INTRODUCTION
The Scientific and Technological Innovation System (SCIT) is the organizational cornerstone for participatory implementation of Cuba’s science and technology policy at the ministerial and institutional levels. It is aligned with Cuba’s economic and social development strategy and with national priorities in science and technology, which are integral to the strategy. For over five decades, SCIT’s role has been defined in various policies and guidelines, aimed at enhancing science’s contribution to development.[1,2] It is regulated by the Ministry of Science, Technology and the Environment (CITMA).[3]
Although each ministry defines its SCIT structure based on its particular needs, in each case, the SCIT covers a broad spectrum, ranging from assimilation, generation and compilation of knowledge, to production and sale of goods and services. It includes basic and applied research, as well as studies in technological, social and management development.[4] SCIT has been fine-tuned in recent decades, with a view to contributing to greater well-being of the Cuban population, a stronger social welfare system and improvements in main social indicators, especially in health (linking science to medical education and practice as one of the principles of Cuban public health).[3–5]
Hospitals require advances in science and technology to fulfill their service, academic and administrative missions, their obligation to conduct clinical research is thus beyond question.[5,6] A SCIT is useful for designing and implementing new diagnostic and therapeutic technologies, programs and services, and for introducing new drugs and medical equipment. Nevertheless, it is difficult to assess the impact of SCIT activity due to lack of consensus on useful indicators, not to mention challenges inherent to measuring them.[7–9]
A hospital’s human scientific potential consists of all human resources capable of conducting research, such as physicians, nurses, health technologists and engineers. Understanding the link between a hospital SCIT and indicators of scientific activity enables evaluation of SCIT results, including development of the scientific human resources necessary for taking on new tasks, tangible scientific outputs, and the impact of the two on national recognition.
Evaluation of scientific activity has been conceived in other scenarios and has its roots in the 1945 Vannevar Busch report, which established its conceptual underpinnings. Today, it is one of the pillars of government science and technology policy for a range of institutions, in Cuba and elsewhere.[8]
Since 1998, scientific activity at the Dr Gustavo Aldereguía Lima University Hospital (HGAL) in Cienfuegos Province is integrated in a SCIT, whose mission is to foster comprehensive implementation of technological research and innovation in response to priority health problems and research lines defined and approved for HGAL—aligned with both the hospital’s primary mission and the province’s science and technology strategy.[1,2] SCIT has four strategic areas: scientific potential, or development of human resources for science; scientific output and technological innovation; management of scientific activity; and intra- and extramural scientific integration (coordination of scientific activities among HGAL departments and services and between HGAL and other provincial and national institutions).
The starting point in HGAL’s SCIT structure is a database of scientific problems that fuel HGAL’s research lines. Reviewed annually, these are derived from strategic problems and policies defined by the Ministry of Public Health (MINSAP) and by HGAL’s own management. HGAL’s regulatory and oversight subsystem consists of the hospital management committee and two advisory bodies: the Scientific Council and research Ethics Committee. A scientific and technological section within HGAL’s teaching and research department directs SCIT implementation. A series of national indicators[7,10,11] is used to evaluate outcomes.
SCIT is mandated to:
- plan scientific activities;
- strengthen the management and research ethics committees;/li>
- train human resources to conduct research;
- generate and implement projects;
- publish and disseminate research results; and
- ensure intra- and extramural institutional integration.
All six activities are part of HGAL’s management plan, evaluated based on periodic reports from HGAL departments and services, especially those involving human resource capacity-building and scientific output.
HGAL is one of the leading research institutions of its kind in Cuba,[12] but there are no studies showing the relationship between SCIT and fulfillment of HGAL’s main scientific objectives or the system’s impact on scientific output. Thus, the purpose of this study is to describe SCIT’s contributions to the main indicators of scientific activity.
METHODS
This was key informant study and document review concerning HGAL’s principal scientific outputs (clinical studies, design or introduction of technology, and scientific capacity development) in the 2000–2014 period. The study’s two main tasks were to define SCIT’s key outcomes and indicators of scientific output, and to have key informants assess whether outputs and indicators were related to SCIT.
Indicator selection A series of indicators was proposed, based on nationally accepted indicators of scientific activity,[10] indicators defined for CITMA’s Scientific and Technological Innovation Entities;[7] and those considered in MINSAP’s strategic projections for 2010–2015.[12,13]
Indicators of scientific activity (scientific and technological output during the period and SCIT’s impact) were divided into three groups:
- scientific potential (researcher training), including percentages of scientific staff with PhDs, scientific staff accredited as researchers, professionals holding MS degrees, medical specialists certified at grade II (highest level of specialization), plus improvement in the human resource performance evaluation program;
- HGAL scientific output, including annual average numbers of publications, studies completed and projects in execution, and total number of clinical trials conducted; and
- recognition of HGAL’s scientific activity, based on
- provincial recognition (e.g., awards in provincial competitions),
- national recognition (e.g., Cuban Academy of Sciences certification as an institution eligible to make nominations for Academy membership; CITMA certification as a Science and Technological Innovation Entity; recognition by the Science and Technology Forum; awards and honorable mentions in the national Annual Health Award; awards from CITMA for technological innovation; awards from the Cuban Academy of Sciences), and
- international recognition (e.g., certification as a PAHO/WHO Collaborating Center).
A questionnaire was designed based on this preliminary selection (Appendix 1; available online at http://www.medicc.org/mediccreview/navarro.html), administered to 22 key informants (group A) to obtain their assessment of SCIT impact on these indicators. Respondents were asked to apply a Likert-type scale to each candidate indicator to assess SCIT’s potential impact as very high, high, moderate, low or none. Indicators were accepted for inclusion if they were assessed as very high or high by 70% of respondents. Indicators were not assigned weights.
The key informants, selected from among members of HGAL’s Scientific Council, were highly regarded researchers who had been associated with HGAL for an average of 26 years. All had advanced degrees in the sciences (32% PhD and 68% MS); 77% were accredited academic researchers; 91% were full or associate professors; and all physicians were grade II specialists. All informants had demonstrated experience in evaluating scientific research as members of various review panels; none declared conflict of interest.
Document review Data for each indicator were taken from the HGAL Statistics Department’s annual report and from the databases of HGAL’s information management and science and technology departments.
The relationship between outputs, their indicators and HGAL scientific activity was determined through quantitative and qualitative analysis of scientific output linked with each result and SCIT activities (activities within each strategic area that contributed to the outputs). We conducted a document review of SCIT objectives, strategic areas and activities, as well as research (publications, doctoral dissertations, master’s and specialty theses, and relevant scientific results presented at the Science and Technology Forum) that contributed to these indicators and that were available in the databases of the Medical University of Cienfuegos information management center and the Cienfuegos Provincial Health Department. The following databases were also searched: PubMed, SciELO and CUMED (for books by Cuban authors and Cuban science journals). The search included all records where names of HGAL personnel appeared in author, title or abstract fields for any of the years studied. Not was only the number of studies carried out considered important, but also introduction of procedures, drugs, technologies or new organizational approaches.
Confirmation Semistructured interviews were then conducted with a second set of 35 key informants (group B), the principal investigators of the research projects linked with the aforementioned scientific results to confirm their relationship to SCIT. Some 22.9% of group B key informants had scientific doctorates; 97.1% had teaching appointments (77.1% full or associate professorships); and all had worked at HGAL for more than 15 years. It should be noted that there was participatory observation by the authors, who have directed HGAL scientific activity for more than 15 years. The study was approved by HGAL’s director and all procedures (interviews and surveys) complied with ethical requirements regarding patient confidentiality.
RESULTS
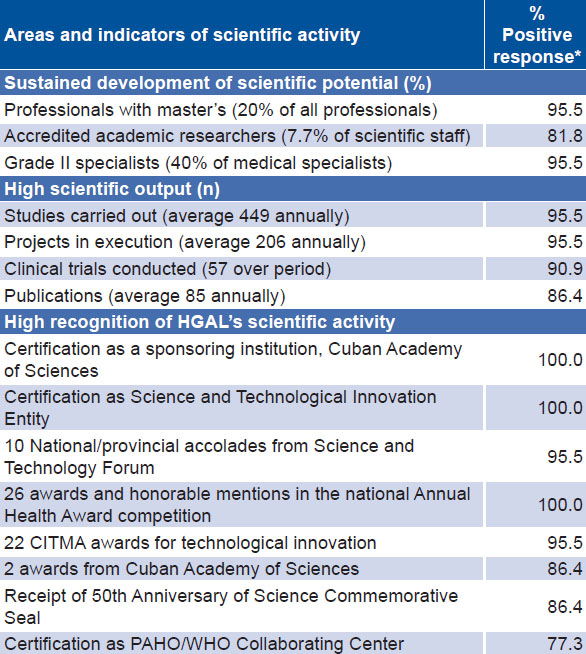
Table 1 displays HGAL’s most important scientific results and group A key informants’ assessments of SCIT’s role in these.
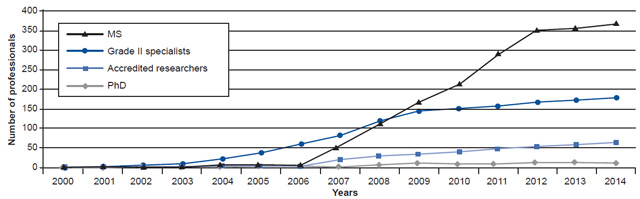
Figure 1 shows sustained development of scientific potential over the study period. In 2014, HGAL had 2012 professionals, 41.5% (834) considered part of its scientific human resources. Key informants did not consider training of PhDs (2.2% of scientific potential) or introduction of a professional performance evaluation program to be related to SCIT. Elements they did consider important were the broadening of criteria for professors’ accreditation (2004); delivery of an extensive master’s degree program (three iterations in 2004–2007); and inclusion in SCIT objectives of a call for applications for researcher accreditation (as of 2007), which promoted and in fact required reorganization of scientific activity.
Table 1: Key informant assessments of areas and indicators of scientific activity, HGAL, 2000–2014

*group A key informant responses indicating high or very high SCIT impact on indicator
CITMA: Ministry of Science, Technology and Environment
HGAL: Dr. Gustavo Aldereguía Lima General Hospital
Figure 1: Number of scientific personnel and distribution by category. HGAL, 2000–2014
CITMA: Ministry of Science, Technology and Environment HGAL: Dr. Gustavo Aldereguía Lima General Hospital
Group A key informants considered that results related to development of scientific potential were influenced by the following SCIT activities: promotion of grade II specialty training, researcher accreditation and awarding of master’s degrees and PhDs in the sciences, development of an extensive continuing education program (for researchers and their mentors), public recognition of professionals with good scientific results, promotion of research and other scientific activities, and the requirement that professional and technical staff participate in national events sponsored by scientific societies.
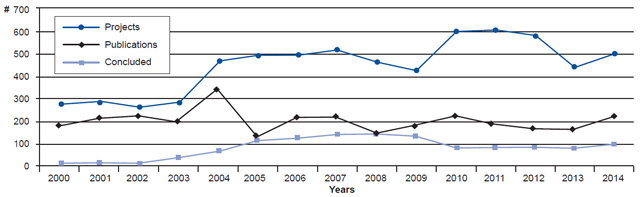
Figure 2 shows an upward trend for the period in studies concluded and presented at scientific events and annual number of publications, along with a slight reduction in projects after a peak in 2004. Over the 15 years, 6730 studies were conducted (averaging 449 annually), 1275 of which were published (averaging 85 annually), with an average of 206 projects in progress each year (a project can encompass more than one study). In addition to creating new knowledge, the results contributed new techniques, mainly organizational, including a system of color coding to prioritize patients and procedures;[14] interventions to improve the quality of patient care (including development of a quality management system);[14–19] new clinical practice guidelines;[14,20] reorganization of surgical activity;[14] and patient safety programs.[21]
Activities that fostered scientific output and technological innovation were periodic redefinition of HGAL’s lines of research; promotion, monitoring and facilitation of technical assistance for science and technology projects; monitoring of clinical trials; commitment by chiefs of services and department heads to execution of at least one institutional research project per year; development of clinical practice guidelines as a system for service delivery; the requirement that senior staff produce at least one publication annually; and requests to the deputy directors for targeted research based on the main problems within each of their services and departments.
Figure 2: Annual number of publications, studies concluded and projects under way, HGAL, 2000–2014
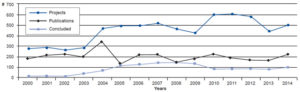
Concluded: studies completed and presented at a scientific event HGAL: Dr. Gustavo Aldereguía Lima General Hospital
The heightened visibility of scientific activity at HGAL during the study period resulted from multiple national awards conferred by MINSAP and other ministries on its researchers and scientific output. Notable among these were 26 awards and honorable mentions in the national Annual Health Award competition, 22 CITMA awards for technological innovation and scientific research, and 2 national and 8 provincial accolades from the Science and Technology Forum. In 2010, HGAL, together with 50 other institutions around the country, was awarded the 50th Anniversary of Science Commemorative Seal.
Activities to improve management of scientific activity were designed to support the work of the management and research ethics committees (including the work of each service’s science committee) as advisory and oversight bodies; establish a department for managing scientific activity, in close collaboration with the management and research ethics committees; promote key scientific events with multidisciplinary participation; facilitate scientific information management at HGAL; integrate SCIT’s principal tasks into HGAL’s management plan and services; facilitate documentation processes and creation of review boards; and ensure logistics for implementation of projects with greater institutional impact. This also included intra- and extramural integration (with other organizations comprising the external elements of the system).
DISCUSSION
Conducting research aligned with MINSAP objectives is one of the three main functions of a public university hospital in Cuba. Considered essential to HGAL’s work, such research has the potential to generate knowledge to help solve problems, foster an environment in which that knowledge will be assimilated, and support decisions aimed at achieving institutional growth and excellence.[5,6,22,23]
HGAL scientific output is high. SCIT development and consolidation has led to sustainability of its historical results in all areas. In the authors’ view, a critical element for developing scientific potential is the intent of HGAL’s management strategy with respect to SCIT and its implementation at all levels. This is in keeping with Lifshitz, who stresses that it is counterproductive to rely solely on individual ability to develop education and conduct research; what is needed is an explicit institutional policy. He also notes that strategic planning uses education and research as tools and that hospitals have responsibilities that extend beyond their walls.[23]
A SCIT that is included in a management plan (as is the case for HGAL’s since its establishment in 1998)[14] turns scientific problems into work areas, promotes research, participates in researcher training, monitors and evaluates scientific activity and facilitates dissemination of new knowledge. It should be noted that as part of SCIT monitoring, most indicators with positive outcomes in this study are periodically checked and year-to-year performance compared.
Research findings represent knowledge generated or modified and serve as inputs for changing a situation, making decisions or solving problems related to the good operation of the health system. Science and technology are therefore essential for development strategies and more effective responses to social demands.[5,24,25]
It should be added that one of the SCIT processes described, project-based planning, is the norm in Cuba’s approach to planning for scientific and technological innovation.[3,7] One of the strengths of a hospital SCIT is a graduation requirement that all residents and master’s degree candidates present a research study as part of their final exam.[26] In the case of residents, this primarily fulfills an academic requirement; but it also serves as a vehicle for promoting research in the various services, since mentors (HGAL specialists) participate actively in study planning and execution. Moreover, accreditation as a grade II specialist or academic researcher requires candidates to have carried out, presented and published research in their specialty.[27]
Features of HGAL’s SCIT have been: the afore mentioned strategic and participatory nature; the merging of the Science and Technology Forum with the annual science meeting as the most important event for presentation of research findings (48.9% of professional and technical staff participate annually, presenting at least one scientific paper related to HGAL’s research lines); review and monitoring of all research projects by the Scientific Council; review of master’s and specialty completion theses prior to their defense or final examination by the Scientific Council; the work of science committees in each of the hospital divisions headed by deputy directors (internal medicine, surgery, maternal and child health, emergency and administration); the system’s integration into hospital management strategies and horizontally across services and departments; and the melding of CITMA and MINSAP regulations.[12] Similarly, to meet SCIT objectives, the Scientific Council and the Scientific and Technological Innovation Department were merged (headed by the secretary of the Scientific Council).
Of course, SCIT is not a static system, which creates attribution challenges. Until 2004, the core of its structure was the Scientific Council,[12] which had executive functions. After that date, SCIT’s structure changed when HGAL and its SCIT were certified by CITMA as science and technological innovation entities.[28] Similarly, some indicators of scientific potential changed in the last two years studied; 2013 opened with the best indicators in the period, but by December 2014, the number of residents increased, reaching 300, and 508 new professionals were added to the staff for different reasons; the increased denominator lowered the percentages of some indicators.
The Hospital Clinic of Barcelona, the paradigm for biomedical research in Spain, attributes its success to a strategy characterized by organizational reform of services and centers, creation of a research foundation, sabbatical years for research, integration of clinical and basic research and creation of one-year research fellowships for professionals upon completion of their residency (Recently graduated specialists do only research during that year and participate in care only if it is clearly related to the research project).[6] HGAL adopted only the first of these features, although not in the same work areas as the Spanish hospital.
Some experiences in hospitals with a good track record in research suggest the need to design services with a mix of professionals with responsibilities for care, research and teaching,[22] or hiring of trained researchers.[23] The guiding principle in Cuba is to have professionals able to effectively engage in all these activities, with their training needs identified and addressed by SCIT.
Given HGAL’s patient-care mission, it is hard to conduct “full-cycle” studies that bring a product through all the phases of development, research, registration and commercialization; and even harder to develop new biotechnology products. Hospitals necessarily focus their scientific work on problems such as clinical and quality management, researcher training, introduction and development of organizational technologies, etc. Their typical projects relate to health systems and services research and health technology assessment.[2]
Many research findings at HGAL involve patient care. They have led to changes in clinical practice,[14,16,17,19] introduced organizational technologies,[12,14,16,20,21] and may be related to the reduction of case fatality in tracer diseases associated with hospital care.[14,15,18,19] One example of this is myocardial infarction, for which the hospital case fatality rate plummeted by 30% during the period;[15] during this time, 26 related studies were conducted, yielding 17 new technologies for management of the condition, along with one doctoral dissertation, 6 master’s theses and 36 publications. Case fatality from cerebrovascular disease fell by 13%;[18] 20 studies were conducted to address this problem, including one doctoral dissertation and 6 master’s theses, with 22 publications. Case fatality from community-acquired pneumonia fell by 16.1%, chiefly in patients who were less seriously ill at the time of admission;[19] 13 studies were conducted on this topic, including 5 theses, with 9 publications.
Activities in science and technology are measured indirectly, using indicators, as opposed to directly. We have taken into account documents reporting on international attempts to set standards for assessing results in science and technology.[7] The authors agree with other researchers that many science outcomes or benefits are hard to quantify economically and socially because they are intangible, multidimensional and slow to materialize;[7,9] for example, measuring an increase in knowledge poses a challenge, since knowledge is an intangible and cumulative concept.
SCIT’s scientific results, defined by the effect of scientific research on science itself or on knowledge,[8] are seen in the upgrading of human resources (almost half of HGAL’s professional staff are trained and certified to conduct research) and their scientific output. Increasing the number of professional staff with scientific accreditation as researchers or grade II specialists makes for professionals better able to solve the most important health problems more quickly. Álvarez underscores the centrality of human beings in any organization, saying that health professionals must be able to innovate and revolutionize processes related to their work.[29] One of the strengths of HGAL’s SCIT is that it covers all personnel categories.
A study in 15 Australian hospitals found that researchers in these institutions were predominantly male physicians aged 45–54 years who were active researchers with senior academic standing.[30] Although we did not examine staff makeup by age and sex, administrative records reveal that it differs from that of the Australian hospitals studied. Hiscock identified lack of the following as barriers to research: time and space for research; adequate financing; education, technical assistance and training for health personnel; researcher versatility; and an adequate institutional system.[30] These barriers must be addressed if the goal is to guarantee quality research.[22,24,30,31]
Few studies offer a comprehensive look at scientific output of hospitals in Latin America and the Caribbean. One commonly used indicator of scientific output is number of publications.[32] At the over 100-year-old Mexico General Hospital (with 6502 workers and 120 researchers) Macías found an average of 117 publications annually in a 14-year period.[25] In contrast, several hospitals in Spain averaged over 160 publications annually;[32] however, the number of professional staff and beds in these institutions is triple that of HGAL.
A bibliometric characterization of HGAL’s scientific output in 2004–2009 (591 publications by 259 authors) showed that 48.6% were original research, 10.3% case studies and 9.3% new clinical practice guidelines; the main journals were Medisur (39.6%) and British Medical Journal (11%).[33] Interviewees considered these results strongly related to activities designed by HGAL to increase number of publications.
Presentation at a national event or publication of results from a research project that has generated new knowledge represents in itself an impact on science. At HGAL, an average of 40 papers was presented annually at the Science and Technology Forum, and an average of 80 papers published, both contributing to a high number of national awards. Within HGAL’s strategic planning, SCIT systematically measures (two or three times annually) indicators such as: presentation of papers at the Science and Technology Forum and other national events; articles written and/or published by specialists, staff with master’s degrees and researchers; and number of studies conducted; as well as increases in the number of grade II specialists, senior teaching staff, researchers and staff with master’s degrees.
Another SCIT indicator is linked to conduct of clinical trials. As a result of multicenter clinical trials, HGAL research has helped validate use of 17 new biopreparations (mainly interferon-α, streptokinase, erythropoietin and epidermal growth factor) currently used in treating cancer and the main chronic non-communicable diseases.[15,34,35]
Finally, external accreditation of HGAL and its SCIT has been conducted four times to evaluate the quality of HGAL’s scientific activity. In 2004, HGAL obtained certification as a sponsoring institution for the Cuban Academy of Sciences; in 2006, it was certified by CITMA as a Science and Technological Innovation Entity; and in 2004 and 2012, it obtained MINSAP’s highest level (III) of hospital accreditation for its science and technology capacity. All of this suggests that SCIT has had a positive impact on HGAL’s scientific prestige.
The authors consider that HGAL demonstrates research capacity,[36] since it is able to conduct and publish scientifically relevant research, has aligned its research priorities with the main health and management problems defined in its strategy, has had the financial independence to invest in priority research, and has shown an aptitude for comprehensive management of research undertaken on its premises, including studies conducted by HGAL as part of the provincial health network.
One study limitation is the lack of baseline data that could enable a pre- and post-SCIT analysis to substantiate key informants’ opinions, but this is offset by the clear upward trends observed between 2000 and 2014. In addition, SCIT is an open system and so outcomes observed may have been influenced by other hospital work with differing objectives during the period, such as human resources management (focused on technical and teaching deve-lopment) and quality management (aimed at improving medical care).
This study shows the potential for scientific and technical deve-lopment in a public hospital. In such institutions, a SCIT that is part of hospital management and performance plans at all organizational levels could be key to ensuring more and better researchers, higher scientific output and recognition of scientific activity as such.
CONCLUSIONS
Sustained improvements in institutional science and technology development and achievement of good scientific results during the period following implementation of HGAL’s SCIT, suggest that such a system can contribute to a hospital’s scientific capacity and productivity.