Chronic diseases are Cuba’s number one health problem, causing 90% of all deaths. The top three killers (in order) are: heart disease, cancer and cerebrovascular diseases, which together account for nearly 60% of all deaths.


Chronic diseases are Cuba’s number one health problem, causing 90% of all deaths. The top three killers (in order) are: heart disease, cancer and cerebrovascular diseases, which together account for nearly 60% of all deaths.
Chronic diseases are Cuba’s number one health problem, causing 90% of all deaths. The top three killers (in order) are: heart disease, cancer and cerebrovascular diseases, which together account for nearly 60% of all deaths.[1]
Chronic vascular conditions are central to this dilemma, sharing risk factors common in the Cuban population:

Panorama of Chronic Vascular Diseases
Recent studies reveal co-existence of these risk factors, as well as co-morbidity among the most important chronic vascular conditions in Cuba (see Prevalence of Obesity and its Association with Chronic Kidney Disease, Hypertension and Diabetes Mellitus. Isle of Youth Study (ISYS), Cuba and Cardiovascular Risk among Older Women in a Havana Health Area). The state of chronic vascular diseases in Cuba can be summed up as follows:[2]
Hypertension (HTN), a disease in itself, is also the most important risk factor in Cuba for coronary heart disease, cerebrovascular disease, and chronic kidney disease; and contributes to retinopathy. In 2004, 24% of Cuba’s adult population had high blood pressure, although HTN is likely under-diagnosed; the rate might actually be as high as 33%, according to epidemiological studies.
Coronary heart disease (CHD) accounted for 18.8% of total deaths and 72.5% of deaths from heart disease in 2004 (15,000 deaths annually). In 2004, there were 285,969 patients diagnosed with coronary heart disease.
Cerebrovascular diseases are on the rise, responsible for 7,000 to 8,000 deaths annually. In 2004, there were 52,717 patients diagnosed with cerebrovascular diseases (4.7 per 1,000 pop.). Age and hypertension are the main associated risk factors.
Diabetes mellitus (DM) was the 8th cause of death in 2004, and accounts for 1,400 to 1,800 deaths annually, or 2.3% of total deaths. Its prevalence is on the rise: 342,371 patients were living with diabetes in 2004 (30.5 per 1,000 pop.). DM is thought to be under-diagnosed; is associated mainly with age and weight gain; and is an important risk factor for heart attack, stroke, and renal disease. Mortality: 11.4 per 100,000 pop.
Chronic kidney disease (CKD) is emerging as an important health problem in Cuba. In 2004, it was the 13th cause of death (503 deaths or 0.6% of all deaths). Prevalence of patients with chronic renal insufficiency in 2004 was 0.87 per 1,000 pop. (9,761 patients). Epidemiological studies project some 1.8 million Cubans are at some stage of CKD; of those, 210,360 suffering from chronic renal insufficiency, and 3,360 requiring dialysis or transplant. Thus, under-diagnosis is evident. For patients in dialysis, incidence is rising at approximately 14% per year (reaching 1,246 patients, or 111 per million pop.) in 2004; and prevalence increased to 2,290 or 213.4 per million population by the end of 2007.[4]
Implications for the Health System
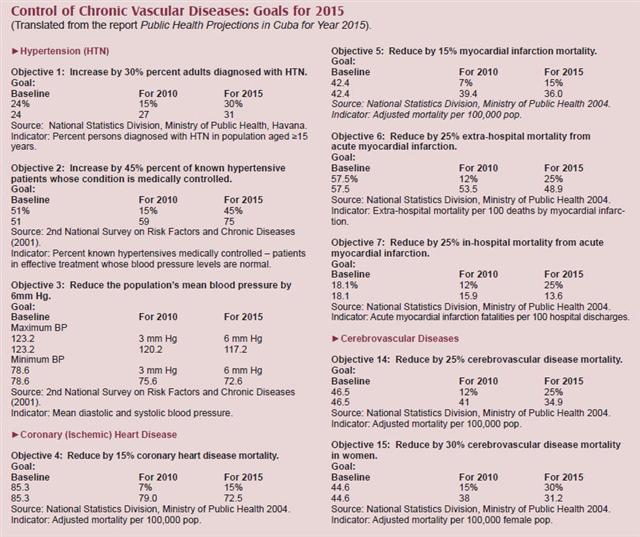
Dr Joaquin García, Vice Minister of Public Health for Medical Attention, says chronic diseases “have forced us to reformulate our public health strategies for the coming years,” the goals of which are contained in the 2006 report Public Health Projections in Cuba for Year 2015.[2]
“We had overcome the main infectious diseases by the 1980s, but it wasn’t until 1991 that we began to think about an integrated approach to chronic conditions, developing a plan through year 2000,” Dr García told MEDICC Review. “But the strategy was smothered by the economic crisis of the 1990s.” Nevertheless, during that decade, national prevention and management programs were implemented in hypertension, diabetes, atherosclerosis, stroke, coronary heart disease; and also updated in chronic kidney disease.
Then, as the country recovered, new strategic thinking began to emerge, both for chronic vascular diseases and cancer. This has been aided by the following initiatives:
1) Broad community-based epidemiological studies in chronic diseases, especially chronic kidney disease (Isle of Youth, Cerro Municipality and Pinar del Río Province); heart disease; and diabetes (Jaruco, Havana Province). “In each study, researchers have sought out under-diagnosed cases and comorbidity, thus determining real prevalence,” says Dr García. Such early active detection was subsequently applied in pilot programs in various municipalities and provinces. This has begun to generate a reliable national mapping of chronic vascular conditions, as well as cancer, and also a reinforced concept of shared risk factors. “Risk factors are more important than the diseases themselves,” says Dr García, “especially if you are serious about prevention.”
2) Based on this work, launching pilot annual family examination and diagnosis programs in 30 polyclinics later this year. “Before this, many times, not everyone was examined annually, and if they were, each person received the same exam and lab tests. Now, we draw from the epidemiological studies to refine this process, and orient which groups of people and families need which kinds of work-ups. This is about genetics, about demographics, about knowing the population,” notes Dr Garcia.
He stresses that this approach brings another change: “we were talking about family medicine, but often just looking at individuals in a family. But a family is more than the sum of its members – these people share common genetic and environmental characteristics, even bad habits are passed down from one generation to another. So, the epidemiological studies have enriched family medicine and primary care.”
3) Continued development of multidisciplinary services in polyclinics, tailored to risk factors and conditions most common in the community served by the facility. This movement was begun with the refurbishing of polyclinics in 2004-2005,[5] and is accelerating as early active detection surveys lead to more precise community health diagnoses. “These services are patient-centered, not speciality-centered,” says Dr García. “An endocrinology service isn’t the same as a service providing comprehensive care for diabetics – where they can see an ophthalmologist, nephrologist or another specialist.”
4) Establishment of the national Health & Quality of Life Commission (2001), which began looking at health more comprehensively, including these diseases and their risk factors. The multidimensional approach involves national and local agencies beyond the health sector (agriculture, environment, water resources, the food industry, transportation, education, sports, etc.). The commission is responsible for provincial and municipal mapping of such key data as rates of specific diseases, smoking, work-related and traffic accidents, vegetable consumption, and regular physical activity by adults. They periodically carry out provincial evaluations on implementation of regulations governing public smoking, cigarette and alcohol purchases and pricing; and on such issues as availability of fruits and vegetables in local markets, thus informing development of new legislation and local regulations.
“In fact, our biggest challenge ahead is quality of life,” says Dr García. “And chronic diseases have pushed us to address this more forcefully. Primary health care was an excellent start to “health for all,” but it wasn’t capable of handling these chronic conditions well: it needs enriching by an intersectorial approach like the one used by the Health & Quality of Life Commission.”
“In the 21st Century, government’s mission of protecting the public’s health and providing medical services also implies a responsibility to create conditions for people to exercise their right and responsibility to safeguard their own health. That is, government must increase access to healthy foods, parks and recreational facilities, ensure clean air,” says the Vice Minister. “The Health & Quality of Life Commission is government’s recognition of its role in influencing at least some of the social determinants of health. And that’s where it begins.”
Reed G. Chronic Vascular Diseases in Cuba: Strategies for 2015. MEDICC Rev. 2008;10(2):5–7.
