Cuba has been building a national strategy using information and communication technologies (ICTs) for health since the establishment of the National Medical Sciences Information Center (CNICM) in 1965. Back then, vital statistics and health data – considered a cornerstone of the country’s new universal health system – were transmitted by hand or over the phone. As technology grew more sophisticated over the next 30 years, microprocessors and computers were integrated into the process. In 1992, reeling from economic crisis, Cuba founded the national health telematics network known as INFOMED (www.sld.cu), betting on the strategy that ICTs could be used to improve population health at low cost. From these initial efforts until today, the country has followed a policy to build and strengthen a virtual health information infrastructure.[1]
Early on, systematizing health data took on a sense of urgency as Cuba confronted the double burden of infectious and chronic diseases and their implications for health policy and programs. But data collection threatened to escalate and administrative responsibilities falling to the country’s health practitioners, then as now, took time away from patients. None of this is unique to Cuba: health systems in the developing world face the same double burden, while also coming under increasing pressure to produce reliable health statistics for international funders and to measure progress towards the UN Millennium Goals.
In fact, evidence shows that developing countries lag far behind in reliableact data collection for even the most basic indicators, including mortality. A recent World Health Organization (WHO) study found that of 115 Member States reporting, 75 had no information on cause of death after 1990; 90% of Africa fell into this category. Furthermore, another 39 states had no mortality data available whatsoever.[2] It is precisely in this area of eHealth that the Cuban experience has relevance, especially for similar resource-scarce settings.
Building a National eHealth Capacity
Cuba’s policy to create a virtual health infrastructure arose from the perennial public health administration dilemma: how to coordinate and share health data, information, and findings in an effective and efficient way so as to improve health delivery and outcomes? In short, how could the Cuban health system ‘manage what it measures,’ as the saying goes?[3]
This question propelled INFOMED into existence, with the aim of integrating health data coming from the local, provincial, and national levels and various institutions. This was a preliminary step to INFOMED’s longer- term goal of linking the entire national health system in a digital network that would provide accurate, consistent, and timely information for decision-making and improving service delivery, at no charge to users (See: A Case Analysis of INFOMED: The Cuban National Health Care Telecommunications Network and Portal; Cuba & ICTs: Real Crisis Leads to Virtual Innovation). “The strategy is to use ICTs in an intelligent and prioritized way to improve health outcomes,” says INFOMED Director Pedro Urra.[4]
In 1997, national guidelines were drafted to systematize the approach both throughout the different levels of the health system and across institutions that work together to benefit health (the intersectoral design that is a hallmark of the Cuban system); this includes national research centers, hospitals, community polyclinics, dental clinics, and even nursing homes (see Table 1). The guidelines focus on a series of health information management methods, techniques, and procedures, in the following areas:
- General state of Cuban population health
- Health sciences’ knowledge and resources
- Information for epidemiological, operational, and strategic decision-making
- Training human resources for health • Automation of services
- Research support
The approach is based on several core principles that drive the process:
- It is patient-centered
- Individual privacy, security, and confidentiality standards must be observed
- The system will be built, maintained, and strengthened using open source software
- Access will be equitable • System sustainability must be built-in
- Impact will be evaluated based on the quality and safety of medical services and population health outcomes
Factors Favoring a National Strategy
Cuba has several contextual factors favoring the development of a national eHealth strategy, including, ironically, lack of resources.
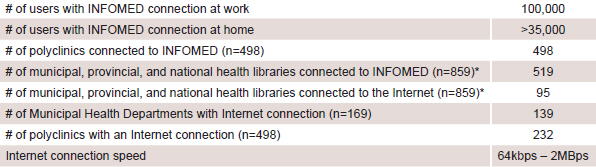
Table 1: Fast Facts: Cuban Health System Connectivity
Source: All data from Pedro Urra, personal communication, December 2, 2007, except *, from Anuario Estadístico de Salud 2006. MINSAP, Havana: 2007.
The seminal WHO report Building Foundations for eHealth, states, “the eHealth community needs to examine how…to prevent eHealth from being driven by ‘technology push’ rather than by needs-based and evidence-led ‘technology pull.'”[5] The Cuban system and its eHealth strategy are needs-based and evidence-led by design; lack of resources, however, mean both are guided by technology push by default.
In the report, the WHO Global Observatory for eHealth identifies three layers of strategic development enabling countries to implement a national strategy; within each are several actionable phases:
1. Foundation policies & strategies – Infrastructure; Funding; Policy; Governance
2. Enabling policies & strategies – Capacity building; Interoperability; Multilingualism & cultural diversity; Equity; Citizen protection
3. eHealth applications – Provider services; Knowledge services; Public services
Cuba’s foundation strategy lends itself to the development of a national system: accurate, timely statistics-gathering systems were already in place, as were trained health professionals to collect the data, when the nation’s eHealth policy was designed. Collaboration among other institutions working together in an intersectoral approach has allowed Cuba to further these foundation policies and strategies in a fairly swift and coordinated way. Nevertheless, this coordination is extraordinarily complex and strengthening the synergy among the different sectors will require continued good governance and sustained funding.
Already Cuba has certain enabling policies in place, defined as “a bridge between foundation strategies and the planned outcome of providing eHealth services for all.”[5] But building that bridge requires a level of computer literacy and competency that not all Cuban health professionals have. Consequently, designers of the country’s virtual health strategy have identified capacity-building among users as their number one challenge. To face this challenge, they’ve begun implementing an aggressive Informatics Literacy Program that trains health professionals to “know when and why they need information, where to find it, and how to analyze, use, and communicate it in an ethical manner.”[6]
Further priority enabling actions include: drafting and enacting eHealth software and hardware standards (service architecture, description language, design requirements, etc.) in order to maximize compatibility moving forward; implementing best practices; documenting the entire eHealth strategy production process; and ensuring independence of the databases.
In terms of implementing eHealth applications, Cuba has, to a large extent, ‘leap-frogged’ over technological and resource constraints by introducing an array of applications for health professionals, students, and the general public. These products and services are generally divided into: primary care, secondary and tertiary care, research, epidemiology, medical education, and health administration. All are available free of charge through INFOMED. Since the philosophy underpinning the virtual infrastructure is equitable access to information designed to improve population health, eServices including second opinions and electronic diagnostic image exchange, have taken priority over other bandwidth- and resource-intensive applications such as telemedicine.[7]

All 498 polyclinics (community-based clinics offering both primary and secondary care) in Cuba are connected to INFOMED and have at least four computer stations. Additionally, there are currently over 230 polyclinics throughout the country connected to the Internet (see Table 1). The next step is to implement decisionmaking software and extend the full ICT bundle to all polyclinics nationwide. Services available to patients in pilot phases include ‘Consult a Specialist’ and ‘Make an Appointment Online.’ Additionally, there are five hospitals where the family health record (similar to individual electronic health records, but for an entire family) is being piloted for primary care.
Health surveillance and epidemiological prediction software has been used to appreciable effect in Cuba. For example, the extent of the 2001 dengue outbreak in Guantánamo Province was predicted with great precision using Prospective Methodology software developed in Cuba (See Interview: Jacinto Duverger). Another Cuban-produced application, VigiRed, for daily epidemiological tracking, will soon be piloted in four Havana City municipalities. It is expected that such locally-produced software will eventually become a source of export income.
In Cuba’s eHealth strategy, as in its public health strategy, research and education are of primary importance; to this end, many applications with training and research purposes are available to health professionals both around the country and around the world via INFOMED. This includes the Virtual Health Library which grants free, 24-hour access to specialized international databases and some 2,000 medical, scientific, and health journals (MedLine, BIREME, Cochrane Library, EBSCO, PLoS, etc); and the Virtual Health University, which offers various degree-conferring courses, including one in Health Information Management. The Virtual Vaccine Library and its associated Virtual Vaccinology Classroom, are innovative portals for scientific research, consultations, and evaluation pertaining to vaccines (See Feature: Cuba’s Virtual Libraries: Knowledge Sharing for the Developing World).
Additional eHealth applications already functioning include specialized networks in nephrology, intensive care, cardiology, and pharmacies, and there is a growing electronic publishing capacity. Future applications include a national health economy management system and a hospital-level management system (digital diagnostic results, inventories, accounting, etc.).
Taken together, these eHealth applications have made INFOMED one of the heaviest trafficked health portals in the world. Of 500,000 sites on the Internet, INFOMED ranked 6,142 according to traffic rankings by Alexa.com. Comparatively, the WHO ranked 3,993 and PAHO 25,777.[8]
Cuban eHealth Timeline
1965 – National Medical Sciences Information Center (CNICM) founded.
1974 – First computer installed for public health ends, at the National Institute of Oncology & Radiobiology.
1976 – Center for Cybernetics Applied to Medicine (CECAM) established.
1984 – Informatics organizational policy drafted.
1985 – Microcomputers introduced at the Ministry of Public Health (through 1989).
1987 – Center for the Development of Informatics in Public Health (CEDISAP) founded.
1992 – INFOMED founded.
1994 – All Cuban medical and scientific journals made openly accessible in electronic format via INFOMED.
1998 – National Statistics Division begins digitizing 128 statistical subsystems nationwide and introducing personal computers for use by health professionals.
1998 – Teaching & Software Laboratory Network established; massive training of health professionals in informatics begins.
1998 – Agreement reached to develop regional Virtual Health Library.
2000 – Health Informatics Groups founded in every province to coordinate strategy.
2001 – eHealth management systems piloted in six Havana City polyclinics.
2002 – Pilot is extended to 94 polyclinics. 2002 – University of Computer Sciences (UCI) founded.
2003 – Digitization of research, scientific, and technical information prioritized to train health professionals.
2004 – New phase of information system strategy for National Health System begins.
2005 – Digital health and blood bank registries launched. 2006 – Virtual Vaccine Library and Latin American Network of Scientific & Technical Vaccine Information launched.
2007 – Virtual Vaccinology Classroom launched.
2007 – Digital hospital information system and national image network launched.
Moving Forward & Challenges Ahead
Strengthening Cuba’s virtual health infrastructure means evaluating the process to date and implementing changes to improve system performance. Efforts to ensure the availability, compatibility, and sustainability of eHealth services and products already online must also be reinforced.
Inarguably, the biggest challenges facing Cuba’s strategy are related to human and financial resources. Research has shown that capacity-building to effectively and efficiently use ICTs for health is most urgent (See: Open Access Journals: Knowledge and Attitudes among Cuban Health Researchers). While training health professionals, policy makers, administrators, and support staff is already underway with the Informatics Literacy Program, this will take time to bear fruit.
Logically, getting the technology in place – from connectivity to computers – is a real barrier for resource-scarce settings. In Cuba’s case, that barrier is fortified by the US economic and financial embargo, which prohibits Cuba from buying equipment of all types, from any source, that contain 10% or more US-produced components. Not only does this drive up the price of technology and limit access to the latest innovations, it introduces high levels of uncertainty into the supply chain thereby affecting sustained planning and growth.
Effective evaluation of the impact of the strategy cannot be overemphasized: since Cuba is able to – and will increasingly – provide evidence-based results of the country’s eHealth strategy, the experience can help answer fundamental questions faced by health systems worldwide: has ICT in health led to productivity gains? Has the quality of care improved, stayed the same, or declined? Has patient satisfaction? Is eHealth effectively working towards disease prevention? What impact has ICT had on the economics of health? Whatever the answers, Cuba’s experience makes it clear that a developing country can begin to bridge the digital divide.
References

- Delgado A, Vidal ML. Informática en la salud pública cubana. Rev Cubana Salud Pública. 2006;32(3).
- Mathers CD, Ma Fat D, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Organ 2005;83:171-7.
- World Health Organization. World Health Report 2006: Working Together for Health. 2006; Geneva.
- Personal Communication. December 2, 2007.
- WHO Global Observatory for eHealth. Building Foundations for eHealth: Progress of Member States. Geneva: World Health Organization; 2006.
- INFOMED Glosario [homepage on the Internet]. Havana: INFOMED; c1999-2007 [updated 2007 Nov 11; cited 7 Dec 2007]. Alfabetización informacional; [1 screen]. (Translated by authors). Available from: http:// INFOMED20.sld.cu/wiki/doku.php/alfabetizacion_informacional
- Telemedicine has been performed successfully in Cuba, notably in bilateral surgical collaborations between the Carlos Finlay Orthopedic Hospital and the Ramón Pando Ferrer Ophthalmology Institute, both in Havana, and Indiana University.
- Alexa: The Web Information Company [homepage on the Internet]. City: Aleza; c1996-2007 [updated 2007 Dec 7; cited 2007 Dec 7]. Traffic Details for WHO, INFOMED, PAHO; [4 screens]. Available from: www.alexa.com