INTRODUCTION
Chronic kidney disease (CKD) is an important global health concern, contributing to cardiovascular disease and end-stage renal disease.[1–4] The estimated global prevalence of CKD is approximately 8–16%, with significant variability across different geographic regions.[1] Worldwide mortality from CKD was 16.3 per 100,000 annually in 2010.[5] Traditional risk factors for CKD in low-income countries are similar to those in high-income countries: aging, diabetes, hypertension and use of nephrotoxic medications.[1,4,6] Other factors—including infections (such as leptospirosis), pesticide and other chemical exposures, herbal medications and food additives—may play a more prominent role in resource-limited settings.[6,7]
Since the early 2000s, a unique epidemiological pattern of CKD has been described in the Pacific lowlands of Central America, disproportionately affecting male agricultural workers, some aged as young as late 20s and early 30s.[8–14] In the fall of 2012, stakeholders at the First International Research Workshop on Mesoamerican Nephropathy (FIRWMN) developed a consensus definition of “Mesoamerican Nephropathy” (MeN), including the documentation of abnormal kidney function by internationally accepted standards related to no known cause of CKD.[8] A small biopsy series of suspected MeN cases in El Salvador demonstrated prominent tubulointerstitial injury and glomerulosclerosis with minimal vascular changes.[15]
Studies of men living in affected regions of Central America have reported a high prevalence of decreased kidney function, with an estimated glomerular filtration rate (GFR) <60 mL/min/1.73 m2 observed in 15–35% of men.[10–13] In a 2008 study in Chichigalpa, Nicaragua, where the current investigation took place, 31% of male participants had an estimated GFR <60 mL/min/1.73 m2.[16]
Several current hypotheses about MeN etiology in the Pacific region of Central America emphasize the potential of heat stress and dehydration as risk factors.[17] Heat stress has been linked to CKD in Thailand;[18] and occupations disproportionately affected by the disease in Central America, such as mining and agricultural work, involve high levels of heat stress.[19–21] A recent animal study demonstrated heat stress can produce kidney damage consistent with that found in Nicaragua.[22] However, because heat stress is not an exposure unique to Pacific Central America, and heat increases over the past two decades are likely insufficient to solely account for the epidemic, other factors are likely involved. Proposed cofactors include exposure to agrochemicals such as 2,4 D and paraquat dichlorate, which have been associated with acute kidney injury,[23] NSAIDs and nephrotoxic antibiotics,[24] infections such as leptospirosis,[25] and exposure to heavy metals.[20] High fructose intake leading to metabolically induced inflammatory kidney damage has also been proposed, based on work in animal models.[22,26,27]
Past studies have shown agricultural workers are at increased risk for MeN.[8–14] This study describes the prevalence of reduced GFR in a region of Nicaragua suspected to harbor high rates of MeN and investigates potential risk factors. It investigates in greater depth specific behaviors and exposures related to agricultural work and their association with reduced GFR in the region, as well as association between reduced GFR and traditional risk factors such as diabetes and hypertension.
METHODS
Design, setting, and participant recruitment A cross-sectional design with nested case-control analysis was employed for its efficacy in rapidly exploring a broad number of population characteristics and risk factors. The study was conducted in a community near the town of Chichigalpa, Nicaragua, in which past investigation had identified a high prevalence of CKD.[16] Initial recruitment was conducted via census, with inclusion criteria encompassing all individuals aged 15–69 years living permanently in a community household (684 identified); pregnant women were excluded.
Participants were recruited using door-to-door canvassing in May–June, 2012. Demographic surveys were administered during recruitment to one household representative—generally the female head of household because of greater availability—who reported demographic information for all other individuals living in the home. All eligible household members were invited to a single study visit at a central location for interview and physical measures.
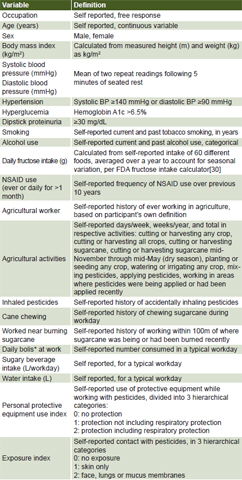
Study variables The dependent variable in this study was reduced GFR, estimated from serum creatinine using the 2009 CKD-EPI formula.[28] “Reduced GFR” was defined as single GFR < 60 mL/min/1.73 m2, which encompasses the quantitative GFR criterion for CKD stages 3–5, but with our point sample the time criterion for CKD diagnosis could not be met.[29] The cutoff value was chosen to minimize false positives from transient, mildly elevated creatinine due to diet or physical activity. Independent variables are listed and defined in Table 1.
Data collection This took place over eight weekend days in July–August 2012. Each participant attended a single session that included researcher-administered questionnaires, a focused physical examination, and collection of blood and urine specimens. Physical examination included measurement of height, weight, and blood pressure—the latter measured on right arm with automatic sphygmomanometer (Omron, Japan), cuff size specific to arm circumference.
An additional survey on conditions of agricultural work, adapted from validated surveys developed by the US Agricultural Health Study, was administered to each participant who reported a history of agricultural employment.[31] Survey questions were adapted to reflect aspects of agricultural work specific to Nicaragua.
Agricultural workers were asked to report the different jobs they had done in agriculture over their working lives. For each job, we asked how many years, hours per day, days per week, and weeks per year they had worked. Workers were asked whether they had ever to their knowledge worked in or near areas where pesticides were being applied, how far they worked from where pesticides were being applied, and how long they waited to re-enter areas where pesticides had been applied. Pesticide applicators were asked to name the chemicals they used.
Table 1: Independent variables

*sugary rehydration packet
Anyone who reported a history of mixing, applying or working near pesticides was asked how many days per year they were exposed, what sort of personal protective equipment they used, the consistency with which they used protective equipment, and which areas of their body were generally exposed to agrochemicals.
Sample collection and processing Each participant provided an early morning, midstream urine sample, self collected in a BD Vacutainer urine collection cup. Venous blood samples were drawn using a BD Vacutainer collection kit and split into two 5-mL pink-top EDTA tubes and one 5-mL gold-top serum separator tube (Becton, Dickinson & Co., USA). Participants aged < 25 years used only the EDTA tubes because we did not measure their HbA1c.
Within 30 minutes of collection, blood samples were centrifuged for 5 min at 3500 rpm using a Hettich EBA20 portable centrifuge (Hettich, Germany);[32] 1 mL of serum was separated for determination of serum creatinine. Serum samples and whole blood samples were transported on ice and stored at −25ºC at the Center for Investigation in Health, Work and the Environment (CISTA, the Spanish acronym) laboratory at the National Autonomous University of Nicaragua UNAN (the Spanish acronym) at León. Within seven days, samples were transported to the UNAN-León Medical Center, where they were processed using the Jaffé compensated method[31] in a Cobas Integra 400 system (Roche Diagnostics, USA). Whole blood specimens were analyzed for HbA1c within 24 hours of specimen collection using a Stanbio Glycohemoglobin Direct Test (Stanbio Laboratory, USA). Urine samples were analyzed on site within 30 minutes of collection, using a Bayer Clinitek 50 Urine Chemistry Analyzer with Multistix 10SG reagent strips (Siemens Diagnostics, Germany).
Data analysis Data on GFR were used to calculate prevalence of reduced GFR. We then selected a subset of participants based on GFR for case-control analysis to assess risk factors for reduced GFR, with cases defined as individuals with a single GFR calculation <60 mL/min/1.73 m2 and controls defined by GFR >90 mL/min/1.73 m2. Individuals with GFR 60–90 mL/min/1.73 m2 were excluded from risk factor analysis because the CKD-EPI equation has not been validated for this population. Exclusion of these individuals also ensured adequate differentiation between GFR groups.
Logistic regression was chosen over linear analysis due to CKD-EPI validation concerns because it was felt that logistic regression would help minimize error resulting from small fluctuations that may exist in applying CKD-EPI in this population. Comparisons of disease prevalence with the 1999–2004 US National Health and Nutrition Examination Survey (NHANES) cohort[33] was conducted using chi-square analysis with Yates correction because of NHANES large n. Comparisons of prevalence among male and female study participants were conducted using the Fisher exact test. Association between potential risk factors and reduced GFR status was determined using bivariate and multiple logistic regression. Variables significant or marginally significant at p <0.05 in univariate analysis were included in multiple regression models, and excluded using backwards regression with p >0.1 as cutoff.
For multivariate analysis among agricultural workers, each variable was evaluated independently using models with only age and sex as covariates due to the lower n compared to the overall population. Sensitivity analyses were conducted using linear regression, with GFR as the continuous response variable. Linear analyses included the entire study population rather than just those selected as cases and controls. All analyses were conducted using SPSS v. 20.
Ethical considerations Participants gave written informed consent, with parents of participants younger than 18 consenting for their children. Protocols were approved by the Mount Sinai Institutional Review Board and the UNAN-León Ethics Committee.
RESULTS
In total, 424 people participated (166 men, 258 women), representing 62% of the eligible population (50.5% of 329 eligible men and 72.7% of 355 eligible women). Participants were slightly older than the overall community population, but the difference was small and did not reach statistical significance for men (mean age 32.1 vs. 29.9 years, p = 0.07) or women (34.8 vs. 33.0 years, p = 0.11). Among participants, 72% of men and 12% of women currently or previously worked in sugarcane agriculture, as compared with 69% of men and 12% of women in the overall census population. One hundred fifty-one participants with an occupational history in any form of agriculture responded, representing 58% of agricultural workers identified in the census population.
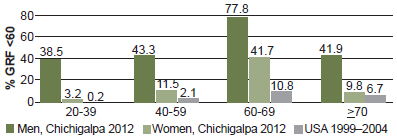
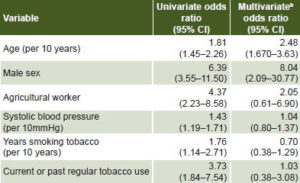
Prevalence of reduced GFR and proteinuria Among the 401 participants who provided blood samples, prior to exclusion of individuals with GFR between 60 and 90 mL/min/1.73 m2, mean GFR was 87.5 ± 30.7 mL/min/1.73 m2 (77.9 ± 37.3 among men, 94.0 ± 23.1 among women, p <0.001). Prevalence of GFR <60 mL/min/1.73 m2 was 22.6%, and was higher in men (41.9% vs. 9.8% in women, p <0.001). When stratified by age, prevalence of decreased GFR was significantly greater in men in all age groups <60 years, and was higher among men aged 60–69 years, although not to a statistically significant degree (Figure 1). Prevalence estimates from US NHANES are provided for context.[33] In univariate analysis (Table 2), older age, male sex, history of work in agriculture, and use of tobacco and alcohol were associated with reduced GFR. Dipstick proteinuria was assessed in 389 participants (92%), among whom proteinuria ≥30mg/dL was present in 15%. Among participants with GFR <60 mL/min/1.73 m2, 44% had proteinuria ≥30mg/dL and only 7 participants (9%) had proteinuria ≥300 mg/dL.
Figure 1: Prevalence of reduced GFR* by sex and age in a Nicaraguan community (2012) and in USA (1999–2004)
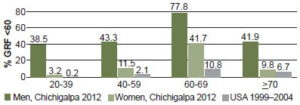
Source: US data are from 1999–2004 US NHANES cohort[33] / *Glomerular filtration rate < 60 mL/min/1.73 m2 body surface area
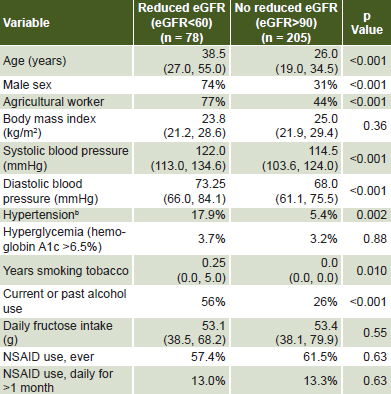
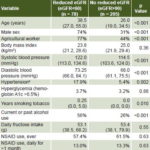
Association with traditional CKD risk factors Among 327 participants who underwent standardized blood pressure measurement, systolic and diastolic BP were significantly higher in participants with reduced GFR. Hypertension was more prevalent among cases than controls (p = 0.002), although overall prevalence of hypertension was only 8.6%. Prevalence of HbA1c >6.5% was 3.7% in case group and 3.2% in control group, consistent with a prevalence of self-reported diabetes of 3.4% in the overall census population, and did not differ between groups (p = 0.88). NSAID use was common (>70% in both cases and controls), but daily use was rarer (13% in cases and 13.3% in controls) and there was no significant difference between cases and controls (p = 0.44). Use of nephrotoxic medications was <1%. In multivariate analysis—including all variables significant in univariate analysis (p <0.05) and using backwards logistic regression (with exclusion criteria: p >0.1)—only older age and male sex remained significantly associated with reduced GFR (Table 3, where data presented show all variables included in model). In sensitivity analysis using linear regression with GFR as the continuous response variable, results were qualitatively similar (data available upon request). Significant variables identified in sensitivity analysis were identical to those identified in case-control analysis.
Table 2: Univariate analysisa of risk factors for reduced GFR in a Nicaraguan community
aBinomial logistic regression; median (1st quartile, 3rd quartile) for continuous variables; percentages for categorical variables / bHypertension: systolic pressure ≥140 mmHg or diastolic pressure ≥90 mmHg
Table 3: Case-control analysis of risk factors for reduced GFRa in a Nicaraguan community
aCase: glomerular filtration rate (GFR) <60 mL/min/1.73 m2
Control: GFR >90 mL/min/1.73 m2
bMultiple logistic regression with all variables included
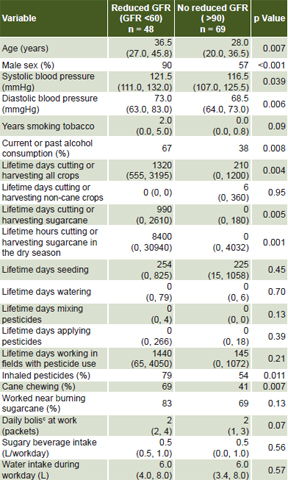
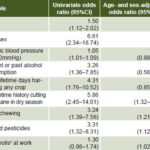
Specific agricultural exposures and reduced GFR Prevalence of reduced GFR among agricultural workers was 31.4%. In univariate analysis, risk factors for reduced GFR identified in the overall population were similar to those in agricultural workers, with the notable exception of systolic blood pressure. Study participants who worked in agriculture predominantly worked in sugarcane (83%), although some cane workers additionally reported subsistence farming on private plots and/or working in other agricultural activities in the past. Respondents reported a number of different occupational activities, including cutting cane and harvesting other crops, seeding the fields, mixing and applying pesticides, and managing irrigation. Among agricultural tasks, only lifetime days cutting or harvesting crops, and lifetime days specifically cutting or harvesting sugarcane were significantly associated with reduced GFR (Table 4).
Table 4: Univariatea analysis of risk factors for reduced GFRb in current or former agricultural workers in a Nicaraguan community

aBinomial logistic regression; median (1st quartile, 3rd quartile) for continuous variables; percents for categorical variables
bGlomerular filtration rate <60 mL/min/1.73 m2
cBolis: sugary rehydration packet
Consumption of bolis (sugary rehydration packets given to workers) was marginally associated with reduced GFR. Water intake during the workday, other sugary beverage intake during the workday, and a history of burning sugarcane or working near areas where cane was being burned were not associated with reduced GFR (Table 4).
Level of personal protective equipment worn was not significantly associated with reduced GFR (p = 0.35). Personal pesticide exposure route (face/lung/mucus membrane vs. skin vs. no exposure) was significantly associated with reduced GFR among individuals who mixed and applied pesticides (p = 0.03) but not individuals who reported exposure while doing other tasks (p = 0.51). Past inhalation of pesticides was also significantly associated with reduced GFR, as was chewing sugarcane during the workday. Pesticides reported as most commonly used were Hendal 2,4 D, Roundup (glyphosate), and Gramoxone (paraquat).
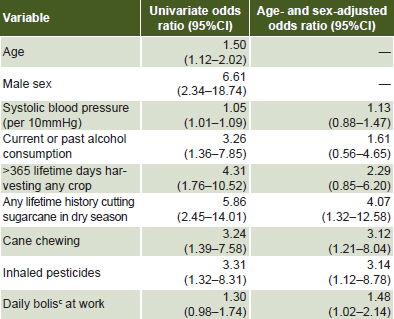
In models adjusted for age and sex, cutting sugarcane in the dry season showed the strongest association with reduced GFR. History of chewing sugarcane and inhaling pesticides also retained their significance after adjustment for age and sex, while daily bolis consumption became significant (Table 5). In models adjusted for total hours cutting sugarcane during the dry season, bolis consumption (OR 1.39, 95% CI 0.99–1.95) and inhaling pesticides (OR 2.61, 95% CI 0.99–6.90) were marginally significant and chewing sugarcane was still significant (OR 2.74, 95% CI 1.11–6.77), with total hours cutting sugarcane during the dry season retaining significance in all models (p <0.002).
In sensitivity analysis using multivariate linear regression, controlling for age and sex, only lifetime hours cutting cane in the dry season, accidental inhalation of pesticides, and diastolic blood pressure remained significant predictors of reduced GFR among agricultural workers (data available upon request). Male sex was no longer significantly associated with reduced GFR in the model incorporating lifetime hours cutting sugarcane in the dry season.
Table 5: Age and sex-adjusted analysisa of reduced GFRb risk factors in a Nicaraguan community
aBinomial logistic regression with variables significant or marginally significant in univariate analysis (p <0.01)
bGlomerular filtration rate <60 mL/min/1.73 m2 body surface area
cBolis: sugary rehydration packet
DISCUSSION
In this cross-sectional, population-based survey, we identified a high prevalence of reduced GFR, based on single-measure GFR calculations <60 mL/min/1.73 m2. We demonstrated that traditional etiologic factors for reduced GFR such as diabetes, hypertension and use of nephrotoxic medications are not major contributors to disease in this population, while specific agricultural tasks and exposures may be important determinants. Our results are consistent with MeN disease patterns identified in other studies in Central America.[10–13]
The observed prevalence of decreased GFR in our study was over three times that of NHANES after stratifying by age, and was over five times greater among men.[33] Because most people with advanced CKD in this region of Nicaragua do not undergo dialysis,[34] it is likely that the duration of disease is shorter in this community compared to the USA due to decreased survival. This suggests that the difference in incidence between the two populations is likely even greater than the difference in prevalence.
While we lack biopsy samples to confirm pathologic changes, our findings are consistent with all other characteristics of MeN proposed by the FIRWMN. Reduced GFR in this community predominantly presented with minimal or no proteinuria, and traditional risk factors for CKD were not important contributors. Use of NSAIDs was relatively common in this population but was not associated with risk for reduced GFR, making it an unlikely sole etiologic factor. Other nephrotoxic medications were used too infrequently to be responsible for an epidemic of this magnitude. Uncontrolled diabetes was rare in this population, with no significant difference between participants with and without reduced GFR.
Although blood pressure was significantly higher among participants with reduced GFR and was found to be significantly associated with reduced GFR among agricultural workers, mean systolic and diastolic blood pressure was in the normal range for both cases and controls and hypertension was present in <10% of the overall population. Additionally, kidney disease can produce elevated blood pressure, so the association found may reflect a consequence rather than cause of CKD. Hypertension may contribute to some cases of reduced GFR in this population, but is unlikely to be a principal causal factor responsible for MeN.
Our findings have important implications for the hypothesis that heat stress is a risk factor for MeN. Aside from age and male sex, the strongest independent association observed was between reduced GFR and lifetime hours cutting sugarcane, particularly during the dry season. Cane cutting is known to subject workers to extreme levels of heat stress; a study of cane harvesting in Costa Rica showed that workers should only engage in cane cutting 15 minutes of every hour in order to meet US Occupational Safety and Health Association (OSHA) standards for health risks from heat.[19] Most sugarcane workers in this area report taking few breaks during an 8–12 hour workday (data available upon request), a finding corroborated by studies of sugarcane workers in other countries.[19,35]
While time spent cutting sugarcane has inherent collinearity with age, a known risk factor for CKD, its retained significance when correcting for age and the lack of association found with cumulative hours indicates its effect cannot be accounted for by age alone, and strongly suggests a role for heat stress in the etiology of MeN in this population. Of concern, climate change models predict that high heat stress days for workers in Nicaragua are likely to increase by 15% in coming decades.[36]
Prior studies have suggested that dehydration may contribute to MeN in this region.[19,34] Our results do not show an association between water intake and disease status, and water intake was close to the OSHA suggested levels in both groups.[37] However, water intake may not be an effective proxy for hydration status, given the strenuous working conditions and high level of heat stress to which these individuals are subjected. Future studies should consider more sensitive measures of hydration status during the workday to elucidate the specific role of dehydration.
The three most commonly used pesticides reported on sugarcane plantations (2,4-D, glyphosate and paraquat) are all known nephrotoxins.[23] A history of accidental pesticide inhalation, as well as a history of chewing sugarcane during the workday (which may represent a source of oral pesticide intake) were associated with reduced GFR in the logistic univariate and multivariate analysis. Additionally, increased self-reported lifetime days mixing, applying, and working near pesticides were significant predictors of GFR in univariate linear analysis. However, this relationship was not observed in binomial logistic analysis, which we believe to be the more appropriate test because the CKD-EPI equation used to calculate GFR has not been validated in this population.
Past studies have suggested that consumption of alcohol, particularly homemade, may be linked to MeN.[12] Alcohol consumption in this study was associated with reduced GFR both in the overall population and among agricultural workers in univariate analysis, but was no longer significantly associated with reduced GFR in multivariate analysis. This study cannot exclude alcohol consumption as a contributing factor to MeN.
One key hypothesis identified at FIRWMN was that high fructose intake may interact with fluid volume depletion and heat stress to produce inflammatory damage to the kidney.[22,26,27] Our findings demonstrate increased fructose intake overall is not associated with reduced GFR, nor is sugary beverage consumption during the workday. However, consumption of bolis and chewing sugarcane at work were found to be associated with increased risk. Chewing sugarcane and bolis consumption is a mechanism for substantial sugar intake when people are actively working in the fields, while soda is more typically consumed during lunch only. Therefore, our findings support the hypothesis that fructose intake while engaged in heat stress-producing activities contributes to kidney injury. Chewing sugarcane may also represent an oral route for pesticide exposure, or a route for exposure to leptospirosis. When controlling for total hours worked cutting sugarcane during the dry season, bolis consumption, chewing sugarcane, and history of pesticide inhalation all retained significance or marginal significance, suggesting increased sugar consumption during the workday and pesticide exposure may be risk factors in themselves for MeN, rather than merely variables which are more common among individuals who have worked the longest or worked in certain jobs.
Although this study provides novel, detailed information on agricultural activities and exposures as contributors to the MeN epidemic, several limitations must be acknowledged. Our response rate was only 62%, and not all participants took part in every aspect of data collection. The main reason for nonparticipation was disinterest, possibly due to study fatigue, given that several past studies had also been based in this community. Nonetheless, the study population was demographically similar to the population as a whole, and was drawn from the entire population rather than a randomly selected subset.
This study employed a cross-sectional design, a method able to assess past exposures but limited in its ability to determine causality. We used only single measures of serum creatinine to calculate GFR and assign reduced GFR, but attempted to ensure cases truly did represent CKD by setting the GFR cutoff at a level corresponding to stage 3 or higher. We sampled nearly all individuals at least 12 hours after they last worked and 8 hours after they last ate meat. Survey questions were adapted from validated studies, but were not themselves validated in the population studied, and are also subject to recall bias. Finally, we used simple models to explain what is thought to be a disease with a complex multifactorial etiology, so nonlinear and nonbinary interaction between these risk factors with respect to reduced GFR may have been lost. Nevertheless, the fact that sensitivity analysis using linear regression generally corroborated the logistic regression findings supports the validity of our results.
CONCLUSIONS
This study provides further evidence for an epidemic of CKD that is not associated with traditional risk factors such as diabetes, hypertension or NSAID use. Our findings suggest that sugarcane cutting and harvesting is an important risk factor for development of this disease, which appears to be driven by a multifactorial combination of heat stress and concurrent sugar consumption, with possible contribution of pesticide exposure. Further study is needed to more fully assess disease mechanisms.
ACKNOWLEDGMENTS
The authors thank the following for their help in this project: Martha Aragón and the rest of the staff at CISTA; Jason Glaser, Eugenia and Juan Salgado, Christian Velásquez, Viola Cassetti, Aleksandra Peresic, Dorien Faber, Katie Stark, Maya Scherr-Wilson, Marissa Ocampo and the other staff and volunteers at La Isla Foundation; Nubia González, Hector Paniagua, Soadth Meyuonni, Denise Pérez and Ana Chávez from UNAN-León; and most importantly the participating community in Chichigalpa, Nicaragua. Funding was provided by the Icahn School of Medicine at Mount Sinai Global Health Department and the research arm of La Isla Foundation (Nicaragua).