INTRODUCTION
Design of university degree programs in a given country responds to that society’s specific problems, which also constitute the foundation for student motivation and incentive to develop effective learning strategies.[1]
In his keynote address at the 7th International Congress on Higher Education in Havana, Cuba’s Minister of Higher Education underscored the university’s role in training future professionals “to face and transform the world.” He alluded to the need to build their capacity to solve a broad range of problems in professional practice in different situations produced by various causes, including poverty, illiteracy and environmental degradation.[2]
Key factors determining the strategic position and functioning of higher education in modern society are:
- Relevance, or capacity to meet the needs of the society for which human resources are being educated;
- Internationalization, understood as universalization of teaching and research, mobility of professors and students, international cooperation, communication and networking; and
- Maintaining quality of research and teaching in carrying out its social mission.[3]
To address these, the university must establish itself as a setting for consolidating and strengthening human values in interaction with society, to learn from it and contribute to its improvement and transformation.[4]
Cuba’s medical universities provide a six-year undergraduate curriculum to train doctors for a primary health care model with a comprehensive clinical, epidemiological and social approach involving health promotion, disease prevention, diagnosis, treatment and rehabilitation. All graduates are then required to specialize: for virtually all, a family medicine specialization is first required before graduates can opt for a second specialty. Competencies are well defined to respond to the Cuban health system’s needs, which is a universal public system, with wide geographic coverage at all levels and in which specialists provide care and perform procedures that in other countries may be required of general practitioners. As well, the existence of such a system means that some conditions amenable to primary or secondary prevention are less frequent. Thus, the needs of Cuba’s health system are not the same as those of other societies with different socioeconomic, political and cultural conditions, and different health systems. Hence, the strategic need to train professionals whose broad profile enables them to adapt to other social demands and situations, and in some cases, to provide for additional professional competencies.[5]
In the 1980s, despite decades of economic limitations, Cuba attained a life expectancy at birth of 75.2 years and an infant mortality rate of 11.1 per 1000 live births, the best among developing countries and on par with developed countries, reflecting levels of population health status and health services organization.[6] These advances influenced a government decision to transform Cuba into a leader in global health, necessitating a curriculum for training physicians in which competencies would be linked to ways of working and ability to organize and apply knowledge acquired, integrating it into practice and relating it to the needs of specific contexts.
Consequently, Cuban undergraduate medical training graduates physicians with a broad professional profile, in which students have dealt with patients in practice settings from the beginning of their degree program; because of this integration of theory and practice, they graduate with a different concept of medical practice.[5,7–10]
During many years, resulting from bilateral government agreements, Cuba trained international students in the health professions alongside Cuban students in its medical universities. This activity increased substantially in 1998, with the opening of the Latin American Medical School, which has since graduated thousands of doctors.[5,8]
One such collaborative agreement for medical education has existed since 1997 between Cuba and the Republic of South Africa, under which Cuban physicians serve as professors at Walter Sisulu University’s Faculty of Health Sciences and young South Africans study medicine in Cuba. By agreement between the two countries, South African medical students complete the last internship year at home, finishing their training there to ensure better integration into their future practice settings.
For many years, South African medicine was characterized by elitism, with universities training doctors for the wealthier sectors. This, together with high tuition costs and the apartheid system, blocked access to medical training for low-income students, primarily non-whites. For a long time, only the predecessors of the University of KwaZulu-Natal—University of Durban-Westville and Natal University College—accepted black students. In the 1970s, these institutions were joined by the Medical University of Southern Africa (now University of Limpopo) and in the 1980s by the University of Transkei (now Walter Sisulu University) in Eastern Cape Province.[11]
At the close of the millennium, most of South Africa’s physicians were working in large cities and primarily in the private sector, with a predominantly treatment-oriented focus—this in the context of the country’s largely rural, low-income majority.[11] Thus, the urgent need arose to educate young people from remote areas and impoverished backgrounds who, upon graduation, would return to their communities to provide medical services and to preserve and restore health.
The first South African students who began their studies in Cuban medical universities returned to South Africa in 2003 as interns in the University of Transkei medical faculty. When the second group of 17 interns returned in 2004, some went to the Medical University of Southern Africa. In 2005, 33 students in the third group began their internships in settings that then included medical faculties in Pretoria, Gauteng Province; Durban, KwaZulu–Natal Province; and Free State in the province of the same name. With the fourth group in 2006, internship sites were extended to faculties of medicine in Cape Town and Johannesburg, bringing the number of faculties involved to eight, three of which did not yet have agreements or faculty exchanges with Cuba.
In 2004, the first class of South African students graduated from the Medical University of Villa Clara (UCMVC, the Spanish acronym). By 2009, there were 93 South African physicians with degrees from this university, of 249 who graduated from the three medical universities in central Cuba.
In 2000, the South African Ministry of Health asked the Cuban Ministry of Public Health (MINSAP, the Spanish acronym) to bolster development of certain competencies of South African students, to better prepare them for their future professional practice. Additional competencies requested include various nursing procedures; administration of anesthesia; and some surgical techniques, such as hernia repair, appendectomy, surgery for ectopic pregnancy and cesarean sections. Professional competency was defined as overall preparation to successfully plan, implement and evaluate professional actions in accordance with the characteristics and demands of practice contexts and patients.[12] Development of these competencies takes places through acquisition of a set of skills during the degree program.
In response to this request, and by agreement with the universities involved and MINSAP’s Vice Ministry for Education and Research, a group of experts from the three medical universities of Sancti Spíritus, Cienfuegos and Villa Clara designed a complementary curricular strategy. The strategy, to be implemented independently by each university, was composed of 12 courses intended to develop professional competencies not covered in Cuba’s regular medical curriculum.
This did not involve a redesign of the medical curriculum; neither courses nor timeframe were affected. Rather, complementary courses organized during elective or extracurricular time or during time scheduled for activities in which South African students do not participate, such as civil defense training. Some were scheduled during vacations in Cuba; in years when students spent their vacations in South Africa, these were 15-day units taught by Cuban professors there. A complementary course was defined as an instructional unit on a specific area of knowledge, structured with all components of the teaching-learning process. Courses were sequenced in the second through fifth years of the medical program, avoiding course overload and making sure students had covered prerequisite content in the regular curriculum.
Strategy implementation began during the 2003–2004 academic year and continued uninterrupted through the time of this study (2010). A complete assessment of results can only be done with 2008 and 2009 graduates, since students in earlier cohorts were not exposed to the entire course sequence. However, South African authorities have continued to be dissatisfied with graduates’ attainment of the additional professional competencies, even in these last two cohorts.
This study aimed to determine why the curricular strategy implemented for nine years in UCMVC to complement South African students’ medical training did not yield the results expected, and to identify possible directions for corrective action.
METHODS
Study type A qualitative exploratory study in the form of curriculum evaluation.
Participants The study universe consisted of all 136 South African students who were enrolled in UCMVC’s Faculty of Medicine of during the 2009–2010 academic year and 24 professors who had consistently worked with these students in both core and complementary courses. Within the student universe, 20 fifth-year medical students were selected for survey because they had been exposed to the full curricular strategy at the time of the study. Another 27 students were selected for three focus groups, one for each of the second, third and fourth years (8, 9 and 10 students, respectively); these were students with the best academic records, on the assumption that their higher academic achievement would be reflected in more thoughtful assessments of the program.
A purposeful sample of professors was composed of eight professors who had taught a complementary course at least five times, on the assumption that their more extensive experience with the South African students would give them greater insight.
Interviews were conducted with the seven senior academic administrators who had had most experience with these students (more than five years)—dean, vice dean, three department heads and two provincial hospital deputy directors for teaching—to elicit their opinions about quality of course design and implementation, the roles of students and professors in the courses, and support and oversight from university administration.
Eight key informants were also included in the study: three Cuban specialists in family medicine who had served in South Africa and were thus familiar with professional demands on doctors there, and five other specialists—two obstetrician-gynecologists, a pediatrician, a general surgeon and an anesthesiologist—who been in South Africa as clinical instructors and were able to observe returning South African graduates’ practical and intellectual professional skills, as well as any gaps in competency. These key informants acted as an expert nominal group that, once apprised of research findings, would be asked advice on the main directions for corrective action (taking into account priorities provided by senior academic management at UCMVC).
Design The first stage involved review of documents: minutes of workshops with South African academic authorities, to verify skills requested as needed for general practitioners in South Africa; program records to verify compliance with the curricular strategy; complementary course syllabi, to assess completeness and quality of course components; and academic records of 17 students who began the program in the 2003–2004 and 2004–2005 academic years.
During the second stage, fifth-year students were surveyed, results used as the basis for focus groups with second-, third- and fourth-year students, by academic year. Focus group results were used to draft guides for in-depth interviews of professors, senior university administrators and key informants. Information obtained from different sources and methods was triangulated; data were distilled, categorized, coded and subsequently presented to the nominal group described above, with a view to determining major steps proposed to improving the situation.
Ethical aspects The UCMVC ethics committee approved the study and all participants gave written informed consent to participate.
Variables The following were considered:
Course assessment Evaluators—the authors, advised by content experts—determined the presence and quality of courses’ structural components: evidence base, objectives; thematic coverage, content depth, teaching strategy, evaluation and references, rating each as positive if it was present and considered of adequate quality, negative if the component was missing or its quality inadequate. Overall course ratings were described as percentages of compliance with these components and qualitatively: positive if they met the essential requirements of ≥4 components and negative if <4.
Satisfaction with courses Students were asked about satisfaction with three aspects of courses: content, organization and future usefulness, using a five-point Likert-like scale, with responses of 4 and 5 considered “satisfied.” Professors were asked the same questions face-to-face for the courses they taught, but responses were simply yes or no. Overall satisfaction with courses was defined thus: satisfied, if more than 75% gave “satisfied” responses, dissatisfied if less than 50% “satisfied responses,” and “moderately satisfied” if between the two.
Instruments Nine data collection instruments (available on request from corresponding author) were developed by the authors and validated in a pilot study in May 2010:
- Document review guide Eight structured points and one open-ended point, with the following search category: explicit or implicit mention of professional competencies that need to be developed in South African medical students.
- Complementary course syllabus review guide Eight points, searching for explicit or implicit congruence between professional competencies requested by South African authorities and stated course objectives. Structural validity of syllabi against specified criteria.
- Student record review guide Structured, with 12 items, searching for evidence that students had taken complementary courses and had been evaluated, by academic year.
- Student survey Semi-structured, exploring dissatisfaction with regard to course content, implementation and future usefulness of courses, along with suggestions for improvement.
- Focus group To identify main perceptions, feelings and attitudes of students as clients or users of complementary courses, along with their proposals for improvements.
- Guide to in-depth interviews with professors Eight points, with the objective of obtaining a critique of courses regarding their subject matter, efficiency in delivery and/or future utility, along with suggestions.
- Key informant interview guide Six points, to determine congruence between competencies requested by South African authorities and professional practice demands in South Africa, and to find evidence of any related deficiencies among students trained at Villa Clara.
- University academic administrator interview guide Seven open-ended points, to detect explicit or implicit acknowledgment of problems with courses and of insufficient action by academic administration.
- Nominal group To obtain expert opinion about most important competency gaps, implementation problems and directions for corrective action, a moderator provided the nominal group with a summary of results found using the other instruments.
Data collection Instruments were administered in June 2010, when students from each year had already completed most of their courses.
Data analysis Steps in organization, triangulation and analysis of data included:
document review transcription, distillation and thematic organization; review of student survey and focus group results and in-depth interviews, to identify and classify elements for which over half the participants’ opinions concurred (data categorization); and simple statistical procedures using percentages for display in tabular format.
RESULTS
Review of the proceedings of the first joint academic workshop of medical faculties of Cuba and South Africa and minutes of international workshops of South African students revealed dissatisfaction by the Walter Sisulu, KwaZulu–Natal and Limpopo universities, emphasizing that students had developed strong human values and motivation for primary health care, but had weaknesses in some professional and communications skills.
Program document review revealed that some of the strategy’s planned actions were not carried out (courses in pediatrics and in obstetrics and gynecology) and that some activities designed to be delivered in South Africa during vacations were never implemented (pharmacoepidemiology refresher, pediatrics and internal medicine courses). Placements in pediatrics and obstetrics and gynecology planned for the final semester of the fifth year did not occur in either cohort.
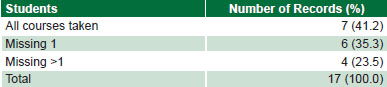
Review of student academic records found that fewer than half of students had completed all the complementary courses and one-quarter were missing more than one course (Table 1).
Table 1: Second-year students in complementary courses, 2003–2004 and 2004–2005 academic years

Source: Academic records
Table 2: Assessment of complementary courses for South African medical students, Medical University of Villa Clara

Table 2 contains results of the assessment of complementary course syllabi. The distribution of positives and negatives shows that there have been difficulties, since in several courses components were lacking or seriously deficient, such as the evidence base, objectives, and teaching and evaluation strategies. Four courses were assessed as complying with <50% of criteria.
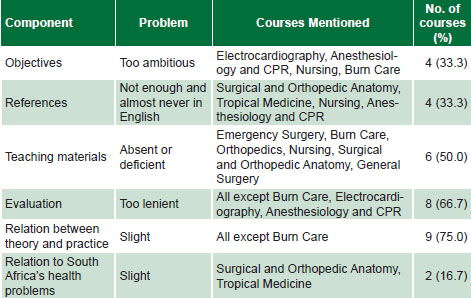
Table 3 displays fifth-year student appraisals of complementary courses from the course survey and focus groups. They perceived a weak link between theory and practice in all courses except Burn Care; and lack of evaluation rigor in most courses, with the exceptions of Electrocardiography, Burn Care, and Anesthesiology and CPR. They also mentioned that teaching materials were lacking or of poor quality in half the courses. Predominant opinions are shown for the different aspects explored in the survey. Focus groups were of the general opinion that on-call shifts were unappealing, as was any type of spontaneous participation in services— such as the emergency room or certain wards—because “they make us take patient medical histories.”
In-depth interviews with professors yielded the following problem ranking:
- Own lack of knowledge of students’ future practice context
- Students’ lack of motivation
- Students’ lack of initiative for self-directed learning
- Students’ problems understanding Spanish
- Course ineffectiveness, or failure to meet its objectives
The majority of professors said that students “are not interested in the courses,” leading them to skip class, participate little and even on occasion not do the course work. Half the professors recognized the courses’ usefulness for students’ future professional practice, but said that students were not performing as well as they could, attributing this to several factors. These were lack of appropriate bibliography, lack of student motivation—which in turn did not impel professors to strive for quality or to be more demanding in evaluations—and lack of appropriate teaching materials. In general, professors perceived that students did not take initiative to participate in practical activities or exercise self-directed learning. Comments included that students “do not take initiative in their learning process, which might be determined by their problems communicating with patients.” “They do not understand Spanish speakers very well and prefer to …associate with [other South African] classmates [rather than Spanish-speaking ones],” which, in the professors’ opinion, contributed to making the language communication problem worse.
Table 3: Problems with complementary courses (n=12) identified by fifth-year students

Table 4: Problems with complementary courses identified by professors (n=8)

As can be seen in Tables 3 and 4, problems identified by students and professors lay in three main categories, related to teachers, to students and to administration, although some can be attributed to logistics (lack of bibliography, lack of teaching aids to illustrate complex phenomena, and scarcity of practice opportunities).
Professors expressed greater satisfaction with complementary courses than did students (75% vs. 66.7%). Both were most satisfied with course content, but to different degrees (professors 100%, students 75%). For professors, future usefulness was the next ranked in satisfaction after content, while for students it was the source of least satisfaction (professors 75%, students 60%). The only aspect on which professors were less satisfied than students was course organization (professors 50%, students 65%).
Academic administrators demonstrated full knowledge of the complementary curricular strategy, which they acknowledged they had not sufficiently supervised. They believed the proposed actions to be of high quality, although they understood that these could be improved and others added. They acknowledged that strategy implementation had been hampered because of the low priority it was given at different levels. They rated the various elements as acceptable but not optimal, in relation to faculty and students as well as material conditions.
Key informant interviews corroborated that complementary courses were an appropriate strategy to fill the competency gap for South African trainees.
The nominal group yielded factors that affect problem persistence and some possible directions for future action:
Problems with professors’ pedagogical training, hampering their ability to provide more appropriate instructional treatment of subject matter, contributing to an imbalance between theory and practice in course content and in evaluations that miss their mark. Suggested action: training in adult education methods for professors who develop and deliver complementary courses.
Poor development of students’ learning strategies, which limits their understanding of the importance of communication in the learning process and keeps them from seeing how self-directed learning helps them acquire professional skills; a reflection of this is their lack of appreciation for the critically important clinical skill of taking a medical history. Suggested action: explicit attention to students’ metacognitive and communications skills.
Ineffective, insufficient management at different levels, related to availability of reference materials, planning of complementary courses in South Africa, vertical and horizontal coordination of planned courses, and alternative solutions to lack of teaching materials. Suggested actions: development of resources for real or simulated teaching–learning activities; and closer connections between university administrations in both countries for more direct dialogue and deeper understanding of educational issues.
DISCUSSION
Two main themes were identified as threats to full compliance with the strategy as designed: scarcity of time and resources for fully implementing planned activities, and insufficient managerial oversight.
With regard to lack of sufficient time for the strategy’s planned activities, we consider there might have been a lack of academic management strategies to optimally plan use of available time, perhaps with a larger dose of independent work and individual responsibility from students, since there are blocks of time that are still not used optimally during the medical program.
Confirmation that some planned activities were not carried out makes gaps in attainment of expected professional skills understandable. The strategy is ambitious, especially in the Cuban health system, where some requested skills are infrequently required of undergraduate students, given the pedagogical model in Cuba, the requirement for specialization by all physicians and the structure of the health system itself. For example, inclusion of strong preventive components in the system’s Maternal and Child Health Program means that students will have scant opportunity to develop skills in diagnosis and management of dystocia. Similarly, students would rarely have occasion to practice nursing procedures, which in Cuba are the purview of university-level nursing personnel. Also, all requested content is in addition to a core curriculum already packed with professional training objectives. Any amount of time that is not used optimally to the benefit of learning is counterproductive.
The university has a responsibility to find ways to develop skills in professionals who must practice under conditions that are different from those they experience during their training. Accordingly, it must engender not only knowledge and skills, but also, and fundamentally, personal motivations, values, skills and resources for practicing with efficiency, autonomy, ethics and commitment to society, along with creativity in the quest for knowledge.[9]
Evaluation of complementary courses confirmed that the requested professional skills served as a guide and starting point for their design. Accordingly, their objectives should have been built on the same foundation, driving student assessment. Although this was shown to be the norm, four courses had objectives that went beyond training for the requested skills. In the logic of teaching and learning, this must have resulted in evaluations that were not very relevant. Along these lines, we are persuaded that a thorough review of complementary courses would be useful, measuring stated objectives against demands for competencies to be developed. If objectives exceed the social needs for which they have been developed, they can upset the balance between programs goals and levels attained.[6]
In some courses, lack of pedagogical analysis of course content to match it to the most effective teaching methods kept professors from planning activities for students to carry out on their own. It is quite appropriate for professors in the different courses to assign students—as individuals or in groups—to take a complete medical history or any of its components, such as review of symptoms. The utility of history taking could also be demonstrated by using simulated patients.
Poor pedagogical training might be the cause of weaknesses in both courses’ pedagogical strategy and student dissatisfaction. A professor with solid teaching skills can design alternative learning activities when faced with practical obstacles to the ones planned; for example, working through a case study of a problem in professional practice or interactive simulations, as long as the teacher knows how to mediate and facilitate students’ internalization of content, both essential components of learning theory.[13]
Results regarding students’ and professors’ levels of satisfaction seem to reflect either greater expectations on the part of students vis-à-vis their training or lack of comprehensive understanding of the complementary course program and its purposes. Professors were more positive about the courses, although they recognized difficulties; interestingly, they were more critical of course organization than were students.
With regard to students’ opinion that some courses do not address their country’s most frequent health problems, we believe that this may be the underlying cause of their discouragement. A contributing factor might be teachers’ lack of familiarity with the setting in which these future professionals will eventually practice.
The assessment of senior academic administrators is valuable, since they showed understanding of the difficulties faced, in tune with opinions collected from other parties involved. Thus, they are well positioned to take on the challenge of improving the strategy.
The nominal group considered that little had been done to develop students’ learning strategies. For example, taking a medical history fosters skills in understanding signs and symptoms of different conditions as described by patients, communication with patient and family members, and logical reasoning in differential diagnosis and application of clinical skills. The authors believe that this is a consequence of problems in the professors’ pedagogical training, which have also been acknowledged.
The key informants are an asset whose inclusion in this process could be helpful to professors in charge of developing complementary courses.
The South African medical students who participated in this study met degree program objectives in each academic year and in addition received training in complementary professional skills. Such competencies are not developed in the short term, so self-directed learning and metacognitive strategies are imperative. It is important for professors to convey to students that theoretical knowledge acquired from courses serves as the basis for building skills, but that these skills develop through increasingly complex actions, which, when shared and practiced in complementary courses, will foster appropriate professional practice at the end of their training.[14]
Limitations of this study include lack of analogous studies for comparison and our inability to study sixth-year students who had already returned to their home country as interns. However, key informants were able to provide external information about competencies of sixth-year students in previous cohorts. Another limitation was the opinion-based nature of the survey, giving results that are by definition subjective.
CONCLUSIONS
It is outside our purview to suggest improvements to the core medical curriculum; closing the competency gaps for South African graduates of Cuban medical schools will thus require improving the complementary curricular strategy. This will take improved academic management to ensure the most important actions:
- Pedagogical education for teachers in charge of the courses and training in other specific aspects.
- Explicit attention to students’ metacognitive resources and their communications skills.
- Development of logistical resources to facilitate real or simulated teaching-learning activities.
- Strengthening the bonds between university managers in both countries, to achieve more direct dialogue and understanding of educational issues.