INTRODUCTION Pediatric urinary lithiasis (urolithiasis) is an important health issue linked to urinary metabolic disorders. In the United States alone, annual costs associated with urolithiasis are $229 million for hospital admissions and $146 million for emergency care.
OBJECTIVE Identify urinary metabolic disorders in Cuban pediatric patients with urolithiasis and better understand the relationship of age, demographic and anthropometric variables to urinary metabolic disorders strongly associated with urolithiasis.
METHODS We carried out a descriptive, cross-sectional study. The study universe was comprised of Cuban patients aged 2 to 19 years with urinary lithiasis who underwent renal metabolic studies at the Dr Abelardo Buch López Nephrology Institute in Havana, Cuba, from 2008 through 2019. All data were obtained from reports of the aforementioned metabolic studies. We collected the following variables: age, sex, nutritional status, urinary volume, plasma and urinary creatine concentrations; and calcium, uric acid, oxalate and citrate urinary excretions collected during a 24-hour period. We included results of urinary cystine tests and urine mini-cultures. We obtained frequency distributions for categorical and qualitative variables and calculated means and standard deviations for quantitative variables. We also evaluated homogeneity of metabolic disorders between children and adolescents.
RESULTS We studied 1592 pediatric patients, of whom 67.7% (1078/1592) were adolescents. The main metabolic disorders included hypercalciuria (39.1%; 622/1592), decreased urinary flow (22.4%; 357/1592) and hypocitraturia (18.2%; 289/1592). Hypercalciuria, hypocitraturia and hyperoxaluria were more common in children, while decreased urinary flow and hyperuricosuria were more common in adolescents. Hyperuricosuria was more frequent in male patients (6.3%; 40/639 vs. 1.8%; 8/439) and had the greatest impact on lithogenesis. Hypercalciuria was more frequent in undernourished children (62.5%; 30/48) than in overweight children (21.7%; 10/46), or those with obesity (33.3%; 15/45).
CONCLUSIONS The main metabolic disorders among Cuban pediatric patients with urinary lithiasis are: hypercalciuria, decreased urinary flow and hypocitraturia. Hypercalciuria, hypocitraturia and hyperoxaluria are more common in children, and decreased urinary flow and hyperuricosuria are more common in adolescents. Identifying urinary metabolic disorders facilitates formulation of treatment plans tailored to decreasing the likelihood of urolithiasis.
KEYWORDS Pediatrics, urolithiasis, urinary lithiasis, hypercalciuria, urine, Cuba
ABSTRACT INTRODUCTION Pediatric urinary lithiasis (urolithiasis) is an important health issue linked to urinary metabolic disorders. In the United States alone, annual costs associated with urolithiasis are $229 million for hospital admissions and $146 million for emergency care.
OBJECTIVEIdentify urinary metabolic disorders in Cuban pediatric patients with urolithiasis and better understand the relationship of age, demographic and anthropometric variables to urinary metabolic disorders strongly associated with urolithiasis.
METHODSWe carried out a descriptive, cross-sectional study. The study universe was comprised of Cuban patients aged 2 to 19 years with urinary lithiasis who underwent renal metabolic studies at the Dr Abelardo Buch López Nephrology Institute in Havana, Cuba, from 2008 through 2019. All data were obtained from reports of the aforementioned metabolic studies. We collected the following variables: age, sex, nutritional status, urinary volume, plasma and urinary creatine concentrations; and calcium, uric acid, oxalate and citrate urinary excretions collected during a 24-hour period. We included results of urinary cystine tests and urine mini-cultures. We obtained frequency distributions for categorical and qualitative variables and calculated means and standard deviations for quantitative variables. We also evaluated homogeneity of metabolic disorders between children and adolescents.
RESULTSWe studied 1592 pediatric patients, of whom 67.7% (1078/1592) were adolescents. The main metabolic disorders included hypercalciuria (39.1%; 622/1592), decreased urinary flow (22.4%; 357/1592) and hypocitraturia (18.2%; 289/1592). Hypercalciuria, hypocitraturia and hyperoxaluria were more common in children, while decreased urinary flow and hyperuricosuria were more common in adolescents. Hyperuricosuria was more frequent in male patients (6.3%; 40/639 vs. 1.8%; 8/439) and had the greatest impact on lithogenesis. Hypercalciuria was more frequent in undernourished children (62.5%; 30/48) than in overweight children (21.7%; 10/46), or those with obesity (33.3%; 15/45).
CONCLUSIONSThe main metabolic disorders among Cuban pediatric patients with urinary lithiasis are: hypercalciuria, decreased urinary flow and hypocitraturia. Hypercalciuria, hypocitraturia and hyperoxaluria are more common in children, and decreased urinary flow and hyperuricosuria are more common in adolescents. Identifying urinary metabolic disorders facilitates formulation of treatment plans tailored to decreasing the likelihood of urolithiasis.
KEYWORDSPediatrics, urolithiasis, urinary lithiasis, hypercalciuria, urine, Cuba
INTRODUCTION Urinary lithiasis is an important health problem in the general population and, although its occurrence is comparatively rare in pediatric ages, evidence suggests that its incidence is increasing in this population.[1,2] Additionally, the disease is characterized by high recurrence rates that can require surgical intervention and is associated with high treatment costs and the risk of developing renal dysfunction requiring renal replacement therapy (dialysis or transplantation).[3] Added to these risks is the decrease in bone mineral density in patients who develop calcium stones, which increases the risk of fractures and can compromise patients’ quality of life.[4]
Although overall incidence of pediatric hospital admissions for urinary lithiasis in high-income countries is 1%–3%,[5] the USA has experienced an increase from 18.4 cases per 100,000 admissions in 1999 to 57 cases per 100,000 admissions in 2008, an adjusted annual increase of 10.6%.[1,5] Estimated recurrence rates in that country range from 16% to 67%,[6] and annual estimated costs for pediatric patients with urinary lithiasis are $229 million in hospital admissions and $146 million for emergency care.[7]
IMPORTANCE This study comprises the best evidence currently available in Cuba on urinary metabolic disorders predisposed to causing urolithiasis in children and adolescents, and offers insights for its primary and secondary prevention.
Development of urinary stones in children and adolescents is associated primarily with urinary metabolic disorders and urinary tract malformations.[8] Consequently, patients presenting with urolithiasis must be rigorously evaluated in order to identify underlying urinary metabolic disorders promoting lithogenesis, and treatments must be tailored to prevent recurrence.[8,9] Data are scarce on metabolic disorders in the Cuban and Latin American pediatric populations, making it difficult to implement strategies for primary and secondary prevention of urolithiasis.[9–11]
The objective of this study was to identify urinary metabolic disorders in the Cuban pediatric population with urolithiasis according to age, demographic and anthropometric variables, and the relation of these variables to disorders with the greatest lithogenic potential.
METHODS Design and participants We conducted a descriptive, cross-sectional observational study. The study universe consisted of all Cuban patients aged 2–19 years who presented with urinary lithiasis (demonstrated by imaging studies, or by spontaneous or instrumental elimination) who underwent renal metabolic studies at the Dr Abelardo Buch López Nephrology Institute in Havana, Cuba from January 2008 through December 2019.
Individuals who had suffered renal colic in the six weeks prior to recruitment or who had poorly collected samples were excluded from our research, as were pregnant individuals, foreign patients, vegetarians, amputees, those with chronic diarrhea or muscular dystrophies, or who were short for their age, according to Cuban height-for-age tables.[12] These patients were excluded because they presented with factors that could either interfere with the quality of the urine sample or could modify excretion of urinary solutes.
Variables Age (two groups: 2–9 years and 10–19 years); sex (female, male); nutritional status (undernourished, thin, normal weight, overweight, obese); urinary volume; plasma and urinary creatinine concentrations; urinary excretion of calcium, uric acid, oxalate and citrate over a 24-hour period; and the results of urinary cystine tests and urine mini-cultures.
Procedures We interviewed all patients (or patients’ caregivers, if patients were pre-verbal) to ensure that they did not meet any exclusion criteria. All medications were suspended for five days before the study. We collected 24-hour urine samples (in washed bottles with 5% thymol included as a preservative) and 5 mL fasting blood samples. Independent urine samples were used for the mini-cultures. We collected anthropometric data (height and weight), estimated the nutritional status of patients according to body mass index (BMI) in kg/m2, and classified patients according to the Cuban BMI-for-age tables.[13] Body surface area (BS) was calculated using the Dubois-Dubois formula.[14] A urine sample was considered ‘well-collected’ when creatinine excretion was less than ±1 standard deviation (SD) from the reference value according to the patient’s age, height and sex, as pathologies that may influence the generation and excretion of creatinine were exclusion criteria.[15]
Analytical determinations were made with a Microlab 300 spectrophotometer (Elitech Clinical Systems, Germany) in the case of urinary citrate and oxalate. For all other analyses, we used a HumaStar 80 spectrophotometric autoanalyzer (Human Diagnostics, Magdeburg, Germany). We followed manufacturer’s guides for both. Citrate and oxalate concentrations were determined via direct ferric cyanide/citrate reaction or formic acid/chromotrophic reaction methods, respectively. Creatinine was measured using the Jaffé kinetic method (alkaline picrate); uric acid using the enzymatic uricase/peroxidase method; and calcium using the calcium–arsenazo method. All reagents were provided by the Carlos J. Finlay Pharmaceutical Laboratory Company in Havana, Cuba. Urinary cystine tests were performed by reaction with sodium nitroprusside (Merck, Darmstadt, Germany). Urine mini-cultures were cultured in MacConkey’s Agar and CLED (cysteine lactose electrolyte deficient) Agar media (National Biopreparations Center, BIOCEN, Cuba).
Renal function was measured by creatinine clearance in mL/min/1.73m2 body surface (BS) and serum creatinine in mg/dL. Cystinuria and urinary tract infections were diagnosed by qualitative methods, the results used to classify patients as positive or negative.
Metabolic disorder diagnostic cut-off values Hypercalciuria Urinary calcium >4.0 mg or 0.10 mmol/kg/day Hyperuricosuria Uric acid >815 mg or 4.85 mmol/1.73 m2/ day Hyperoxaluria Urinary oxalate >45 mg or 0.5 mmol/1.73 m2/day Hypocitraturia Daily urinary citrate <365 mg or 1.90 mmol /1.73 m2 in males and <310 mg or 1.61 mmol/1.73 m2 in females Low urinary flow Urinary volume <20 mL/ kg /day[16]
Data collection and analysis We obtained information for the above selected variables from the first metabolic study conducted on each patient. All information was processed using the Statistical Package for Social Science (SPSS) version 22.0 for Windows (IBM, USA). We constructed frequency distributions for qualitative variables and calculated absolute frequencies and percentages. For quantitiative variables, we calculated means and standard deviations. The age distribution was divided into quartiles. In order to analyze associations between patient demographics and nutritional status, and metabolic disorders with the greatest lithogenic potential (hypercalciuria, hyperuicosuria, hyperoxaluria and hypocitraturia) we constructed double- and triple-entry contingency tables to provide a descriptive analysis of homogeneity.
Ethics This study was approved by the Scientific Council and the Research Ethics Committee of the Dr Abelardo Buch López Nephrology Institute. Confidentiality of all data obtained during the investigation was guaranteed.
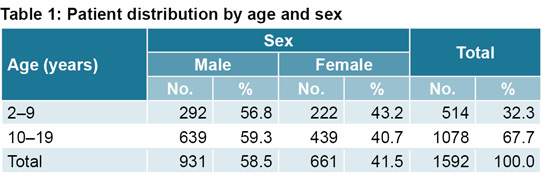
RESULTS We studied 1592 pediatric patients who presented with urolithiasis, 67.7% (1078/1592) were adolescents, aged 10–19 years. Children studied had an average age of 6.4 years (SD: 2.2 years) and adolescents, 13.9 years (SD: 2.6 years). There was a higher proportion of male patients, both in children (aged 2–9 years) and adolescents, at 56.8% (292/514) and 59.3% (639/1078), respectively (Table 1).
Children had a mean renal function of 104.5 mL/min/1.73 m2 BS (SD: 21.5); mean BMI of 16.2 kg/m2 (SD: 3.3) and mean body surface area of 0.87 m2 (SD: 0.22), while 321/514 (62.5%) of children were classified as normal weight; 10.5% (54/514) thin; 9.3% (48/514) undernourished; 8.9% (46/514) overweight; and 8.8% (45/514) obese.
Adolescents had a mean renal function of 105.7 mL/min/1.73 m2 BS (SD: 20.2); mean BMI of 19.4 kg/m2 (SD: 3.6) and mean body surface area of 1.43 m2 (SD: 0.26). Of the adolescents, 66.0% (712/1078) were of normal weight, 5.3% (57/1078) were classified as thin; 4.5% (49/1078) undernourished; 14.1% (152/1078) overweight and 10.0% (108/1078) obese.
The most frequent renal metabolic disorder was hypercalciuria (39.1%; 622/1592). This was followed in order of frequency by decreased urinary flow (22.4%; 357/1592) and hypocitraturia (18.2%; 289/1592). Other urinary metabolic disorders in the study had an overall frequency of <10%. Comparing children and adolescents, we found statistically significant differences in the relative frequencies of hypercalciuria, hypocitraturia and hyperoxaluria, which were higher in children; and also for decreased urinary flow and hyperuricosuria, which were more common in adolescents. Urinary tract infection was low in overall frequency and similar between the two groups (Table 2).
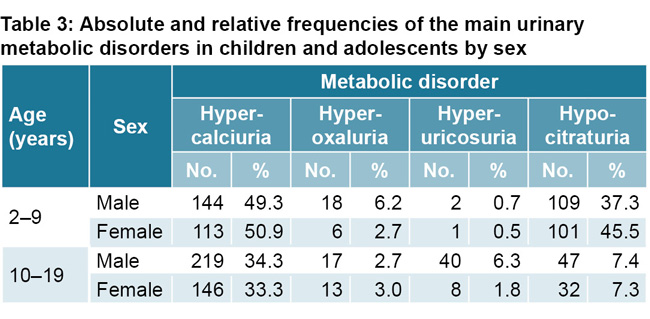
In terms of frequency of urinary metabolic disorders, it should be noted that we found minimal differences between the sexes in either children or adolescents. The greatest differences were found in hypocitraturia in children: 45.5% (101/222) in girls versus 37.3% (109/292) in boys, and in hyperuricosuria in adolescents; 1.8% (8/439) in female patients versus 6.3% (40/639) in male (Table 3).
There were notable differences in the frequencies of hypercalciuria and hypocitraturia in children and in the frequencies of hyperuricosuria and hypocitraturia in adolescents (Table 4).
Table 2, 3 y 4 and 5
In children, hypercalciuria appeared more often in children aged 5.0–6.9 years (59.3%, 83/140), while least often found in children aged 7.0–7.9 years (34.1%, 28/82). Hypocitraturia presented at higher rates in children at younger ages, which decreased as they grew older. In adolescents, frequency of hypocitraturia was higher in patients aged 10.0–11.9 years (15.3%, 37/242), compared with other age groups. Frequency of hyperuricosuria increased from 1.7% (4/242) in patients aged 10.0–11.9 years to 6.7% (20/299) in those aged 16.0–19.9 years.
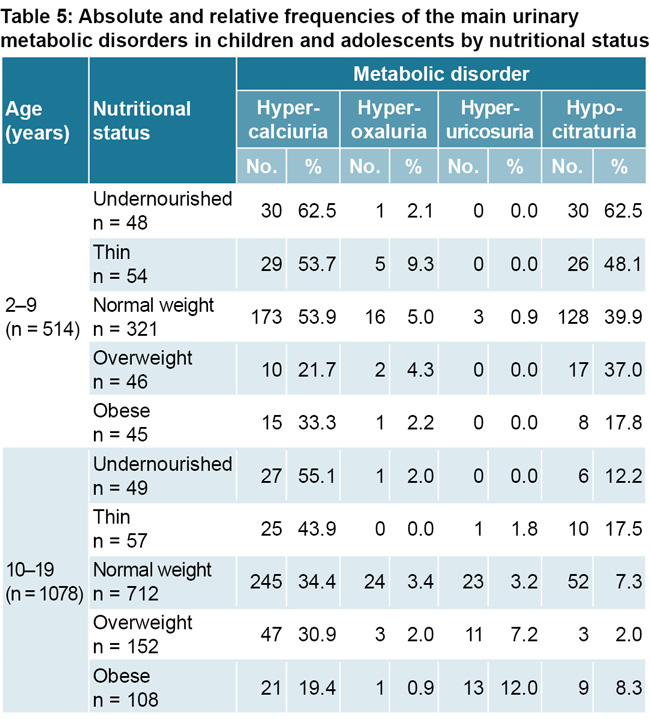
There were also appreciable differences for hypercalciuria and hypocitraturia in children, and for hypercalciuria, hyperuricosuria and hypocitraturia in adolescents when comparing disorder frequencies with groups according to patient nutritional status (Table 5). Frequencies of hypercalciuria and hypocitraturia were higher in undernourished children (62.5%; 30/48 for both disorders); frequencies of hypercalciuria were lower among overweight children (21.7%; 10/46) and cases of hypocitraturia were less frequent in obese children (17.8%; 8/45). Among adolescents, frequency of hypercalciuria and hypocitraturia were also high in undernourished patients, at 55.1% (27/49) and 12.2% (6/49) respectively. However, contrary to what we observed in children, frequency of hyperuricosuria was higher in obese adolescents (12.0%; 13/108) than in other weight categories.
DISCUSSION Although 24-hour urine composition tests are essential for diagnosing urinary metabolic disorders that promote lithogenesis and, consequently, for preventing lithogenesis recurrence, studies of this type in significant numbers of pediatric patients are rare on the global scale and nonexistent in Cuba. Additionally, urinary metabolic disorders are conditioned by dietary, genetic, water quality and climatic factors, among others, which does not allow data from other populations to be extrapolated to the Cuban population.[17]
The higher frequency of urolithiasis we found in the male sex coincides with results from both national and international epidemiological studies in adults.[18,19] However, the results in the pediatric population are less consistent.[20–22] Prevalence of lithiasis has also been described in adolescents,[23] and it is believed that the recent increase of the disorder in pediatric patients has occurred mainly within this age group. However, we can make no such assertions in the context of this study, since it was not conducted in an open population but only in urolithiastic patients who underwent urinary composition studies. It should also be noted that while urinary composition studies may have been conducted during adolescence, a first lithiastic episode could have happened during childhood. But to conduct such tests in children is difficult, as problems with 24-hour urine collection are more common in younger individuals.[24]
Worth noting is that approximately one fifth of the children in our study were in either the thin or undernourished categories. This may be due to the fact that several causes of lithiasis during childhood have an impact on nutritional status. One of the most important is renal tubular acidosis, whose incidence peaks during childhood and is a known cause of malnutrition in children. We were not able to explore this possible link since our research did not include urinary acidification studies.[25] It is also noteworthy that nearly a quarter of adolescents were either overweight or obese, both well-known risk factors for lithogenesis in adults and whose rates have increased in adolescent populations worldwide.[26]
Renal function was preserved in the vast majority of patients, to be expected given their young age, as the damage to renal function caused by stones in the urinary tract is cumulative, and often due to obstructive nephropathy. Another consideration is that urinary tract infections are often associated with lithiasis, which can contribute to impaired kidney function.[27] However, in this study, the frequency of urinary tract infections was low and similar between all groups.
In the absence of 24-hour urinary composition studies in healthy Cuban children, for this study we used internationally-accepted reference values in defining each disorder.[16] One problem with these definitions is that the risk of lithiasis increases with an increase in excretion or in concentration of the metabolite in question, which does not necessarily occur within a defined threshold, even when healthy individuals have been used to determine these thresholds.[20]
Frequencies of hypocitraturia and low urinary flow are higher in the pediatric populations with lithiasis than in the Cuban adult population with lithiasis. However, frequency of hyperuricosuria and urinary infections is higher in the adult population, consistent with findings in other studies.[8,28,29] Relative frequencies of urinary metabolic disorders in pediatric patients are similar to those found by Celiksoy in Turkey[30] and Amancio in Brazil.[10] Other studies, including Yang in China,[31] and Akhavan in Iran,[32] found hypocitraturia to be the most common disorder. These differences may be due to dietary habits or genetics.
Unfortunately, relative frequencies of disorders in these kinds of studies are not usually stratified in children and adolescents. Our findings are similar to those of the Cambareri study, which was carried out in four US centers and identified higher frequencies of hypercalciuria and hyperoxaluria in children ≤10 years of age and decreased urinary flow in those over the age of 10.[33]
Our finding of low urinary flow in adolescents stands out, and its cause should be investigated. This could be due to engaging in demanding physical activity without adequate hydration, which is common in school, sports and military settings, or to the trend in these age groups, as identified in the general pediatric population in the United States, to fail to comply with dietary recommendations.[34] We consider promoting increased water intake a fundamental therapeutic recommendation for these age groups, and vital for both primary and secondary urolithiasis prevention.
The low frequency of cystinuria found in this study is consistent with findings in Cuban adults with lithiasis,[28] and contrasts with other studies in China and Turkey, revealing considerably higher frequency. This may be due to genetics underlying the frequency of cystinuria, which exhibits great variability between populations with different ethnic origins.[8,30,31]
The higher frequency of hyperuricosuria in male adolescents seems to be linked to increased concentration of male sex hormones that occurs in the second decade of life. These hormones do not have a direct effect on the frequency of hyperuricosuria, but act through other metabolic mediators.[21,35] Uric acid is produced in the liver as a byproduct of digestion, and, as it cannot be metabolized by humans, constitutes a final metabolic product. This product is then eliminated in the gastrointestinal tract by bacteria that break down uric acid (intestinal uricholysis), a process that is responsible for one third of excretion (the remaining two thirds are excreted in urine).[35] Endogenous production of uric acid is the element that seems to be the most heavily influenced by sex hormones and thus may be responsible for an increase in urinary excretion (hyperuricosuria), which occurs in higher frequencies among overweight and obese adolescents, both of which are nutritional states that are linked to higher incidence rates of hyperuricemia and hyperuricosuria.[36]
Both children and adolescents experience development through notable changes in relatively short periods of time, so it is important to understand how frequencies of disorders most prone to lithogenesis vary by age subgroups. However, there are no other studies that include comparisons between age groups, probably due to the relatively large number of patients that would be required to perform this stratification.
The higher frequency of hypercalciuria in children aged <7 years is consistent with Bergland’s findings in male children aged <8 years,[37] and other evidence pointing to decreased urinary calcium excretion with aging.[38] No dietary modifications were made before this study was carried out, so hypercalciuria could not be classified into renal, intestinal or bone (resorptive hypercalciuria).[20]
The increased rate of hypocitraturia in earlier ages, both in children and adolescent subgroups, is likely due to a progressive increase in urinary citrate excretion with age, as identified by Kirejczyk in a study of 2334 Polish children and adolescents.[39] This is of particular interest, considering the trend pointing to increased frequency of hypocitraturia in several studies of lithiasis patients. This increased rate also points to the importance of urinary citrate which is the most abundant organic anion in urine and is a notable inhibitor of urinary calculi, as it bonds to ionic calcium and reduces urinary calcium saturation, which in turn prevents the growth of calcium crystals in addition to promoting an increase in urinary pH that decreases uric acid lithogenesis.[9,16,30,32,40] In light of the results of this study, young children and younger adolescents would benefit the most from oral citrate salt supplements.
Although the influence of diet on urolithiasis is well known, surprisingly little work has been done exploring the relationship between urolithiasis and nutritional status.[41] This makes it difficult to draw larger comparisons using the results of this study.
Association between hypercalciuria and malnutrition has been studied in particular disorders, like renal tubular acidosis, but at least part of this association is due to a defined calcium cut-off value of 4 mg/kg/day for this disorder, as undernourished and lean individuals, who as a matter of definition have lower body weights than their peers, are diagnosed with hypercalciuria despite having levels of calcium excretion similar to that of other children their age.[16,25] Added to this is new evidence suggesting monogenic causes of urolithiasis, many of which are characterized by the presence of hypercalciuria, which in turn may affect patient nutritional status.[42]
Association of hypocitraturia with thinness and undernutrition have been classically attributed to states of chronic metabolic acidosis that cause increased proximal citrate reabsorption and tissue catabolism.[20,25] Other causes include chronic diarrhea, use of drugs influencing urinary acidification (which were not considered in our study, due to exclusion criteria), and distal renal tubular acidosis (including incomplete forms).[20,43] Although we did not evaluate urinary acidification for the purpose of diagnosing renal tubular acidosis, and this precludes us from making categorical attributions, we are aware that idiopathic hypocitraturia must have made at least some contribution to our study results.[25]
Association of hyperuricosuria with obesity in adolescents was expected, as the relationship between obesity and increased trunk fat with hyperuricemia and hyperuricosuria is known. This has been proposed as an explanation for the increased incidence of lithiasis in adolescents, although not all studies have drawn this conclusion.[36,44–46] Hyperuricosuria not only causes uric acid lithiasis, but also urinary calculi (a phenomenon known as epitaxis). Obesity and states of insulin resistance create conditions of acidic urinary pH, which in turn favors the formation of urate crystals that can constitute nuclei leading to the formation of uric and calcium stones (a phenomenom known as epitaxis).[43,47,48] Prevention and treatment of obesity in adolescents should be included in guidelines for preventing pediatric lithiasis.
The main limitations of this study are the use of only one 24-hour urine sample per patient (more samples are ideal, but these are difficult to obtain in children),[49] the poor representation of children in the total study sample, the use of international cut-off values in defining metabolic disorders and the failure to study urinary acidification or control patients’ diets prior to sample collection, which would have allowed for greater diagnostic precision. However, this research included a considerable number of individuals from across Cuba, with a standardized study protocol, and constitutes the best evidence available for the country on urinary metabolic disorders prone to causing urolithiasis in the pediatric population. It can thus serve as a reference in designing strategies for primary and secondary urolithiasis prevention in Cuban pediatric patients.
CONCLUSIONS Hypercalciuria, decreased urinary flow and hypocitraturia are the main metabolic disorders identified in the Cuban pediatric population with urolithiasis. Hypercalciuria, hypocitraturia and hyperoxaluria are more frequent in children, while decreased urinary flow and hyperuricosuria are more frequent in adolescents. Hypercalciuria in children is most closely related to age and nutritional status. Hyperuricosuria in adolescents is most closely related to age, sex and nutritional status. The findings of this study provide a foundation for the prevention of urolithiasis in Cuban children and adolescents.
Sas DJ, Hulsey TC, Shatat IF, Orak JK. Increasing incidence of kidney stones in children evaluated in the emergency department. J Pediatr. 2010 Jul;157(1):132–7.
Van Dervoort K, Wiesen J, Frank R, Vento S, Crosby V, Chandra M, et al. Urolithiasis in pediatric patients: a single center study of incidence, clinical presentation and outcome. J Urol. 2007 Jun;177(6):2300–5.
Pong YH, Huang WY, Lu YC, Tsai VF, Chen YF, Chang HC, et al. Temporal trend of newly diagnosed incidence, medical utilization, and costs for pediatric urolithiasis, 1998-2007: a nationwide population-based study in Taiwan. Urology. 2015 Jan;85(1):216–20.
Schwaderer AL, Cronin R, Mahan JD, Bates CM. Low bone density in children with hypercalciuria and/or nephrolithiasis. Pediatr Nephrol. 2008 Dec;23(12):2209–14.
Routh JC, Graham DA, Nelson CP. Epidemiological trends in pediatric urolithiasis at United States freestanding pediatric hospitals. J Urol. 2010 Sep;184(3):1100–4.
Pietrow PK, Pope JC 4th, Adams MC, Shyr Y, Brock JW 3rd. Clinical outcome of pediatric stone disease. J Urol. 2002 Feb;167(2 Pt 1):670–3.
Wang HHS, Wiener JS, Lipkin ME, Scales CD Jr, Ross SS, Routh JC. Estimating the nationwide, hospital based economic impact of pediatric urolithiasis. J Urol. 2015 May;193(5 Suppl):1855–9.
Spivacow FR, Negri AL, del Valle EE, Calviño I, Fradinger E, Zanchetta JR. Metabolic risk factors in children with kidney stone disease. Pediatr Nephrol. 2008 Jul;23(7):1129–33.
Velásquez-Forero F, Esparza M, Salas A, Medeiros M, Toussaint G, Llach F. Risk factors evaluation for urolithiasis among children. Bol Med Hosp Infant Mex. 2016 Jul–Aug;73(4):228–36.
Funes P, Echagüe G, Ruiz I, Rivas L, Zenteno J, Guillén R. Perfil de riesgo litogénico en pacientes con urolitiasis en Paraguay. Rev Méd Chile. 2016 Jun;144(6):716–22. Spanish.
Berdasco A, Esquivel M, Gutiérrez JA, Jiménez JM, Mesa D, Posada E, et al. Segundo estu dio nacional de crecimiento y desarrollo. Cuba, 1982: valores del peso y talla para la edad. Rev Cubana Pediatr. 1991 Jan–Apr;63(1):4–21. Spanish.
Esquivel M, Rubí A. Valores cubanos del índice de masa corporal en niños y adolescentes de 0 a 19 años. Rev Cubana Pediatr. 1991 May–Aug;63(3):181–90. Spanish.
Dubois D, Dubois EF. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition. 1989 Sep–Oct;5(5):303–11.
Badell Moore A, Bacallao Méndez RA, Mañalich Comas R. Sobre el establecimiento de valores de referencia de la excreción de creatinina para la población cubana. Rev Cubana Aliment Nutr. 2015 Jan–Jun;25(1 Suppl 1):S28–S60. Spanish.
Hoppe B, Kemper MJ. Diagnostic examination of the child with urolithiasis or nephrocalcinosis. Pediatr Nephrol. 2010 Mar;25(3):403–13.
Durán Álvarez S. Urolitiasis en el niño. Rev Cubana Pediatr. 2013 Jul–Sep;85(3):371–85. Spanish.
Sorokin I, Mamoulakis C, Miyazawa K, Rodgers A, Talati J, Lotan Y. Epidemiology of stone disease across the world. World J Urol. 2017 Sep;35(9):1301–20.
Bacallao Méndez RA, Victores Aguiar I, Mañalich Comas R, Gutiérrez García F, Llerena Ferrer B, Almaguer López M. Caracterización clínico epidemiológica de la litiasis urinaria en un área rural de Artemisa. Rev Cubana Invest Bioméd. 2016 Oct–Dec;35(4):300–10. Spanish.
Seitz C, Fajkovic H. Epidemiological gender-specific aspects in urolithiasis. World J Urol. 2013 Oct;31(5):1087–92.
Coward RJM, Peters CJ, Duffy PG, Corry D, Kellett MJ, Choong S, et al. Epidemiology of paediatric renal stone disease in the UK. Arch Dis Child. 2003 Nov;88(11):962–5.
Dwyer ME, Krambeck AE, Bergstralh EJ, Milliner DS, Lieske JC, Rule AD. Temporal trends in the incidence of kidney stones among children: a 25-year population-based study. J Urol. 2012 Jul;188(1):247–52.
Chan KH, Moser EA, Whittam BM, Misseri R, Cain MP, Krambeck A, et al. Initial collection of an inadequate 24-hour urine sample in children does not predict subsequent inadequate collections. J Pediatr Urol [Internet]. 2019 Feb [cited 2020 Mar 17];15(1):74.e1–74.e7. Available at: http://www.sciencedirect.com/science/article/abs/pii/S1477513118306387
Besouw MTP, Bienias M, Walsh P, Kleta R, Van’t Hoff WG, Ashton E, et al. Clinical and molecular aspects of distal renal tubular acidosis in children. Pediatr Nephrol. 2017 Jun;32(6):987–96.
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017 Dec 16;390(10113):2627–42.
El-Zoghby ZM, Lieske JC, Foley RN, Bergstralh EJ, Li X, Melton LJ 3rd, et al. Urolithiasis and the Risk of ESRD. Clin J Am Soc Nephrol. 2012 Sep;7(9):1409–15.
Bacallao Méndez RA, Madrid Mancia C, Mañalich Comas R, Gutiérrez García F, Badell Moore A. Trastornos metabólicos renales en pacientes cubanos adultos con litiasis urinarias. Rev Cubana Med. 2014 Sep–Dec;53(4):456–67. Spanish.
Spivacow FR, Negri AL, del Valle EE, Calvino I, Zanchetta JR. Clinical and metabolic risk factor evaluation in young adults with kidney stones. Int Urol Nephrol. 2010 Jun;42(2):471–5.
Celiksoy MH, Yilmaz A, Aydogan G, Kiyak A, Topal E, Sander S. Metabolic disorders in Turkish children with urolithiasis. Urology. 2015 Apr;85(4):909–13.
Yang D, Tiselius HG, Lan C, Chen D, Chen K, Ou L, et al. Metabolic disturbances in Chinese children with urolithiasis: a single center report. Urolithiasis. 2017 Jun;45(3):285–90.
Sepahi MA, Eftekhari SS, Shahmoradi S, Talebizadeh M, Rashidinia S, Hejazi SS. Metabolic and anatomic abnormalities associated with pediatric nephrolithiasis: a cross-sectional study. Int J Pediatr. 2017 May;5(5):4833–8.
Cambareri GM, Kovacevic L, Bayne AP, Giel D, Corbett S, Schurtz E, et al. National multi-institutional cooperative on urolithiasis in children: age is a significant predictor of urine abnormalities. J Pediatr Urol. 2015 Aug;11(4):218–23.
Kant AK, Graubard BI. Contributors of water intake in US children and adolescents: associations with dietary and meal characteristics – National Health and Nutrition Examination Survey 2005-2006. Am J Clin Nutr. 2010 Oct;92(4):887–96.
Kubota M. Hyperuricemia in children and adolescents: present knowledge and future directions. J Nutr Metab [Internet]. 2019 May 2 [cited 2020 Mar 17];2019:Art ID 3480718. Available at: https://www.hindawi.com/journals/jnme/2019/3480718/
Shatat IF, Abdallah RT, Sas DJ, Hailpern SM. Serum uric acid in U.S. adolescents: distribution and relationship to demographic characteristics and cardiovascular risk factors. Pediatr Res. 2012 Jul;72(1):95–100.
Bergsland KJ, Coe FL, White MD, Erhard MJ, DeFoor WR, Mahan JD. Urine risk factors in children with calcium kidney stones and their siblings. Kidney Int. 2012 Jun;81(11):1140–8.
Butani L, Kalia A. Idiopathic hypercalciuria in children how valid are the existing diagnostic criteria? Pediatr Nephrol. 2004 Jun;19(6):577–82.
Kirejczyk JK, Porowski T, Konstantynowicz J, Kozerska A, Nazarkiewicz A, Hoppe B, et al. Urinary citrate excretion in healthy children depends on age and gender. Pediatr Nephrol. 2014 Sep;29(9):1575–82.
Kovacevic L, Wolfe-Christensen C, Edwards L, Sadaps M, Lakshmanan Y. From hypercalciuria to hypocitraturia a shifting trend in pediatric urolithiasis? J Urol. 2012 Oct;188(4 Suppl):1623–7.
Saxena A, Sharma RK. Nutritional aspect of nephrolithiasis. Indian J Urol. 2010 Oct;26(4):523–30.
Daga A, Majmundar AJ, Braun DA, Gee HY, Lawson JA, Shril S, et al. Whole exome sequencing frequently detects a monogenic cause in early onset nephrolithiasis and nephrocalcinosis. Kidney Int. 2018 Jan;93(1):204–13.
Copelovitch L. Urolithiasis in children. Pediatr Clin North Am. 2012 Aug;59(4):881–96.
Shavit L, Ferraro PM, Johri N, Robertson W, Walsh SB, Moochhala S, et al. Effect of being overweight on urinary metabolic risk factors for kidney stone formation. Nephrol Dial Transplant. 2015 Apr;30(4):607–13.
Kokorowski PJ, Routh JC, Hubert KC, Graham DA, Nelson CP. Association of urolithiasis with systemic conditions among pediatric patients at children’s hospitals. J Urol. 2012 Oct;188(4 Suppl):1618–22.
Sarica K, Eryildirim B, Yencilek F, Kuyumcuoglu U. Role of overweight status on stone-forming risk factors in children: a prospective study. Urology. 2009 May;73(5):1003–7.
Bacallao Méndez RA, Mañalich Comas R, Gutiérrez García F, Badell Moore A, Caldevilla Rodríguez Y. pH urinario y estado nutricional en pacientes cubanos con urolitiasis. Rev Cubana Med. 2015;54(2):119–28. Spanish.
Murphy MO, Erpelding SG, Chishti AS, Dugan A, Ziadab A, Kiessling SG. Influence of BMI in nephrolithiasis in an Appalachian pediatric population: a single-center experience. J Pediatr Urol [Internet]. 2018 Aug [cited 2020 Mar 19];14(4):330.e1–330.e8. Available at: http://www.sciencedirect.com/science/article/pii/S1477513118301931
Parks JH, Goldfisher E, Asplin JR, Coe FL. A single 24-hour urine collection is inadequate for the medical evaluation of nephrolithiasis. J Urol. 2002 Apr;167(4):1607–12.
THE AUTHORS Raymed Antonio Bacallao-Méndez (Corresponding author: raymed@infomed.sld.cu), nephrologist with master’s degrees in emergency medicine and diagnostic methods. Associate professor and associate researcher, Dr Abelardo Buch López Nephrology Institute (INEF), Havana, Cuba. https://orcid.org/0000-0002-7043-0597
Reynaldo Mañalich-Comas, nephrologist with a doctorate in medical sciences. Senior professor and senior researcher, INEF, Havana, Cuba. https://orcid.org/0000-0002-9424-5839
Francisco Gutiérrez-García, physician specializing in biostatistics, with a master’s degree in bioethics. Associate professor and researcher, INEF, Havana, Cuba. https://orcid.org/0000-0002-9972-4142
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.