ABSTRACT
INTRODUCTION Despite growing research interest in the epidemic of chronic kidney disease of nontraditional etiology (a distinct form of chronic kidney disease disproportionately affecting agricultural populations across Mesoamerica—Central America and southern Mexico), its etiology remains poorly understood.
OBJECTIVE Elucidate factors that impact researchers’ efforts to understand the epidemic of chronic kidney disease of nontraditional etiology.
METHODS Semistructured interviews were conducted with 39 international researchers, selected based on their publications and participation in conferences about chronic kidney disease of nontraditional etiology. Interviews were conducted from May through September of 2015 in English or Spanish by video conference, telephone or in person. Interviews were audio recorded, transcribed, and analyzed iteratively using content analysis.
RESULTS Of 39 researchers interviewed, 30.8% were women, 84.6% had a medical and/or doctoral degree and 74.3% had ≥6 years’ experience carrying out research on chronic kidney disease of nontraditional etiology. Three major themes were identified related to factors affecting research progress. The first, influence of state and private interests, concerned perceptions that sugar industry and some governments in Mesoamerica dismissed, hindered, intimidated and inaccurately represented research on chronic kidney disease of nontraditional etiology. The second, limited material and human resources, had to do with scarcity of stable, impartial funding and adequate in-country research infrastructure. Researchers were largely funded by nontraditional sources (charitable organizations, private donations, sugar industry in Mesoamerica, personal funds) or not funded at all. The third, logistical challenges across study lifetimes, referred to barriers such as unwieldy approval mechanisms, gang interference and publication hurdles.
CONCLUSIONS Producing high quality and clinically relevant studies to address chronic kidney disease of nontraditional etiology in the resource-scarce Mesoamerican research climate has been fraught with challenges. These findings contextualize the progress that has been made in understanding chronic kidney disease of nontraditional etiology to date and highlight the need for public health and biomedical organizations to support researchers’ ongoing efforts to engage all stakeholders in addressing the epidemic, disseminate their research findings and identify feasible strategies for addressing the community-wide suffering caused by chronic kidney disease of nontraditional etiology.
KEYWORDS Chronic kidney disease, chronic renal insufficiency, chronic renal failure, chronic kidney failure, interstitial nephritis, qualitative research, epidemiology, occupational health, Costa Rica, El Salvador, Guatemala, Mexico, Mesoamerica, Nicaragua
INTRODUCTION
Chronic kidney disease of nontraditional etiology (CKDnt), also called chronic interstitial nephritis of agricultural communities and Mesoamerican nephropathy, among other names, is a distinct form of chronic kidney disease that disproportionately affects young male agricultural laborers in communities along the Pacific coast of Central America.[1,2] Although historical data are lacking, this epidemic is estimated to have caused at least 20,000 deaths in this region in the last 2 decades.[1,3,4] Furthermore, other countries, notably Sri Lanka and India, are experiencing what many researchers argue are clinically and etiologically similar outbreaks of CKDnt.[2,5,6]
Since the first peer-reviewed article about this phenomenon in Mesoamerica (which includes Central America and Southern Mexico) was published by a team of Salvadoran investigators in 2002, a small but growing group of researchers—along with local governments, scientific societies, PAHO and WHO—has mobilized to investigate this notion further.[7–9] They have found, among other key insights, that CKDnt disproportionately affects sugarcane harvesters. Although the disease has been shown to also affect men not employed in agriculture, women and children, much research has focused on agricultural workers and, specifically, sugarcane harvesters, given the disproportionate burden in this population. Sugarcane in Mesoamerica today is mostly produced in expansive monoculture plantations owned by powerful conglomerates.[10] Sugar plantations in these countries rely on local manual labor to sustain their large-scale production. Sugarcane cutters are the men and (less often) women who use machetes to cut down ripe sugarcane by hand, so it can be processed in mills. These cutters are often exposed to intense heat, pesticides, long shifts and other hazardous working conditions, and are paid meager, piecework wages, both keeping workers poor and incentivizing overexertion.[11,12] However, as the amount of land used for sugarcane production has grown in many places across Mesoamerica and many young, undereducated and impoverished individuals in these areas may have few other employment options, many become sugarcane harvesters out of necessity.
IMPORTANCE Findings suggest opportunities for facilitating progress toward nuanced understanding of the epidemic of chronic kidney disease of nontraditional etiology in Mesoamerica, which may have positive implications for affected populations.
CKDnt’s etiology remains poorly understood, despite mounting research interest and efforts by ministries of health to engage national and international experts with the support of international public health agencies.[13] For example, although researchers agree that CKDnt is multifactorial, involves complex macro-level social determinants of health and is not associated with diabetes or hypertension—leading causes of chronic kidney disease globally—more specific causes have yet to be identified.[1,3,4,8] Previous research has focused on investigating risk factors and causal hypotheses (including recurrent heat stress and dehydration, pesticides, infectious agents and heavy metals) to address these gaps in basic and clinical understanding.[14–19] Some investigators have begun developing targeted interventions to protect affected communities, based on findings from this etiological research.[10] Given that renal replacement therapies are often scarcely available and prohibitively expensive for patients in this region, such intervention efforts are especially important.[20]
To date, no studies have assessed the challenges of carrying out CKDnt research from researchers’ perspectives. In light of discussions of the challenges of CKDnt research in some editorial commentaries and news media coverage of the role of the sugar industry and national governments in responding to the epidemic, this research explores how these and other factors may have shaped CKDnt research.[21–23] Understanding such influences may help researchers advance toward a comprehensive, unified understanding of CKDnt, with positive implications for affected populations.
This qualitative study involved semistructured interviews with a diverse sample of leading international researchers studying CKDnt in Central America and Mexico. The primary aim was to elucidate factors that have impacted researchers’ efforts to understand the disease. Better understanding the context in which CKDnt research has been conducted to date can help identify specific strategies to facilitate high-quality, clinically relevant CKDnt research.
METHODS
Design and population A multidisciplinary team, including a medical anthropologist and an environmental sociologist, developed an interview guide for this project. This guide included questions and probes about participants’ understanding of CKDnt, their own CKDnt research and perceptions of the CKDnt research environment. Experts in qualitative methodology on our team provided training for conducting semistructured interviews and data analysis, as well as input and feedback on all aspects of the study.
We selected participants purposively, with the objective of sampling individuals extensively familiar with and involved in CKDnt research from across demographic and relevant, expertise-related variables. We began this process by conducting a review of peer-reviewed literature and publicly available attendance lists for international conferences about CKDnt. We identified a list of 101 researchers involved in such work who had attended at least one conference and/or been a coauthor on multiple peer-reviewed articles about CKDnt. We narrowed this list down by focusing on senior and active members of research teams when multiple individuals from one research group were captured and selecting individuals with distinct training (medical, doctoral, or master’s degree), expertise, length of involvement in CKDnt research, geographical location and institutional affiliation(s). We initially invited 69 researchers to participate.
Data collection and processing Of the 69 researchers we initially invited to participate, 54 (78.3%) responded, 1 of whom declined to participate due to perceived lack of relevant experience to contribute. We interviewed 39 of the 53 (73.6%) who agreed to participate, from May through September 2015. The remaining 14 were not interviewed, either because they did not respond to attempts to schedule an interview or because other members of their research teams with similar roles and training had already been interviewed. Researchers who did not respond to our initial invitation to participate or who did not participate for other reasons did not differ in gender, expertise, or country from those who participated.
Interviews were conducted by video conference, telephone or in person and were audio recorded. One participant participated via Qualtrics survey based on the interview guide because establishing an internet connection reliable enough for live contact was not feasible. Recruitment continued until thematic saturation was reached. Interviews were transcribed verbatim, deidentified and (if in Spanish) translated into English by the study team.
Given the small population of CKDnt researchers, we took rigorous precautions to deidentify participant data and allowed participants to review deidentified quotes prior to inclusion in this publication. All participants directly quoted here were given an opportunity to remove their quote(s) to ensure they did not feel identified.
Analysis Transcripts were analyzed iteratively and collaboratively by inductive content analysis.[24] We began designing a coding structure by open coding three transcripts. A study team member read and annotated them to distill participants’ points, record impressions of them and attend to unifying ideas as well as variations over participant type. After grouping these annotations, we developed a provisional codebook. Our study team reviewed this initial set of codes, providing feedback to address ambiguities and redundancies in the codes. We then applied the codebook to all transcripts. Coding discrepancies were resolved by consensus. New codes were added as they were identified. When a section of a transcript addressed multiple concepts, it was marked with all applicable codes. We also examined whether interview responses differed by participant location (local: from Central America, Mexico, or Cuba; international: from other than Central America, Mexico or Cuba; expatriate: from a country outside of Central America, Mexico, or Cuba, but now living and working on CKDnt in the region). Although Cuba is not within Mesoamerica, we categorized participants from Cuba as “local” given cultural and political similarities between Cuba and Mesoamerica, relative to other “international” countries where participants resided (the USA and European countries), and our interest in the influence of these factors on participant responses. Emergent themes were identified inductively through abstraction of data collected from coding as it progressed and organized into major themes and subthemes.
Ethics This study was exempt from review by the Institutional Review Board (IRB) of Brown University (where the author was studying), but study procedures were conducted in accordance with IRB guidelines for informed consent, participant safety and data quality. All participants provided written informed consent (consent form provided in both English and Spanish).
RESULTS
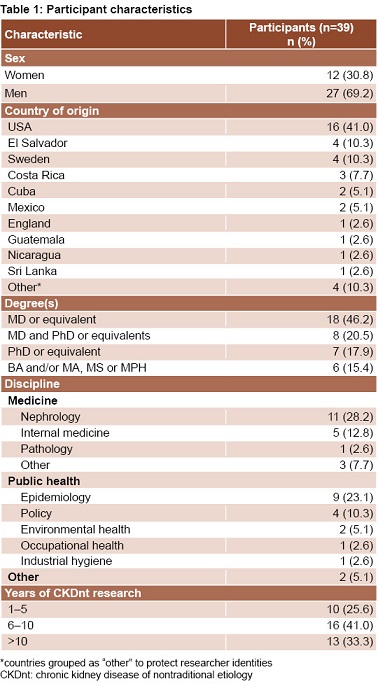
We interviewed 39 researchers from 14 countries, with diverse expertise and experience in CKDnt research from clinical, laboratory, academic and/or field settings (Table 1). Interviews were conducted in English (29/39, 74.4%) and Spanish (10/39, 25.6%) and lasted an average of 46 minutes (range 16–87 minutes). Thematic analysis generated three themes, each with associated subthemes (Table 2).

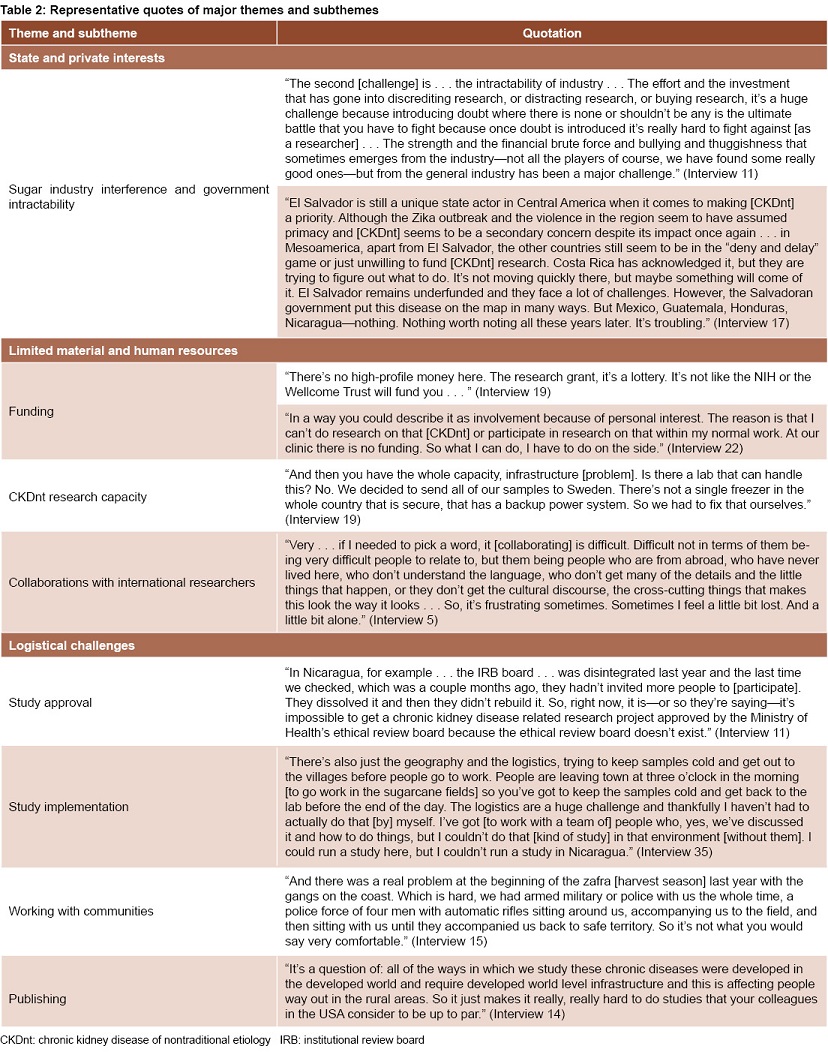
Theme 1: Influence of private and state interests Sugar industry interference and government intractability Although a few instances were identified in which sugar industry and national governments cooperated with or spearheaded responses to CKDnt, participants more often reported that these stakeholders had stymied CKDnt research. Regarding industry, participants said that sugarcane companies had largely refused to participate in studies of CKDnt. Only two research teams had been engaged in long-term work on plantations in the region at the time interviews were conducted. Researchers reported that some sugarcane harvesters who participated in CKDnt research had been fired as a result. Participants said the sugar industry had also misrepresented research findings in company publications. Participants also felt that industry had sometimes targeted CKDnt researchers directly. For example, two participants described being followed, approached or watched by strangers, attributing it to their work on CKDnt. Additionally, three participants reported having received threats (one participant explicitly described them as death threats) because of their work studying links between sugar industry working conditions and CKDnt. Expatriates living and working in Central America expressed concerns about being targeted directly because of their work on CKDnt more often than did national and international researchers.
Governments in Mesoamerica, participants said, had also largely been intractable. Participants’ attention to government roles centered on the lack of monetary and institutional support for CKDnt research and related policy-change efforts. Most participants agreed that Costa Rica and El Salvador had, at least recently, taken a more proactive, coordinated approach to addressing CKDnt. Conversely, many researchers, both from Nicaragua and elsewhere, lamented that the Nicaraguan government continued to dismiss the epidemic. Participants said it had dissolved the Ministry of Health’s ethics review committee (preventing approval of research proposals), issued formal directives to local agencies to not engage in CKDnt research and suppressed government employees who did not support the government stance on the issue.
Theme 2: Limited material and human resources Funding Securing substantial, stable, impartial funding for CKDnt research was widely described by participants as one of the major challenges. Although participants recognized funding challenges were not unique to CKDnt science, high-caliber funding was perceived as acutely scarce in this arena. Most participants’ work was funded by nontraditional sources such as charitable foundations, sugar industry in Mesoamerica, or private donations from friends, family or religious groups. In addition, many participants described using their own personal resources to fund their work on CKDnt. Several of them received no funding at all for their CKDnt research. Suggested reasons for this difficulty obtaining funding included major charitable foundations preferring to fund work to eradicate diseases rather than understand them and Latin America having relatively low priority on the geopolitical agenda for international aid and research support. Many participants linked the slow pace and overall limited scope and quality of CKDnt research to their reliance on piecemeal and limited funding.
Mesoamerican research capacity A majority of participants, from both Mesoamerica and elsewhere, also noted the paucity of infrastructure and high-quality biomedical equipment necessary for CKDnt research in Mesoamerica. For example, electricity can be unreliable in many parts of Mesoamerica, making it difficult to properly refrigerate biological samples. Furthermore, few in-country laboratories are equipped to handle and process these samples. As a result, research teams often rely on point-of-care biological assays, which can be less accurate.
Ten participants, all of whom work from outside Mesoamerica, commented on the availability of highly trained researchers in Mesoamerican countries. Their consensus was that there were too few researchers in Mesoamerica available and/or interested in studying CKDnt in the context of limited funding. Those who did engage in CKDnt research were perceived as overextended and overloaded with other responsibilities, to a greater degree than their US or European counterparts.
Collaborations with international researchers. In part to help address this limited local research capacity, researchers from other regions including the USA and Europe have begun studying CKDnt, a development which drew mixed responses. Several participants, across countries of origin, said that collaborations were productive and that the resources, expertise and media attention contributed by international collaborators had helped improve CKDnt research quality. Others warned that the influx of funding and investigators from abroad may distract from an emphasis on national institutions, funding and researchers. Expatriate researchers working both with international counterparts and national team members sometimes described having difficulty navigating cultural and language boundaries and distinct interests among collaborators.

Theme 3: Logistical challenges across study lifetimes According to participants, carrying out studies in Mesoamerica presents distinct, nontrivial logistical challenges. These factors affected the feasibility and quality of all phases of CKDnt research, from design to data collection and publication.
Study approval Obtaining study approval was often slow and laborious. Researchers affiliated with institutions outside Mesoamerica must get approval at their own institutions and Mesoamerican ones, which may have very different procedures. Three participants described extensive difficulty getting study approval from the Nicaraguan Ministry of Health. One participant described waiting at least two years for study approval.
Study implementation If a project was approved, transporting and supporting equipment and researchers presented another set of obstacles, participants said. Given limited national research infrastructure, some participants described trying to bring laboratory equipment from their home countries to be able to process biological samples. Others had opted to ship samples to the USA or Europe for analysis. For studies examining sugarcane cutters during the harvest season, researchers had to transport themselves and their equipment to the fields to assess workers before the work day begins, as early as three in the morning. Community-based studies required commuting to remote locations by sometimes impassable roads. Furthermore, researchers reported that homes rarely have addresses or internet accessibility, preventing mail or email contact with participants.
Working with communities Researchers described numerous complexities in engaging and studying Mesoamerican communities related to their social and political context. In El Salvador, where gang violence is a threat, researchers had to be accompanied by teams of armed policemen. Participants detailed how studies had gone awry because of gang influence, a phenomenon that prompted some investigators to seek permission from gang leaders for study staff to enter communities. In other areas, communities’ distrust of foreign researchers and health professionals was a significant barrier, which several international and expatriate researchers recognized. Some community members were wary of participating in CKDnt research because sugarcane workers who had done so before had been fired. More broadly, participants said that, although communities at the epicenters of the CKDnt epidemic understand the importance of etiological research in developing prevention strategies to address CKDnt, some had experienced substantial research fatigue.
Publishing According to participants, disseminating CKDnt research was also challenging. First, some researchers required language support to publish their findings in widely disseminated biomedical journals. Second, as one clinician discussed, publishing findings about CKDnt etiology was difficult if findings challenged current accepted knowledge in the field. Finally, a few participants discussed what may be the most dismaying of challenges: despite researchers’ ingenuity in the face of these complexities of CKDnt science, their studies may not be accepted for publication because they do not match methodologica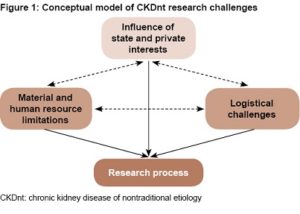 l standards that are expected in higher resource settings.
l standards that are expected in higher resource settings.
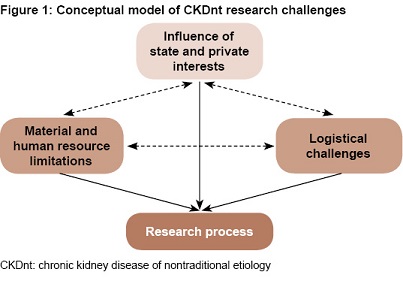
A proposed conceptual model of CKDnt research challenges Participants’ perceptions of factors influencing CKDnt research were used to develop a conceptual model of CKDnt research challenges (Figure 1). This model illustrates that the three classes of challenges described by researchers—state and private interests, material and human resource limitations, and logistical challenges—are distinct, but interrelated. For example, limited availability of high-quality laboratory resources and clinical equipment locally in Mesoamerica in turn creates logistical challenges for transporting samples abroad for maintenance and analysis. Similarly, attempts by the sugar industry to intimidate CKDnt researchers and limited access to sustainable, substantial funding have likely exacerbated the perceived shortage of researchers interested in carrying out CKDnt research. According to participants, these challenges affect CKDnt research at every stage, from obtaining funding to publication. Our proposed model accounts for both the interconnectedness of challenges facing CKDnt research and their influence on the overall research process.
DISCUSSION
In this qualitative study involving leading CKDnt researchers, participants described the CKDnt research process and environment. We found that numerous factors have hindered, delayed, threatened and complicated the CKDnt research process. Although many of these challenges, from the influence of private interests to resource limitations, have been explored in detail in other scientific arenas and resource-limited settings,[25–27] this study is the first to elucidate the complexities of carrying out CKDnt science in particular. It is also one of only three existing CKDnt studies that have employed qualitative methodology[10,28] and the first to examine CKDnt researchers’ perspectives.
Our participants described that although some sugar plantations in Mesoamerica are responding to concern about CKDnt, others—at least at the time these interviews were conducted—continued to stymie CKDnt research. Numerous examples exist of corporations (including in the tobacco, mining and sugar industries) making similar efforts to protect themselves from potentially damaging research in high-, middle- and low-income countries.[27,29,30]
The CKDnt research community has already made considerable progress toward establishing transparent, productive relationships with the sugar industry, focused on public health protection and scientific understanding of CKDnt. They have begun building networks among researchers, sugar plantations, affected workers, national governments and other key stakeholders, taking economic and political pressures felt by sugarcane plantations into account in workplace interventions and other studies, and collaborating with researchers who have experience studying industry-related health problems.[10,31–33] Participants also commented on the reactions of some government bodies to this issue, though largely from a regional stance. Despite participants’ comments about the intractability of some government bodies in some countries at the time these interviews were conducted, several publications have resulted from collaboration between national specialists and experts appointed by international cooperation institutions, as well as multiple meetings establishing CKDnt as a public health priority and specific governmental actions taken in response to the problem.[9,13,16,34–38] As policies, legislation and reforms that protect at-risk communities such as sugarcane workers are enacted, it will be important to ensure that plantations and local governments are implementing these new protections.
We also elucidated the difficulties of working in a resource-poor setting in which high-tech laboratories and substantial funding are scarce. A minority of international researchers additionally commented on the relatively limited availability of highly trained researchers and clinicians to study CKDnt in Mesoamerica, in comparison with the USA or Western Europe. Rather than being meant as a slight to the competence of national professionals, these opinions were expressed in the context of broader comments about the importance of national clinicians, researchers and public health workers in this field, as well as concerns about the impact of limited CKDnt funding on national and international researchers’ involvement.
There was no debate that national experts were among the first to draw attention to the epidemic, have made numerous significant contributions to our understanding of CKDnt epidemiology and etiology in Mesoamerica, and are essential to carrying out CKDnt research. Efforts to build nephrology workforce and research capacity, strengthen research networks that enable pooling of resources, expertise and data, and establish CKDnt research priorities are already under way.[8,9,39–41] However, research on other diseases of public health importance in low- and middle-income countries (LMIC), such as HIV/AIDS, has shown that some research “collaborations” can be exploitative of in-country researchers, resources and patient populations as well as insensitive to the nuances of carrying out research in that particular context.[42] Recognizing and emphasizing existing in-country expertise, including that of affected communities, will only become more important in the field of CKDnt as more researchers, funding and institutions from outside Mesoamerica mobilize to address this public health crisis.
We have found that carrying out CKDnt science presents significant challenges across study lifetimes. Together, these challenges make it difficult for CKDnt research that reaches the publication stage to meet methodological standards derived from and adjudicated in more generously resourced settings. This significant barrier to publication has been documented, yet there are no realistic, practical strategies to address it.[43] Expanding the role of scientists from these countries as editors and reviewers in high-impact scientific publications, offering journal-initiated mentorship to submitting authors, and addressing potential biases in review of manuscripts from LMICs would support researchers from resource-limited settings such as Mesoamerica in publishing their work, without negating other initiatives to improve research quality and methodological soundness.[44–46]
Limitations Several limitations should be considered concerning our findings. First, because we interviewed a purposive sample of leading researchers studying CKDnt in Central America and Mexico in particular, conclusions drawn here may not be generalizable to the entire population of CKDnt researchers or those studying CKDnt in other regions. Second, since this study involved one-time interviews, opinions and experiences communicated should be considered in the context of the timeframe during which interviews were conducted, May through September of 2015. Third, we analyzed what CKDnt researchers articulated in semistructured interviews, not direct observations. Fourth, we were unable to validate all reported concerns, given the sample size and subjective perspectives in this study. Finally, since this is the first study of its kind in the field of CKDnt research, these results should be viewed primarily as hypothesis generating.
CONCLUSIONS
Public health and biomedical research in low-resource, marginalized communities often present distinct complexities and pitfalls. These challenges are magnified when the public health problem under study is an etiologically novel non-communicable disease, as is the case with CKDnt. We have shown that these circumstances create a unique constellation of challenges to researchers attempting to address the CKDnt epidemic. Our findings identified important considerations for contextualizing progress in understanding CKDnt and underscored the need to enact and support efforts to facilitate CKDnt science and address the community-wide suffering it causes. Further studies reexamining CKDnt research challenges in other samples, time points and settings will help capture shifting and distinct factors not addressed in this single study. Finally, continued study of CKDnt’s biomedical and epidemiologic characteristics is essential. Scientific understanding of and consensus about these aspects of the epidemic will have important implications for what kinds of treatments and protections can be put into place and enforced for affected workers and their communities.
ACKNOWLEDGMENTS
Thanks to Professors Sherine Hamdy and Scott Frickel for their feedback on project design and coding of interview data, and for their comments on the manuscript; also to Drs Lara Traeger and Nwamaka Eneanya for feedback on the manuscript. This work was supported by a Royce Fellowship from Brown University’s Swearer Center for Public Service.
References

- Ramírez-Rubio O, McClean MD, Amador JJ, Brooks DR. An epidemic of chronic kidney disease in Central America: an overview. J Epidemiol Community Health. 2013 Jan;67(1):1–3.
- Jayasumana C, Orantes C, Herrera R, Almaguer M, López L, Silva LC, et al. Chronic interstitial nephritis in agricultural communities: a worldwide epidemic with social, occupational and environmental determinants. Nephrol Dial Transplant. 2017 Feb;32(2):234–41.
- Correa-Rotter R, Wesseling C, Johnson RJ. CKD of unknown origin in Central America: the case for a Mesoamerican nephropathy. Am J Kidney Dis. 2014 Mar;63(3):506–20.
- Brooks DR, Ramírez-Rubio O, Amador JJ. CKD in Central America: a hot issue. Am J Kidney Dis. 2012 Apr;59(4):481–4.
- Nanayakkara S, Komiya T, Ratnatunga N, Senevirathna ST, Harada KH, Hitomi T, et al. Tubulointerstitial damage as the major pathological lesion in endemic chronic kidney disease among farmers in North Central Province of Sri Lanka. Environ Health Prev Med. 2012 May;17(3):213–21.
- Rajapurkar MM, John GT, Kirpalani AL, Abraham G, Agarwal SK, Almeida AF, et al. What do we know about chronic kidney disease in India: first report of the Indian CKD registry. BMC Nephrol. 2012 Mar 6;13:10.
- Trabanino RG, Aguilar R, Silva CR, Mercado MO, Merino RL. Nefropatía terminal en pacientes de un hospital de referencia en El Salvador. Rev Panam Salud Pública. 2002 Sep;12(3):202–6. Spanish.
- Wesseling C, Crowe J, Hogstedt C, Jakobsson K, Lucas R, Wegman D, editors. Mesoamerican Nephropathy: Report from the First International Research Workshop on MeN. First International Research Workshop on Mesoamerican Nephropathy; 2012 Nov 28–30; San Jose, Costa Rica. Heredia (CR): Program on Work, Environment, and Health in Central America; 2013. 240 p.
- Pan American Health Organization. Chronic Kidney Disease in Agricultural Communities in Central America. 152nd Session of the Executive Committee. Washington, D.C.: Pan American Health Organization; World Health Organization; 2013 Jun. 12 p.
- Bodin T, García-Trabanino R, Weiss I, Jarquín E, Glaser J, Jakobsson K, et al. Intervention to reduce heat stress and improve efficiency among sugarcane workers in El Salvador: Phase 1. Occup Environ Med. 2016 Jun;73(6):409–16.
- Bolaños J. Nicaragua. Sugar Annual. Nicaragua: Sugar production down 4 percent [Internet]. Washington, D.C.: United States Department of Agriculture Foreign Agricultural Service; 2016 Apr 20 [cited 2017 Jul 15]. 5 p. Available from: https://gain.fas.usda.gov/Recent%20GAIN%20Publications/Sugar%20Annual_Managua_Nicaragua_4-20-2016.pdf
- Hutchinson Y. Sickly Sweet: Human Rights Conditions for Sugarcane Workers in Western Nicaragua [Internet]. León (NI): La Isla Foundation; 2014 Aug [cited 2017 Apr 30]. 73 p. Available from: http://laislanetwork.org/wp-content/uploads/2014/08/Sickly-Sweet-InDesign.pdf?7a2409
- Rodríguez MI. Chronic Kidney Disease in Our Farming Communities: Implications of an Epidemic. MEDICC Rev. 2014 Apr;16(2):77–8.
- Wesseling C, Aragón A, González M, Weiss I, Glaser J, Bobadilla NA, et al. Kidney function in sugarcane cutters in Nicaragua – A longitudinal study of workers at risk of Mesoamerican nephropathy. Environ Res. 2016 May;147:125–32.
- Roncal Jiménez CA, Ishimoto T, Lanaspa MA, Rivard CJ, Nakagawa T, Ejaz AA, et al. Fructokinase activity mediates dehydration-induced renal injury. Kidney Int. 2014 Aug;86(2):294–302.
- Orantes CM, Herrera R, Almaguer M, Brizuela EG, Núñez L, Alvarado NP, et al. Epidemiology of Chronic Kidney Disease in Adults of Salvadoran Agricultural Communities. MEDICC Rev. 2014 Apr;16(2):23–30.
- Raines N, González M, Wyatt C, Kurzrok M, Pool C, Lemma T, et al. Risk Factors for Reduced Glomerular Filtration Rate in a Nicaraguan Community Affected by Mesoamerican Nephropathy. MEDICC Rev. 2014 Apr;16(2):16–22.
- Murray KO, Fischer RS, Chavarria D, Duttmann C, García MN, Gorchakov R, et al. Mesoamerican nephropathy: a neglected tropical disease with an infectious etiology? Microbes Infect. 2015 Oct;17(10):671–5.
- McClean M, Amador JJ, Laws R, Kaufman JS, Weiner DE, Sánchez Rodríguez JM, et al. Investigating biomarkers of kidney injury and chronic kidney disease among workers in Western Nicaragua [Internet]. Massachusetts: Boston School of Public Health; 2012 Apr 26 [cited 2017 Apr 30]. 52 p. Available from: http://www.cao-ombudsman.org/documents/Biological_Sampling_Report_ April_2012.pdf
- Obrador GT, Rubilar X, Agazzi E, Estefan J. The Challenge of Providing Renal Replacement Therapy in Developing Countries: The Latin American Perspective. Am J Kidney Dis. 2016 Mar;67(3):499–506.
- Silva LC, Ordúñez P. Chronic Kidney Disease in Central American Agricultural Communities: Challenges for Epidemiology and Public Health. MEDICC Rev. 2014 Apr;16(2):66–71.
- Glaser J, Weiss I; La Isla Foundation. CKDu: strategies for saving lives now. MEDICC Rev. 2014 Apr;16(2):81–2.
- Murphy H. Deadly Illness in Nicaragua Baffles Experts. New York Times [Internet]. 2014 May 8 [cited 2017 Nov 13]; [about 6 screens]. Available from: https://www.nytimes.com/2014/05/09/world/americas/deadly-illness-in-nicaragua-baffles-experts.html
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nursing. 2008 Apr;62(1):107–15.
- Brown P, Morello-Frosch R, Zavestoski S; Contested Illness Research Group. Contested Illnesses: Citizens, Science, and Health Social Movements. Los Angeles: University of California Press; 2012. 324 p.
- Livingston J. Improvising Medicine: An African Oncology Ward in an Emerging Cancer Epidemic. Durham (NC): Duke University Press; 2012. 228 p.
- Brandt AM. Inventing conflicts of interest: a history of tobacco industry tactics. Am J Public Health. 2012 Jan;102(1):63–71.
- Ramírez-Rubio O, Brooks DR, Amador JJ, Kaufman JS, Weiner DE, Scammell MK. Chronic kidney disease in Nicaragua: a qualitative analysis of semi-structured interviews with physicians and pharmacists. BMC Public Health. 2013 Apr 16;13:350.
- Kirsch S. Mining capitalism: The relationship between corporations and their critics. Oakland: University of California Press; 2014. 314 p.
- Kearns CE, Glantz SA, Schmidt LA. Sugar Industry Influence on the Scientific Agenda of the National Institute of Dental Research’s 1971 National Caries Program: a historical analysis of internal documents. PLoS Med. 2015 Mar;12(3):e1001798.
- About the WE Program [Internet]. León (NI): La Isla Network; c2017 [cited 2017 Apr 30]. Available from: http://weprogram.org/about/
- Wegman D, Crowe J, Hogstedt C, Jakobsson K, Wesseling C, editors. Mesoamerican Nephropathy: Report from the Second International Research Workshop on MeN. Second International Research Workshop on Mesoamerican Nephropathy; 2015 Nov 18–20; San Jose, Costa Rica. Heredia (CR): Program on Work, Environment, and Health in Central America; 2016. 200 p.
- Wesseling C, Aragón A, Elgstrand K, Flores R, Hogstedt C, Partanen T. SALTRA: a regional program for workers’ health and sustainable development in Central America. Int J Occup Environ Health. 2011 Jul–Sep;17(3):223–9.
- Ordúñez P, Nieto FJ, Martínez R, Soliz P, Giraldo GP, Mott SA, et al. Chronic kidney disease mortality trends in selected Central America countries, 1997–2013: clues to an epidemic of chronic interstitial nephritis of agricultural communities. J Epidemiol Community Health. 2018 Apr;72(4):280–6.
- Lozier M, Turcios-Ruiz RM, Noonan G, Ordúñez P. Chronic kidney disease of nontraditional etiology in Central America: a provisional epidemiologic case definition for surveillance and epidemiologic studies. Rev Panam Salud Pública. 2016 Nov;40(5):294–300.
- Consejo de Ministros de Salud de Centroamérica y República Dominicana. Resolución de la XXXC Reunión del Consejo de Ministros de Salud de Centroamérica y República Dominicana (COMISCA); 2011 1–2 Dec; San Salvador, El Salvador [Internet]. San Salvador (SV): Ministry of Health of El Salvador; 2011 Dec 2 [cited 2018 Mar 5]. 13 p. Available from: http://www.sica.int/busqueda/busqueda_basica.aspx?IdCat=26&IdMod=3&IdEnt=143. Spanish.
- Chavkin S. Reform in Costa Rica signals new strategy against lethal epidemic [Internet]. Washington, D.C.: The Center for Public Integrity; 2015 Jul 29 [cited 2018 Mar 5]; [about 4 screens]. Available from: https://www.publicintegrity.org/2015/07/29/17716/reform-costa-rica-signals
-new-strategy-against-lethal-epidemic
- Ministerio de Medio Ambiente y Recursos Naturales (MARN) [Internet]. San Salvador (SV): MARN; c2018. Noticias. Diputados aprobaron dictamen que prohíbe el uso de 53 agroquímicos; 2013 Sep 6 [cited 2018 Mar 5]; [about 1 screen]. Available from: http://www.marn.gob.sv/diputados-aprobaron-dictamen-que-prohibe-el-uso-de-53-agroquimicos/. Spanish.
- Dirks JH, Robinson SW. The global perspective of the International Society of Nephrology: A decade of experience with COMGAN. Kidney Int. 2005 Oct;68(4):1395–410.
- Caplin B, Jakobsson K, Glaser J, Nitsch D, Jha V, Singh A, et al. Epidemiology of eGFR in Low and Middle Income Populations – Rationale and core protocol for the Disadvantaged Populations eGFR Epidemiology Study (DEGREE). BMC Nephrol. 2017 Jan 3;18(1):1.
- Wesseling C, Crowe J, Hogstedt C, Jakobsson K, Lucas R, Wegman DH. The Epidemic of Chronic Kidney Disease of Unknown Etiology in Mesoamerica: A Call for Interdisciplinary Research and Action. Am J Public Health. 2013 Nov;103(11):1927–30.
- Crane JT. Scrambling for Africa: AIDS, Expertise, and the Rise of American Global Health Science. New York: Cornell University Press; 2013 Sep 24. 224 p.
- Weisinger JR, Bellorin-Font E. Latin American nephrology: Scientific production and impact of the publications. Kidney Int.1999 Oct;56(4):1584–90.
- Balster RL. Expanding the role of scientists from low and middle income countries in the journal publication process. Drug Alcohol Depend. 2006 May;82(3):185–6.
- Northridge ME, Holtzman D, Bergeron CD, Zambrana RE, Greenberg MR. Mentoring for publication in the American Journal of Public Health. Am J Public Health. 2015 Mar;105(Suppl 1):S14–6.
- Harris M, Macinko J, Jiménez G, Mahfoud M, Anderson C. Does a research article’s country of origin affect perception of its quality and relevance? A national trial of US public health researchers. BMJ Open. 2015 Dec 30;5(12):e008993.
THE AUTHOR
Emily M. Wright (e.morgan.wright@gmail.com), doctoral student in the Population Health Sciences program at the Harvard Graduate School of Arts and Sciences. Clinical research coordinator, Massachusetts General Hospital, Boston, USA.
Submitted: October 27, 2017 Approved: May 07, 2018 Disclosures: None