case; isolation of all suspected or confirmed cases in hospitals, regardless of the presence or absence of symptoms; quarantine of contacts of confirmed cases in isolation centers; epidemiological surveillance of travelers; and other control measures in accordance with WHO guidelines.[23] Most of these protocols, with the exception of strict isolation measures, are still in effect.
Table 3: Asymptomatic and symptomatic primary case distribution, according to secondary case generation
A shift in transmission from a predominance of symptomatic to asymptomatic cases during the first wave was likely due to
increased diagnostic capacity and contact tracing, in which more asymptomatic and pre-symptomatic cases were counted that would have gone undetected at the very beginning of the pandemic. At the same time, there was wide community transmission and defined diagnostic testing criteria, in an asymptomatic population that was mostly young and healthy and associated with more benign clinical progression.
This situation continued until the end of 2020, when borders closed due to the pandemic began to open, and cases in foreign visitors and Cubans visiting from abroad introduced new SARS-CoV-2 variants, which are associated with more severe forms of COVID-19 that are more likely to be symptomatic,[24] a situation that has continued through 2021.
The first Cuban travel restrictions were implemented on March 21, 2020, and borders were definitively closed on April 7, 2020.[25] Most cases were either imported or introduced during this period. From then on, outbreaks in closed communities or institutions, where confirmed cases were not linked to travelers from affected areas, suggest that autochthonous transmission was a fundamental aspect of the pandemic, confirmed by this and other national studies.[4,5,18,26,27]
The observation that imported and introduced cases mainly presented as symptomatic before the borders were closed could be related to the fact that Cuba’s epidemiological surveillance system during the very beginning of the pandemic defined a ‘suspected case’ of COVID-19 as an individual who presented with symptoms compatible with COVID-19 who came from countries or territories with documented transmission. After studies began of all contacts, identification and diagnosis of asymptomatic cases increased, which led to a change in the definition of ‘suspected case.’
SARS-CoV-2 can affect people of all ages. In this instance, both globally and within groups, infection was more common in middle-aged adults, similar to results found in additional studies in Cuba,[5,18] and other countries,[2,28] with the exception of those carried out in Santiago de Cuba[26] and Camagüey[27] provinces, in which older adults were more susceptible to infection. These results could be due to the fact that middle-aged adults comprise the group with the highest levels of social interaction, as they continue to work and carry on family activities, while children remained at home after schools were closed and older adults self-isolated, among other posible causes.[2]
In our study, asymptomatic infection was most common in individuals <60 years of age, while older adults were more likely to manifest the disease symptomatically. This result is consistent with other literature on the same period of the pandemic, in which children were generally less susceptible to infection and manifested milder symptoms than adults, suggesting however that they posed a high risk of transmitting the disease through asymptomatic presentation. In adults, advanced age is directly correlated with greater risk of infection, as well as more severe clinical presentations, and death.[29–33]
In some studies, the highest rates of infection were reported among men,[5,33,34] while others report the opposite.[26] In this study, both sexes showed the same probability of becoming infected and presenting with symptomatic (or asymptomatic) forms.
According to official information published in the Cuban media,[35,36] health workers (during the study period) were not among the risk groups with the highest SARS-CoV-2 infection rates, nor did theirs compare with such rates in other countries. Public health programming within the country led to increased staff awareness and compliance with biosafety protocols. The proportion of cases with occupations outside the healthcare sector was higher in this study; however, the overall proportion of symptomatic and asymptomatic cases was similar in both groups.
The degree to which SARS-CoV-2–positive individuals spread the virus depends to a great extent on environmental and seasonal conditions, and social behavior.[37] COVID-19 transmission dynamics are characterized by the fact that much of disease’s spread is due to a small group of infected individuals.[38]
The epidemiological networks and transmission chains of each group in this study led to the identification of a lower R0 among asymptomatic cases, with a lower percentage of transmission chains initiated by asymptomatic individuals, which translates directly into generation of a smaller number of secondary cases; a finding in direct contrast with one Chinese study,[11] and similar to that found by Ruiz Nápoles in Cuba’s Holguín province and another study performed in China during the beginning of the epidemic.[39,40]
We also found that superspreader events occurred more often among symptomatic patients, except for one asymptomatic superspreader case that occurred in a closed internment institution.
The results of this study affirm that it is not possible to know in advance which persons have the ability to transmit the infection, so from an epidemiological point of view it is advisable to promote and respect measures to avoid specific socio-environmental conditions that favor transmission: not frequenting crowded public places or closed spaces with poor ventilation, maintaining physical distancing, masking, and frequent hand washing in all circumstances.
In agreement with Nishiura,[41] estimating the percentage of asymptomatic cases and their role in the spread of the epidemic has substantially expanded knowledge of the disease, and has improved understanding of SARS-CoV-2 transmission.
New SARS-CoV-2 variants of concern Molecular surveillance carried out by the Pedro Kourí Tropical Medicine Institute in Havana has shown that COVID-19 transmission patterns in Cuba during the beginning of the epidemic were similar to those in Wuhan, China. During almost all of 2020, the mutation in position 614 (D614G) was the most common, coinciding with the period in which asymptomatic or pre-symptomatic infection was the most predominant form of infection. After borders re-opened in November 2020, the alpha and beta variants of concern (VOCs) were identified and later isolated in all Cuban provinces. VOC beta was associated with significant increases in case numbers and with case severity in certain regions, including Havana and Jagüey Grande, Matanzas province. This situation worsened after the introduction of VOC delta, first identified in a traveler at the end of April 2021 and detected in local transmission cases by May. Within a short period of time, this variant spread throughout most provinces, especially Havana, Matanzas, Ciego de Ávila, Cienfuegos, Holguín and Guantánamo.[42,43] Delta’s rapid extension—associated with characteristics that facilitate greater transmissibility—led to its predominance over other variants, including beta, also the case in the Americas.[44]
The change caused by the new variants in the proportion of symptomatic and asymptomatic cases at the time of diagnosis is remarkable. In 2020, asymptomatic patients exceeded 70% of all patients during certain periods, while by the end of August 2021, asymptomatic cases represented only 5% of daily confirmed cases.[42] The increase in the proportion of symptomatic cases, together with a shortening incubation period, an increase in viral load and lengthened transmissibility periods suggest that the contribution of symptomatic cases could continue to be an important factor in community transmission of SARS-CoV-2 compared with asymptomatic transmission, as was observed in 2020.
Study limitations As we used information from the Cuban database of confirmed cases, pre-symptomatic cases may have been included in the asymptomatic case group, as there was no clinical follow-up as to whether these cases became symptomatic. It was also not possible to calculate disease attack rates, as it would have been necessary to know the exposed population in each epidemiological network.
CONCLUSIONS Asymptomatic SARS-CoV-2 infection was the most common form of COVID-19 in Havana during the study period, and such individuals were less likely to spread the infection than those who were symptomatic. Superspreader events, most likely under specific conditions, played an important role in sustaining the epidemic.
United Nations [Internet]. New York: United Nations; c2021. Noticias ONU. ¿Cómo se transmite el coronavirus que causa COVID-19? 2020 Jul 9 [cited 2020 Jul 27]; [about 5 p.]. Available at: https://news.un.org/es/story/2020/07/1477231. Spanish.
Venero-Fernández SJ, Más-Gómez M, Cuellar-Luna L, de Armas-Águila Y, Suárez-Medina R, Pérez-González DR, et al. Características epidemiológicas de la COVID-19 en La Habana, epicentro de Cuba. Rev Cubana Hig Epidemiol [Internet]. 2021 Feb 27 [cited 2021 Apr 13];58. Available at: http://www.revepidemiologia.sld.cu/index.php/hie/article/view/1025. Spanish.
Mizumoto K, Kagaya K, Zarebski A, Chowell G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance [Internet]. 2020 Mar 12 [cited 2020 Jul 7];25(10):2000180. Available at: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.10.2000180
Zhao S, Lin Q, Ran J, Musa SS, Yang G, Wang W, et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: a data-driven analysis in the early phase of the outbreak. Int J Infect Dis [Internet]. 2020 Mar [cited 2021 Feb 15];92:214–7. Epub 2020 Jan 30. Available at: https://www.sciencedirect.com/science/article/pii/S1201971220300539
Endo A, Abbott S, Kucharsky AJ, Funk S; Center for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group. Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China. Wellcome Open Res [Internet]. 2020 Jul 10 [cited 2021 Feb 15];5(67). Available at: https://doi.org/10.12688/wellcomeopenres.15842.3
Chi Q, Hu Y, Peng B, Tang XJ, Wang W, Su K, et al. Effective control of SARS-CoV-2 transmission in Wanzhou, China. Nat Med [Internet]. 2021 Jan [cited 2021 Feb 15];27(1):86–93. Available at: https://doi.org/10.1038/s41591-020-01178-5
Lloyd-Smith JO, Schreiber SJ, Kopp PE, Getz WM. Superspreading and the effect of individual variation on disease emergence. Nature. 2005;438(7066):355–9.DOI: 10.1038/nature04153
Rodríguez Labrada R, Vázquez-Mojena Y, Velázquez-Pérez L. Transmisión asintomática y presintomática del SARS-CoV-2: la cara oculta de la COVID-19. An Acad Ciencias Cuba [Internet]. 2020 [cited 2020 May 4];10(2). Available at: http://www.revistaccuba.cu/index.php/revacc/article/view/770. Spanish.
Martínez Gandolfi A, Rodríguez Mir J. Asintomáticos COVID-19 excluidos de protocolo. Aten Primaria [Internet]. 2021 Jan 21 [cited 2021 Jul 27];53(1):118–9. Available at: https://doi.org/10.1016/j.aprim.2020.06.005
Nishiura H, Kobayasi T, Miyama T, Suzuki A, Jung SM, Hayashi K, et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int J Infect Dis [Internet]. 2020 May;94:154–5. DOI: 10.1016/J.IJID.2020.03.020. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/32179137/
Song H, Xiao J, Qiu J, Yin J, Yang H, Shi R, et al. A considerable proportion of individuals with asymptomatic SARS-CoV-2 infection in Tibetan population. medRxiv [Preprint]. Available at: https://doi.org/10.1101/2020.03.27.20043836
Noriega V, Pría MC, Corral A, Alvarez ME, Bonet M. La infección asintomática por el SARS-CoV-2: evidencias para un estudio poblacional en Cuba. Rev Cubana Salud Pública [Internet]. 2020 [cited 2020 Nov 25];46 (Suppl):e2707. Available at: http://www.revsaludpublica.sld.cu/index.php/spu/article/view/2707. Spanish.
Rongrong Y, Xien G, Xiong Y. Comparison of clinical characteristics of patients with asymptomatic vs symptomatic Coronavirus disease 2019 in Wuhan, China. JAMA Network Open [Internet]. 2020;3(5):e2010182.DOI: 10.1001/jamanetworkopen.2020.10182. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7254178/
Lee S, Kim T, Lee E, Lee C, Kim H, Rhee H, et al. Clinical Course and Molecular Viral Shedding Among Asymptomatic and Symptomatic Patients With SARS-CoV-2 Infection in a Community Treatment Center in the Republic of Korea. JAMA Intern Med [Internet]. 2020 Aug 6;180(11):1447–52. Available at: DOI: 10.1001/jamainternmed.2020.3862
Yang R, Gui X, Xiong Y. Comparison of clinical characteristics of patients with asymptomatic vs symptomatic Coronavirus disease 2019 in Wuhan, China. JAMA Netw Open. 2020 May 1;3(5):e2010182. DOI: 10.1001/jamanetworkopen.2020.10182.
Ferrer Castro JE, Sánchez Hernández E, Poulout Mendoza A, del Río Caballero G, Figueredo Sánchez D. Caracterización clínica y epidemiológica de pacientes confirmados con la COVID-19 en la provincia de Santiago de Cuba. MEDISAN [Internet]. 2020 [cited 2020 Jun 16];24(3). Available at: http://medisan.sld.cu/index.php/san/article/view/3145. Spanish.
Medina-Fuentes G, Carbajales-León EB, Figueredo-González Y, Carbajales-León AI, Silva-Corona I. Características clínico epidemiológicas de pacientes positivos a la COVID-19 pertenecientes al policlínico “Joaquín de Agüero y Agüero”, Camagüey. Rev Electrón Dr. Zoilo E. MarinelloVidaurreta [Internet]. 2020 [cited 2020 Nov 25];45(4). Available at: http://www.revzoilomarinello.sld.cu/index.php/zmv/article/view/2352/0. Spanish.
Kronbichler A, Kresse D, Yoon S, Hwa Lee K, Effenberger M, Shin JI. Asymptomatic patients as a source of COVID-19 infections: a systematic review and meta-analysis Int J Infect Dis [Internet]. 2020 Sep 1 [cited 2020 Nov 25];98:180–6. Available at: https://doi.org/10.1016/j.ijid.2020.06.052
Cheung KS, Hung IFN, Chan PPY, Lung KC, Tso E, Liu R, et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from the Hong Kong cohort and systematic review and meta-analysis. Gastroenterology [Internet]. 2020 Jul [cited 2021 May 19];159(1):81–95. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/32251668/
Zimmermann P, Curtis N. Coronavirus infections in children including COVID-19. An overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr Infect Dis J [Internet]. 2020 [cited 2020 Dec 4]; 39:355–68. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/32310621/
Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection in children and adolescents. A systematic review. JAMA Pediatrics [Internet]. 2020 [cited 2021 May 19]. Available at: https://jamanetwork.com/journals/jamapediatrics/fullarticle/2765169
Shekerdemian SL, Mahmood NR, Wolfe KK, Riggs B, Ross C, McKiernan C, et al. Characteristics and outcomes of childrens with Coronavirus disease 2019 (Covid 19) infection admitted to US and Canadian pediatric intensive care units. JAMA Pediatr [Internet]. 2020 Sep 1 [cited 2021 May 19]. Available at: https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2020.1948
Betancourt J, Vázquez R, Acao François L. Determinación de patrones de contactos para enfermedades de transmisión aérea en comunidades de Camagüey. Cuba. Rev Cubana Hig Epidemiol [Internet]. 2011 Jan–Apr [cited 2020 Nov 25];49(1):4–14. Available at: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-30032011000100002. Spanish.
Ruiz Nápoles JB, Ruiz Nápoles K. Comparación de las características clínicas y epidemiológicas entre pacientes asintomáticos y sintomáticos con la COVID-19. Rev Cubana Med Milit [Internet]. 2021 Apr 19 [cited 2020 Aug 20];50(2). Available at: http://www.revmedmilitar.sld.cu/index.php/mil/article/view/919. Spanish.
Nishiura H, Kobayashi T, Miyama T, Suzuki A, Jung SM, Hayashi K, et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int J Infect Dis. 2020 May;94:154–5. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/32179137/
Pan American Health Organization; World Health Organization. COVID-19 Report 72. Havana: Pan American Health Organization; World Health Organization; 2021 Jun 28. Spanish.
Pan American Health Organization; World Health Organization. Variantes de SARSCoV-2 en las Américas. Washington, D.C.: Pan American Health Organization; World Health Organization; 2021 Aug 8. Spanish.
THE AUTHORS Elba Cruz-Rodríguez (Corresponding author: elba@ipk.sld.cu, elbacr@infomed.sld.cu), physician specializing in family medicine and epidemiology, with a master’s degree in epidemiology. Associate professor and adjunct researcher, Pedro Kourí Tropical Medicine Institute (IPK). IPK’s Research, Diagnostics and Reference Center (CIDR), Epidemiological Surveillance and Research Department, Havana, Cuba. https://orcid.org/0000-0002-1134-6571
Waldemar Baldoquín-Rodríguez, physician specializing in family medicine and biostatistics. Assistant professor and adjunct researcher, Epidemiological Surveillance and Research Department, CIDR, IPK, Havana, Cuba. https://orcid.org/0000-0001-9231-7109
Niurka Molina-Águila, physician specializing in family medicine and epidemiology, with a master’s degree in infectious diseases. Assistant professor, Epidemiological Surveillance and Research Department, CIDR, IPK, Havana, Cuba. https://orcid.org/0000-0002-6267-4954
Belkys María Galindo-Santana, physician specializing in family medicine and epidemiology, with a master’s degree in epidemiology and a doctorate in health sciences. Full professor and senior researcher, Epidemiological Surveillance and Research Department, CIDR, IPK, Havana, Cuba. https://orcid.org/0000-0002-8757-4036
Manuel Romero-Placeres, epidemiologist with a doctorate in health sciences. Full professor and senior researcher, IPK, Havana, Cuba. https://orcid.org/0000-0001-9940-1581
Tania María González-Gross, family physician, Provincial Hygiene, Epidemiology and Microbiology Center, Havana, Cuba. https://orcid.org/0000-0002-1914-8289
Isabela Morgado-Vega, family physician, Provincial Hygiene, Epidemiology and Microbiology Center, Havana, Cuba. https://orcid.org/0000-0001-7068-8224
Yadira Olivera-Nodarse, family physician, Provincial Hygiene, Epidemiology and Microbiology Center. Havana, Cuba. https://orcid.org/0000-0002-4224-1967
María Guadalupe Guzmán, physician specializing in microbiology with a master’s degree in virology and a doctorate in health sciences. Full professor and distinguished researcher. CIDR, IPK, Havana, Cuba. https://orcid.org/0000-0003-3927-0844
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.