INTRODUCTION
Lung cancer is the leading cause of cancer death worldwide.[1,2] In Cuba malignant tumors caused 22,532 deaths in 2012, overtaking heart disease as the leading cause of death. Tumors in trachea, bronchi and lung (ICD-10 No. C33–C34) occupied first place among causes of cancer deaths, with a rate of 45.3 per 100,000 population.[3]
If health is to be improved and disease prevented, health should be recognized as a social product and process, based on organized and coordinated contributions by all social stakeholders concerning living conditions.[4] Health promotion has been defined as an organized community effort to create policies for improving individual and population health conditions, and for developing a social system that ensures everyone a standard of living adequate for maintaining and improving health.[5]
Prevention has been defined as a set of activities aimed at reducing problems caused by diseases or disorders in individuals through early intervention at each stage of a health problem, including primary prevention to avoid occurrence of the problem in the first place.[6] Prevention depends on awareness of risk factors and their health implications if changes are to be brought about in attitudes, behavior, standards and family conditions. Knowledge by itself will not change a person’s behavior, but it can determine which healthy actions are possible.
Health education promotes participation of various groups in the learning process by facilitating sharing of information and experiences, raising awareness and developing skills that help to change values, practices and lifestyles.[7] Sanabria suggests that educational programs help to improve or preserve the population’s health. They are designed to promote awareness, create positive attitudes to transform behavior, develop self-care skills, foster change from unhealthy lifestyles, develop negotiation skills, or create public awareness to demand the right to health, among many goals. The proposed educational program covers a broad spectrum, from strengthening or modifying (as applicable) individual lifestyles to empowering people to defend their spaces and attain health and better quality of life.[7] The advantages of this type of intervention lie in the fact that the group is understood to have a mediatory role and, at the same time, to be well placed for building and developing subjectivity, which constitutes, undoubtedly, an instrument for change.[8]
Research and practical educational interventions have been grounded in theories and models developed in diverse disciplines, areas of knowledge and professional fields.[9,10] These educational programs presuppose a set of actions focused on raising target populations’ awareness of health-promoting behaviors.[9]
Women play an important role in health maintenance and improvement, since they are essential figures for instilling healthy behaviors, habits and lifestyles early in life that will become part of their families’ knowledge and practice for health maintenance. [7] Moreover, the realms of women’s action and social interaction are many, depending on their living environment; daily family and community life may be an ideal setting for potential social changes towards more health promotion.[10] We therefore set out to develop a woman-centered educational program to strengthen knowledge and responsible behavior for primary prevention of lung cancer.
INTERVENTION
The universe comprised 149 women enrolled in courses in January 2012 at the Women and Family Center run by the Cuban Women’s Federation in Ranchuelo Municipality, Villa Clara Province. Participants were women with no reported addictions (including smoking) who gave written consent to participate. Of these, 16 dropped out, leaving a study population of 133.
The program was developed in three stages. The first diagnostic and cross-sectional stage aimed to identify the women’s learning needs. The second developmental stage was creation of an educational program, with expert validation and implementation. In the third, quasi-experimental stage, the program was carried out and then evaluated by women users, and one year later, the influence these women had on their families was assessed. In the diagnostic stage, the distribution of selected variables was established and the survey instrument and detection model for learning needs were designed, using the approach described by Cabrera.[8] The survey instrument was developed after review of bibliography and other instruments with similar purposes. Its content was validated by three experienced (>10 years) psychologists, as well as by a pilot test with 15 local women, in order to evaluate question comprehension. The survey contained both open-ended and closed questions and was self administered.
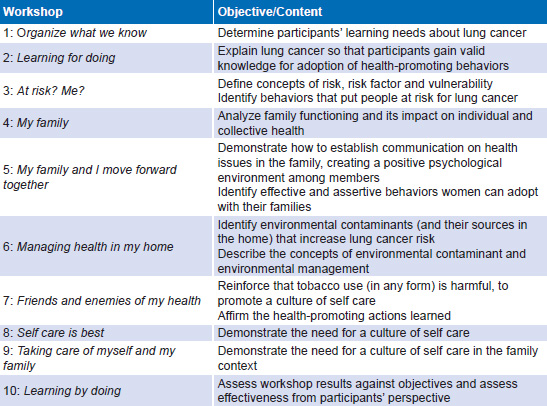
The educational program was developed in the second stage, based on results from the diagnostic stage. The program consisted of a series of 10 weekly 90-minute workshops (listed in Table 1), delivered to 9 groups of 10–15 participants each, in which interactive educational activities were carried out.
In each workshop, lessons and tasks from the previous meeting were reviewed before new content was addressed, concluding with summarizing and closing activities. Participatory group reflection and motivational techniques that fostered group cohesion were used to build new awareness and skills. Each workshop established specific tasks for attaining objectives. Evaluation was systematic throughout the program, each workshop ending with feedback questions and homework assignments. At the end of the program, a comprehensive evaluation was carried out of knowledge acquired and behavioral changes, including participants’ ability to clearly convey to their families what they had learned.
Participatory techniques were used for building collective awareness and encouraging skill acquisition. These techniques were validated by experts selected from an initial nominal list of individuals fulfilling the following criteria: subject knowledge and infl uence on perceptions of health promotion’s importance in lung cancer prevention (determined by reviewing their publications, research and teaching experience). From a potential group of 20 experts, 12 were selected (2 men and 10 women, 4 with doctorates and 8 with master’s degrees) from 3 provincial medical universities (in Havana, Villa Clara and Cienfuegos provinces).
Table 1: Educational program themes and content
Evaluation To assess intervention effect, we examined sociodemographic and epidemiologic variables; self-reported awareness of tobacco harm, environmental management and self care; and health-promoting behaviors.
Sociodemographic variables Age in 10-year groups (20–29 years, 30–39, 40–49, 50–59), schooling (middle school, high school, technical training), occupation, household composition (nuclear family: couple and children; extended: nuclear family plus grandparents; enlarged: extended plus any other relative or friend).
Epidemiologic variables Personal and family history of lung cancer.
Awareness regarding
- harm from tobacco use (identification of its effects and association with lung cancer)
- environmental management (identification of actions—occupational and domestic—that reduce lung cancer risk)
- self care (identification of actions a person should perform to
- benefit her body, preserve health and prevent lung cancer)
The following scale was used to assess awareness:
- high: correct responses to 70%–100% of questions
- moderate: correct responses to 60%–69% of questions
- low: correct responses to <60% of questions
Health-promoting behaviors
Reported performance of environmental management actions to reduce lung cancer risk, such as:
- decreasing use of bleach and chemical disinfectants in domestic chores (washing, scrubbing, cleaning bathrooms)
- avoiding exposure to gas and vapor from oils and fats
- decreasing use of insecticides and chemical products (air fresheners) at home
- avoiding burning garbage
- avoiding unprotected fumigation in agricultural work
- avoiding application of herbicides at home
- avoiding consumption of foods exposed to insecticides
- avoiding use of asbestos
Three aspects of self care (actions taken by the person herself—paying attention and taking care of her body to maintain health and prevent lung cancer) were assessed: awareness, and development of behavioral and of communication skills.
The following scale was used to assess health-promoting behaviors:
- acceptable: 80%–100% of women and their families take actions to manage their home environment
- somewhat acceptable: 60%–79% of women and their families take actions to manage their home environment
- unacceptable: <60% of women and their families take actions to manage their home environment
At the end of the workshop series, participants gave feedback on program content, activities and processes (experiences, participation and instructor performance, among others). Additionally, they reported overall satisfaction on a 1–10 scale, 1–3 was low satisfaction, 4–6 moderate and ≥7 high satisfaction.
To assess the program’s longer-term influence on the women and their families, participants completed another written questionnaire one year later. The questionnaire considered communication (their ability to share health issues and knowledge with their families), whether their families listened to them (whether they succeeded in instilling positive change and persuaded their relatives to take health-promoting actions) and behavior (frequency with which they and their families performed health-promoting actions modeled in the educational program).
Analysis Data were summarized in absolute and relative frequencies. For before-and-after comparisons, the marginal homogeneity test was applied, with significance threshold set at p = 0.05.
RESULTS AND LESSONS LEARNED
Most of the 133 participants (116, 87.2%) were aged 40–49 years. The most frequent educational level completed was high school (53, 39.8%), with ninth grade and technical training equally distributed (40 each, 30.1%). Married women were the largest group by marital status (90, 67.7%), and housewives the largest occupational group (89, 66.9%). Most women (116, 87.2%) had children, and enlarged families predominated (74, 55.6%). Family history of lung cancer was reported by 64 participants(48.1%).
Workshops had 100% attendance and punctuality. However, session participation and task performance were not spontaneous and had to be stimulated by researchers with participatory animation techniques.
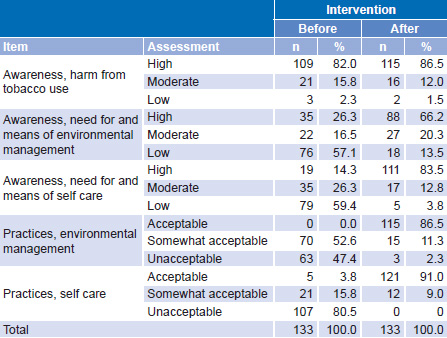
Table 2 shows participants’ reported awareness and practices before and after the workshop program. The proportion of participants with high awareness of harm due to tobacco use increased slightly, from 82% (109/133) before to 86.5% (115/133) after intervention. Fewer were highly aware of actions for environmental management (35, 26.3%) and self care (19, 14.3%) before the program; both increased substantially afterwards, to 66.2% and 83.5%, respectively (Table 2); both shifts were statistically significant (p < 0.001 in both cases).
Table 2: Self-reported awareness and practices before and after educational program (n = 133)
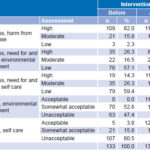
The proportion of women who reported acceptable levels of environmental management practices improved after the intervention, from 0% to 86.5% (p <0.001). Similarly, the proportion with acceptable levels of self-care practices increased from 3.8% to 91.0%. None of the women reported unacceptable levels of self care practices after the intervention (p <0.001) (Table 2).
One year after the intervention, the effect on family communication was explored through participant self report. Before the intervention, all women reported ineffective communication behaviors with their families (yelling, repeating themselves, verbal aggression, etc.); one year later, 66.2% of them reported effective communication with their families, especially regarding health matters.
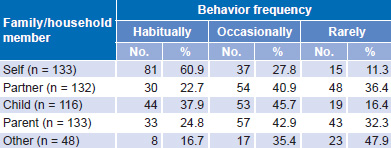
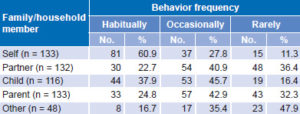
Participants believed that the intervention influenced them and their families, with respect to applying acquired knowledge. The intervention had a greater influence on the women themselves, with 60.9% reporting habitual application. They reported relatives’ application of program recommendations mainly as occasional. Among relatives, children were the most influenced (37.9% habitual) (Table 3).
All women reported that the workshops fulfilled their expectations regarding training objectives, providing them with new skillsor tools to act as health promoters at home. They reported that group work was instrumental in acquisition of knowledge and abilities. Participants reported that more assistance was needed in environmental management at home and effective techniques to improve self care. Regarding communication, all stated that, after the workshop, they felt they were being listened to, mostly by their children, then by their spouses, parents and others, all of whom they helped to improve self care.
Table 3: Reported frequency of any health-promoting behavior by participants and their families one year after educational program
This experience suggests that a woman-centered educational program can increase awareness and health-promoting behavior related to lung cancer. Designers of such programs should take into account women’s ability to communicate and transfer lessons learned cognitively and behaviorally to their family members, and thus contribute to improving community health.