INTRODUCTION
Arterial hypertension (HT) is the most prevalent non-communicable disease worldwide, long recognized as a major risk factor for cardiovascular and cerebrovascular disease.[1] It has been associated with a 62% risk of cerebrovascular disease, such as ischemic stroke, and 49% risk of cardiovascular disease.[2] A recent meta-analysis revealed that stroke risk increased with the severity of prehypertensive status.[3]
HT management includes assessment of target organ damage (i.e., heart, blood vessels, kidneys and brain), because multi-organ damage is associated with worse prognosis. But in practice, less than 15% of clinicians investigate brain damage caused by HT.[4]
The brain is an early target for organ damage due to HT.[1,5] Subclinical or “silent” vascular brain lesions are often detected by neuroimaging in asymptomatic patients. These can subsequently lead to cognitive decline, dementia or stroke.[6] Thus, early detection of such lesions could identify patients at higher risk for stroke, dementia and cardiovascular events, who could benefit from more aggressive preventive strategies.
Since HT is so common, clinicians look carefully for signs of organ involvement; a large body of evidence is now available on the crucial role of subclinical organ damage,[1,4,7] well established, for cardiovascular and renal diseases because the techniques applied are widely available. In contrast, detection of early brain deterioration requires imaging techniques too scarce and costly for routine use in general practice.
The challenge is to detect asymptomatic brain lesions early with cost-effective techniques for mass population screening. This article reviews the current status of biomarkers for early detection of brain damage in HT, with emphasis on use of blood-based biomarkers, presenting as well our experience and thinking on serum biochemical markers of brain injury.
Our objective was to review the various biomarkers used for early detection of brain damage in HT, and to assess their usefulness and feasibility of routine use. In particular, blood-based biomarkers were explored due to their potential for providing a more accessible, rapid and less expensive solution, requiring minimal expertise to interpret.
EVIDENCE ACQUISITION
Studies were identified through PubMed, SciELO and Cochrane databases through March 30, 2015 using the following search terms: hypertension AND brain damage AND biomarkers, without language restrictions. Published studies that evaluated subclinical brain damage in patients with HT employing different biomarkers (brain imaging, ambulatory blood pressure monitoring, quantitative retinal microvascular assessment, quantitative electroencephalography, carotid ultrasonography, neurocognitive studies and blood-based biomarkers) were included.
Because subclinical white matter lesions (WML) have other risk factors besides HT (age, diabetes mellitus and others),[6] we also included studies of age and diabetes mellitus, and community-based studies of associations between asymptomatic WML and blood-based biomarkers. References in retrieved articles were also reviewed to search for additional pertinent sources.
RESULTS
Hypertension and subclinical brain damage HT can surreptitiously damage the body for years before symptoms deve-lop, through an event cascade that thickens and stiffens artery walls throughout the body, blocking blood flow to the heart, kidneys, brain and limbs. This silent and progressive damage over decades subsequently leads to peripheral artery disease and/or damage to heart, kidneys and brain.[8,9]
Continuous blood pressure changes in the brain cause vascular remodeling, hemodynamic alterations, increased vascular resistance and endothelial dysfunction, all related to tissue damage, revealed as silent lacunar infarcts, microbleeds and white matter changes. Chronic ischemia or acute disruption of blood supply to brain tissue can further trigger mild cognitive impairment, dementia, transient ischemic attacks or stroke.[10,11]
A population study of 3600 participants (free of stroke or transient ischemic attack, mean age 65 years) using MRI found only 4.4% free of any white matter abnormalities. That is, the vast majority of the population had degenerative changes, which were associated with impaired cognitive and lower extremity function.[12]
Silent cerebral WML are frequently found on brain MRI in older adults. However, they tend to occur earlier and appear to be more severe in patients with HT.[13] In the Atherosclerosis Risk In Communities Study (ARIC) of 1920 persons aged 55–72 years, without history of stroke or transient ischemic attack, the prevalence of MRI-defined WML was 85%, associated with HT duration, treatment and control.[14] In the Cardiovascular Health Study, WML prevalence was 87% in HT patients.[15] Lower WML prevalence has been reported by van Boxtel in 65% of HT patients with a mean age of 57.4 years,[16] and Henskens in 44% of a younger cohort (mean age 51.6 years).[7] In one Cuban study of HT patients with a mean age of 44.2 years, classical silent brain lesions were detected in 40%;[17] while our group reported silent WML in 73.9% of an older cohort (mean age 59 years) of essential HT patients,[18] and more recently, classical silent MRI-detected brain lesions in 70.6% of essential HT patients.[19] In sum, WML frequency in reases with age.
Van Dijk demonstrated that systolic and diastolic blood pressure were positively associated with WML progression, in patients aged 60–90 years, new lesions occurring in up to 40% of patients.[20] This effect on brain lesion progression was stronger in younger patients and remained after adjusting for use of antihypertensive medications.[20] Gottesman found a similar pattern for midlife patients.[21]
While the entire vasculature is affected by HT, its particular effects on small vessels are key in the severity of damage to cerebral structures.[8,13] Perforating vessels—which originate in the cortical and leptomeningeal arteries—have a relatively poor anastomotic system, making white matter particularly vulnerable to blood pressure changes, so both low and high blood pressure have been reported as WML risk factors.[8]
Sierra hypothesized that long-standing HT causes lipohyalinosis of the media and thickening of vessel walls, with luminal narrowing of the small perforating arteries and arterioles that nourish the deep white matter, developing the changes that lead to WML.[22]
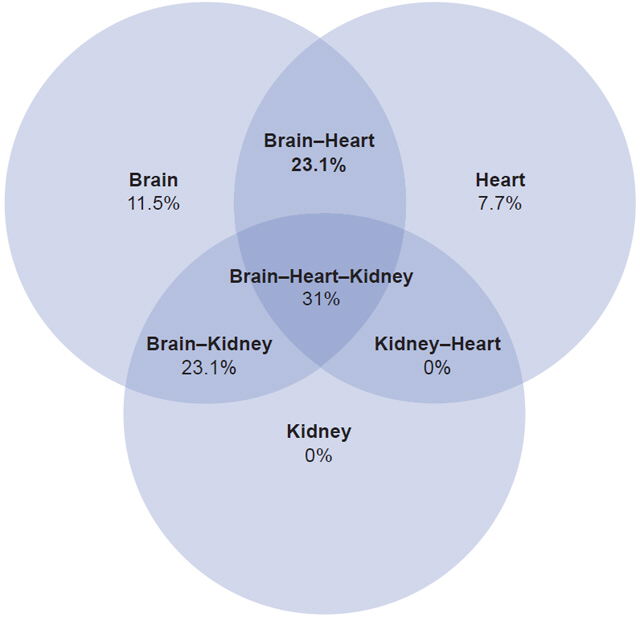
Figure 1: Target organ damage detected in 34 asymptomatic HT patients

Source: González-García,[19] used under terms of Creative Commons Attribution
4.0 license
HT: hypertension
WML are also related to mild cognitive impairment in cognitively intact older adults.[23] In HT patients aged 40–88 years, prevalence of silent brain infarcts ranges from 20%–86% and is related to stroke and cognitive decline.[20] The multiethnic Northern Manhattan Study (NOMAS) examined a clinically stroke-free population and found 17.7% had subclinical brain infarcts, prevalence increasing with age.[24] Both subclinical infarcts and white matter hyperintensity volume were associated with a globally worse cognitive performance.[25] Delgado recently reported a 10.1% prevalence of silent brain infarcts in a cohort of 976 essential hypertensive patients aged 50–70 years.[26] The high prevalence of silent brain infarcts in the population and their clinical consequences led the American Heart Association to include them in their 2013 updated stroke definition.[27]
Research on the third generation of the Framingham Heart Study found accelerated brain aging in HT and prehypertensive individuals in their 40s, including damage to the structural integrity of the brain’s white and gray matter. They concluded that subtle vascular brain injury caused by raised blood pressure develops gradually, with noticeable effects even in young adults. Their findings also revealed significant brain-cell damage in people with HT decades prior to the appearance of dementia symptoms,[2] emphasizing the need for early and optimal blood pressure control.
The foregoing supports the contention that brain damage in the form of WML and silent brain infarcts can be present in asymptomatic HT patients,[1,7] highlighting the importance of assessing subclinical brain injury in HT patients, especially those with cognitive changes.
Assessment of subclinical brain injury in HT patients The gold standard for assessing early brain damage in HT is brain MRI, although positron emission tomography (PET) has also been employed.[7,28] Recent advances in MRI methods using contrast agents provide additional opportunities to measure events in the cerebral vasculature, such as blood–brain barrier rupture, leukocyte infiltration, cell adhesion, molecule upregulation and vascular remodeling.[29]
While assessment of HT’s cardiorenal effects has been routine clinical practice for years, not so for HT neurological damage due to limited availability of MRI and cost considerations. Thus, alternative methods for demonstrating asymptomatic neurological damage by HT are needed.
Other more accessible and less expensive techniques to assess risk of subclinical brain damage have been proposed, such as ambulatory blood pressure monitoring,[16,24] quantitative retinal microvascular assessment,[30,31] quantitative electroencephalography,[17,32] carotid ultrasonography[19] and neurocognitive studies.[9]
Ambulatory blood pressure monitoring Twenty-four hour ambulatory blood pressure monitoring (ABPM) has become an important tool for improving HT diagnosis and management. Several studies have demonstrated an association between 24-h ABPM results and white matter hyperintensities in HT patients.[16,22,33,34] However most of these studies have been cross-sectional, so any conclusions about the direction of the relationship between ABPM and WML remain speculative. Longitudinal studies are required to establish causality.
Steady and pulsatile components of daytime, nighttime and 24-h blood pressure have gained increased interest in the prediction of WML, lacunar infarctions and stroke. Van Boxtel reported no association between nighttime dipping of blood pressure and white matter hyperintensity load, whereas daytime and 24-h pulse pressure averages were associated with paraventricular WML, and systolic blood pressure and mean arterial pressure for all periods were higher in patients with lacunar infarctions. He concluded that there was no relationship between diurnal blood pressure rhythm and signs of structural or functional cerebral damage in a population of newly diagnosed HT individuals, but that ABPM profiles may predict lesion type in early asymptomatic cerebral abnormalities.[16]
It remains unknown whether and to what extent ABPM could prove useful for detecting subclinical central nervous system damage in HT patients. Notwithstanding, in 2014 Avet’s PROOF study of 830 individuals aged 65±1 years found relationships between total WML score and 24-hour systolic blood pressure, 24-hour diastolic blood pressure, daytime systolic and diastolic blood pressure, and nighttime systolic blood pressure; WML score was not associated with nocturnal blood pressure dip, nor with other recognized cardiovascular risk factors. They identified a mean 24-hour systolic blood pressure threshold of 123 mmHg for identifying patients at high-risk for WML.[34]
Quantitative retinal microvascular assessment The retina offers a unique, noninvasive and easily accessible window to study the microvascular etiology of cerebrovascular disease. HT retinal changes defined qualitatively from a fundus examination have been traditionally classified into four grades of retinopathy;[35] nevertheless, most HT patients today are diagnosed early in the process of their illness, and hemorrhages and exudates (grade 3) and papilledema (grade 4), are observed very rarely. Milder degrees of retinopathy appear to be largely nonspecific arteriolar alterations (grades 1 and 2) and their usefulness for prognosis has been questioned.[5]
Thus, more selective methods for objectively investigating ocular HT damage have been developed and studied. Digitized retinal photography has been used to quantify the geometric and topological properties of arteriolar and venous trees, demonstrating that retinal arteriolar and venous narrowing may precede HT development.[31]
Cheung developed new quantitative and qualitative parameters to describe retinal branching patterns and improve sensitivity and specificity in detecting retinal microcirculatory alterations. This approach provided interesting data on quantitative and qualitative assessment of retinal microvascular abnormalities in a general population and their relationships with blood pressure values.[30] Scuteri related presence of WMLs not only to elevated brachial systolic blood pressure, pulse pressure and arterial stiffness, but also to retinal arterial narrowing.[9]
Retinal microvascular flow is known to be reduced in persons with WML and lacunar infarction. In a cohort of 1684 asymptomatic individuals aged 51–72 years from the ARIC study, those with WML were more likely to have retinal microvascular abnormalities and at greater long-term risk of subclinical cerebrovascular disease on MRI, independent of conventional risk factors. The ARIC authors suggested that retinal microvascular abnormalities are early and possibly more sensitive markers of subclinical cerebral small vessel disease than imaging techniques.[36]
Although quantitative retinal microvascular assessment seems promising as a biomarker for predicting early brain damage in HT patients, one obstacle to its translation to routine clinical practice is the need for accurate documentation and measurement of retinal arteriolar narrowing, which requires highly specialized and automated equipment not yet commonly available in primary care settings.
Quantitative electroencephalography Another line of investigation has been brain electrical activity in HT. A study in neurologically asymptomatic subjects with essential HT found that quantitative EEG revealed altered spontaneous brain activity, mainly in the frontal and midline regions of the left hemisphere, which the authors interpreted as due to brain hypoperfusion.[32] The same researchers later used low-resolution electromagnetic tomography to investigate abnormal electrical activity in 84 hypertensive patients with no history of neurological disease.[37] They found that the electrical sources were located mainly in right Brodmann areas 17 and 37, and left Brodmann areas 6, 10 and 39, regions that are very sensitive to hypoperfusion secondary to HT. Although these studies revealed impairment of brain electrical activity in neurologically asymptomatic HT patients, neither associated quantitative EEG findings with brain MRI lesions.[32,37]
Hernández assessed the diagnostic accuracy of a broad battery of tests for predicting subclinical brain MRI lesions in a pilot study of 50 HT patients with no known neurological disease (excluded from the Cuban Human Brain Mapping Project solely because of HT), and noted that quantitative EEG predicted more severe MRI lesions, with almost 91% diagnostic accuracy.[17] Brown assessed the results of conventional EEG in the same patients, quantifying observations from visual inspection employing the grand total EEG scale, and found an association between severity of EEG changes and brain MRI lesions.[38]
Carotid ultrasonography There are very few studies correlating structural and hemodynamic carotid ultrasound parameters with extent of brain MRI lesions in asymptomatic HT patients, and the results are controversial.The most frequently examined variable in extracranial ultrasound has been intima–media thickness, which was found increased in association with brain MRI lesions.[17,39] In a cohort of 1684 asymptomatic persons aged 51–72 years from the ARIC study, individuals with WML had increased carotid intima–media thickness.[36] However, Heliopoulos found no such association in a sample of 52 HT patients (mean age 71.4 years).[40] Arterial stiffness has also been associated with microvascular brain damage.[9] Maillard found systolic blood pressure linearly associated with markers of cerebral white matter microstructural damage in young adults.[2] In turn, high systolic pressure has been considered to be a result of accelerated arterial aging or increased stiffness.[41] Our group recently reported increased resistive index and decreased diastolic velocity in essential HT patients with classical brain MRI lesions, possibly indicating a resistive carotid flow pattern in these patients.[19]
Neuropsychological assessment Neuropsychological methods have demonstrated impairment in HT patients in different cognitive domains (attention, memory, executive function), predominantly affecting executive function, with slower information processing, impaired ability to shift from one task to another, and deficits in working memory (ability to hold and manipulate information).[9] It has been suggested that increased blood pressure may explain HT individuals’ deterioration in cognitive functions through small vessel disease, white-matter lesions and endothelial dysfunction.[20] Van Boxtel found an association between presence of WML and poor performance on neuropsychological tests in asymptomatic, never-treated essential HT patients.[16]
There is accumulating evidence that the negative effect of elevated blood pressure on cognitive aging is probably mainly mediated by WMLs. Increased WML volume has been associated with decreased episodic memory and executive function, the association stronger for evolution of existing WMLs than for occurrence of new ones.[42]
Cognitive tests may help detect initial brain deterioration in HT patients, but widespread application is challenging because these are time consuming and require a high degree of skill to interpret.
Blood-based biomarkers Blood withdrawal is a very simple and common procedure for assessing numerous cellular and biochemical parameters in medical conditions. Some of these have been explored in connection with subclinical brain damage in asymptomatic individuals. WML and silent cerebral infarcts are the MRI imaging expression of cerebral small vessel disease, whose main risk factor is arterial HT, but also includes others such as age and diabetes mellitus.[6] Mechanisms leading to development of subclinical WML may be different, but the ultimate lesions probably share common molecular indicators of injury in the bloodstream. Thus we consider that information about blood biomarkers of asymptomatic brain damage in individuals with other predisposing conditions may also be of value to appraise changes observed in arterial HT.
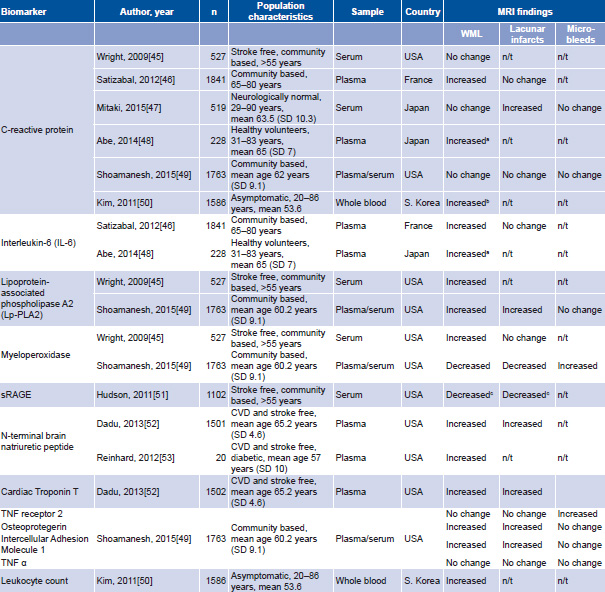
Low-grade systemic inflammation participates in the pathophysiology of HT, and C-reactive protein (CRP)—possibly the most studied blood marker for HT-related inflammation—has been associated with greater risk and severity of stroke in healthy populations[43] and among hypertensive men.[44] Nevertheless, evidence relating inflammatory markers and brain damage is controversial. Table 1 summarizes results reported for association of several blood biomarkers with presence of brain MRI lesions in neurologically asymptomatic individuals. Elevations of the inflammatory markers lipoprotein-associated phospholipase A2 and myeloperoxidase, but not CRP, were found to be associated with a greater burden of WML.[45] Satizabal studied an elderly community-based sample and reported an association between circulating interleukin-6 (IL-6) and CRP levels and more severe WML, but not with lacunar infarcts,[46] while Mitaki revealed opposing results with CRP: an association with silent lacunar infarcts, but not with WML or with cerebral microbleeds.[47] On the other hand, high levels of IL-6 and CRP were reported as useful biomarkers for identifying high risk for periventricular hyperintensities in healthy Japanese subjects.[48]
Shoamanesh’s study of a middle-aged, community-based sample (n = 1763) is perhaps one of the most extensive concerning the possible role of inflammation in pathogenesis of cerebral small vessel disease.[49] It assessed the association of a comprehensive panel of 15 systemic inflammatory markers with MRI measures of cerebral small vessel disease. Increased levels of tumor necrosis factor (TNF) receptor 2 and myeloperoxidase were associated with cerebral microbleeds, but not with WML or lacunar infarcts, while higher levels of osteoprotegerin, intercellular adhesion molecule 1 and lipoprotein-associated phospholipase A2, as well as lower myeloperoxidase, were observed in participants with greater WML volumes and silent cerebral infarcts. No associations were encountered between cerebral microbleeds and osteoprotegerin, intercellular adhesion molecule 1 and lipoprotein-associated phospholipase A2; no changes in CRP or TNF alpha levels accompanied brain MRI lesions.
Kim used leukocyte count as a marker of systemic inflammation in his study of 1586 asymptomatic individuals who underwent brain MRI for a routine checkup. He found that elevated blood leukocyte count was associated with moderate to severe WML, independently of known cardiovascular risk factors such as age, HT and diabetes.[50] Additionally, these authors found higher CRP levels related to moderate to severe WML, but this association disappeared after adjustment for leukocyte count, age, and other clinical and demographic variables.
In NOMAS, lower serum levels of soluble receptors for advanced glycation end-products (sRAGE) were associated with higher prevalence of silent brain infarcts and WML in stroke-free Hispanic and black subjects in the USA, respectively, suggesting that sRAGE may be predictive of subclinical cerebrovascular disease, particularly in ethnic/racial groups with increased risk for cerebrovascular disease.[51]
Some biomarkers for cardiovascular disorders have also been explored. Higher N-terminal brain natriuretic peptide and cardiac troponin T were associated with silent brain infarcts and WML, suggesting their usefulness for identifying individuals with subclinical cerebral injury.[52] In addition, a small cross-sectional study by Reinhard revealed that N-terminal brain natriuretic peptide was positively correlated with WML in diabetic patients.[53] Plasma markers of endothelial dysfunction such as intercellular adhesion molecule-1 and P-selectin have also been associated with WML.[54,55]
Table 1: Association of several blood-based biomarkers with brain MRI lesions in neurologically asymptomatic subjects

aonly for periventricular hyperintensity, not for deep-and-subcortical white matter hyperintensity
bin univariate analysis; association disappeared after adjustment for leukocyte count, age, sex, cardiovascular risk factors and aspirin use
conly in black patients for WML and Hispanic patients for silent brain infarcts
CVD: cardiovascular disease (coronary heart disease or heart failure) n/t: not tested TNF: tumor necrosis factor WML: white matter lesion
Blood biomarkers for systemic inflammation, endothelial dysfunction and oxidative stress have been explored in relation to subclinical brain damage in the general population, in hypertensive patients and those with diabetes mellitus, but biomarkers more specific to brain damage have been less thoroughly investigated. Abraham’s 2016 review of cardiovascular risk factors and small vessel brain disease, assessing studies associating nonglycemic blood biomarkers with WML, did not look at blood biomarkers specific to brain damage.[56]
Blood-based biomarkers specific to brain damage have been employed to assess degree of brain injury and as outcome predictors in different clinical contexts (stroke, traumatic brain injury and cardiac arrest, among others),[57–62] and also as end points for evaluating the effect of new therapies.[63] In general, notwithstanding the etiology of most brain lesions, at some point the blood–brain barrier becomes compromised, making it easier for cytosolic contents released from injured brain tissue to reach the blood. Among these biomarkers, brain-specific proteins (neuronal or glial in origin) have received growing attention in clinical neurological research: neuron-specific enolase (NSE), a cytosolic neuronal protein;[57,59] S100B calcium-binding protein and glial fibrillary acidic protein (GFAP), both glial-derived proteins.[59–61] Also autoantibodies to brain-specific proteins have been the object of growing interest.[64] Studies employing autoantibodies to NR1[63] and NR2 peptides of NMDA receptors[65–68] have shown promise as biomarkers of brain damage in ischemic stroke.
The idea of employing blood-based biomarkers of brain damage for predicting subclinical brain damage in HT is attractive and is supported by the previously mentioned findings clearly demonstrating subclinical brain lesions in neurologically asymptomatic HT patients. These chronically affected brain regions—mainly involving white matter—could be leaking brain-specific molecules into the blood stream at a rate much lower than in acute brain injuries (stroke, brain trauma, global ischemia due to cardiac arrest). Nevertheless, the possibility of detecting these brain-specific proteins in blood is undoubtedly increasing with the greater availability and sensitivity of current commercial kits. In this respect, measurement of autoantibodies to these proteins or their subunits is even more promising when dealing with chronically established brain lesions, as occurs with HT.[64–69]
Some studies have examined serum concentrations of brain-specific proteins in asymptomatic HT persons, but without looking for associations with subclinical brain MRI changes. Dambinova reported no changes in NR2A autoantibodies in a young cohort of 25 HT patients (mean age 36.9 years).[66] Schmidt provided preliminary evidence that increased S100B was associated with eclampsia, but not with preeclampsia or chronic HT in pregnant women (although these conditions are very dissimilar to essential HT), hypothesizing that increased S100B could be secondary to cerebral vascular changes leading to overperfusion, edema and ischemia, as well as to seizures themselves.[70] Al-Rawi measured salivary and serum levels of NSE in 25 HT patients, observing higher mean serum NSE levels in HT patients than in healthy controls, with values ranging between those obtained in ischemic stroke patients and healthy controls. Differences were not statistically significant,[71] possibly because of small sample size.
Gruden studied 72 healthy volunteers of both sexes and different ages and blood pressure levels, measuring S100B, the HLDF24 peptide fragment of leukemia differentiation factor (HLDF) and idiotypic autoantibodies to these proteins to determine their possible usefulness as biomarkers for HT risk. They found that serum concentrations of these molecular factors varied significantly by blood pressure level, even between those with optimal blood pressure and those whose blood pressure was merely “normal.” The authors concluded that variations in serum concentration of these factors and their antibodies could reliably predict HT risk in healthy adults.[69]
Our review yielded that the only attempt to predict silent brain damage in essential HT by measuring brain-specific proteins in serum was a pilot study conducted by our group, where NSE and S100B serum concentrations were assessed in 50 asymptomatic essential HT patients. Serum levels of NSE and S100B were increased in HT patients, but only NSE levels were associated with indicators of HT severity (high diastolic blood pressure and retinopathy grade). Brain MRI conducted in 23 patients showed an association of higher NSE levels with more severe WML.[18]Increasing the sample size to 101 HT patients (34 with brain MRI scans) produced similar findings. Thus, serum NSE levels could be useful in identifying HT patients with putative subclinical brain damage for subsequent brain MRI scanning. Longitudinal study of this cohort provided additional information suggesting that increased NSE could be a useful prognostic marker for central nervous system vascular events in asymptomatic HT patients.[72]
These results could constitute a baseline for future research on serum biomarkers for detection of subclinical brain damage in HT. Other molecules should be investigated, among which autoantibodies against NR1 or NR2 NMDA receptor peptides show promise, based on results obtained in studies of ischemic stroke.[65–68] These peptides also have the advantage of being very specific to the central nervous system, thus minimizing or eliminating the possibility of extracerebral sources.
Cuban experience According to Cuba’s 2012 Third National Survey on Risk Factors and Chronic Diseases, HT prevalence is 30.9% in the population aged ≥15 years. Treated HT patients comprise 89.2% of the total, but only 55.1% were reported as controlled.[73] Thus, essential HT and its target-organ sequelae constitute a major health problem in Cuba. Prevention is a fundamental principle of Cuba’s National Health System, so the 2008 Guidelines for Prevention, Diagnosis and Treatment of Arterial Hypertension emphasize not only HT prevention (the most important, universal and least expensive health intervention), but also preventing cardiovascular, cerebrovascular and renal diseases through identification of subclinical target organ damage.[74]
As we stated above, the frequency of subclinical brain damage in HT patients in the two Cuban research cohorts is comparable to that reported by other groups: 70.6% for a cohort with a mean age of 59 years[19] and 40% for a younger cohort (mean age: 44.2 years).[17] As in most countries, cardiorenal damage is routinely screened in HT patients, but low availability and high costs of brain MRI scanning preclude its use for early detection of asymptomatic brain lesions. Developing countries urgently need effective, less expensive and more accessible methods for widespread screening for subclinical brain damage, enabling most efficient use of scarce MRI resources.
Two Cuban research groups have focused on this goal. One group, at the Cuban Neuroscience Center, published the previously mentioned pilot study, reporting that quantitative EEG predicted subclinical brain damage on MRI much better than a battery of alternative tests (visual EEG, ABPM, fundoscopy and other clinical measures).[17] The results of another study involving the same patients (cited above) suggested that grand total EEG score could be used to screen for subclinical cerebrovascular lesions among HT patients, since it was associated with classical brain MRI lesions.[38]
The second research group, our own at the Cuban Neurology and Neurosurgery Institute, published a study in 50 patients with essential HT referred by family physicians for assessment of retinopathy.[18] Our main goal was to explore whether serum concentrations of brain-specific proteins (S100B and NSE) could predict subclinical brain MRI lesions. The results (summarized briefly above) indicated that higher serum NSE levels were useful predictors of more severe brain lesions in this group of patients. Similar results were observed when we later followed a larger cohort (101 HT patients) for an average of 33 months.[72] Our review did not find any earlier research[18] employing serum levels of brain-specific proteins to predict subclinical brain damage in HT patients. Finally, our group also reported a resistive carotid flow pattern in HTpatients with classical MRI lesions, characterized by increased resistive index and decreased diastolic velocity, suggesting the potential usefulness of carotid structure and hemodynamics as imaging biomarkers of subclinical brain lesions.[19]
CONCLUSIONS
Prediction of subclinical brain damage in HT patients and other risk conditions for cerebrovascular disease has been explored employing several biomarkers. To date, none of these has been introduced in general medical practice due mainly to prohibitive cost, and the need for specific technologies and highly specialized expertise. Although still infrequently assessed, blood-based biomarkers, especially brain-specific proteins, show promise as more accessible and less expensive tools to help stem the increased disease burden of stroke, cognitive decline and dementia. If proven effective, such biomarkers could have encouraging implications for resource-scarce settings, enabling countries such as Cuba to optimize use of MRI scanning.