ABSTRACT
This paper contextualizes the chronic kidney disease epidemic and related burden of disease affecting Central American farming communities. It summarizes the two main causal hypotheses (heat stress and agrochemicals), draws attention to the consequences of dichotomous reasoning concerning causality, and warns of potential conflicts of interest and their role in “manufacturing doubt.” It describes some methodological errors that compromise past study findings and cautions against delaying public health actions until a conclusive understanding is reached about the epidemic’s causes and underlying mechanisms. It makes the case for a comprehensive approach to the historical, social and epidemiological facts of the epidemic, for critically assessing existing studies and for enhanced rigor in new research.
KEYWORDS: Epidemiology, public health, chronic kidney disease, causality, epidemic, agriculture, environment, agrochemicals, pesticides, heat stress, social determinants of health, Central America
INTRODUCTION
In 2002, the first alarm was sounded on a spike in cases of chronic kidney disease (CKD) in Central American farming communities.[1] Only in 2013, however—after several years of neither concerted nor effective action to stem the ensuing epidemic—did PAHO member states recognize this new type of CKD as an important public health problem and agree on urgent, coordinated action to address it.[2]
The CKD described most frequently in certain economically and socially marginalized farming communities on the Pacific coast of Central America and southern Mexico[3–6] poses important challenges for clinical medicine, epidemiology and public health. Among these are: clinical characterization of a disease not entirely attributable to traditional causes; fully understanding its pathogenesis; and the need for stronger surveillance systems to determine its burden and patterns of distribution.
A PAHO analysis showed that by about 2008, mortality from chronic renal failure (N18, ICD-10), a proxy for the kind of CKD being reported in Central America, was substantially higher in El Salvador (41.9/100,000 population) and Nicaragua (39.5/100,000) than elsewhere in the Americas.[7] Consistent with other studies conducted in these two countries,[3,4] mortality from chronic renal failure was markedly higher in men than in women: 64.5/100,000 vs. 24.1/100,000 in El Salvador and 63.0/100,000 vs. 18.2/100,000 in Nicaragua. The latter pattern contrasts sharply with those seen, for example, in the USA (4.3 vs. 3.2/100/000) and Cuba (2.8 vs. 2.2/100,000).[7] Thus, the two CKD mortality figures for El Salvador and Nicaragua are equally striking when compared to the rest of the hemisphere’s overall mortality and sex-related mortality.
Another indicator of the epidemic’s impact in Central America is disability-adjusted life years lost (DALY). A 2010 Institute of Health Metrics and Evaluation (IHME) study found that CKD was among the top ten causes of age-standardized DALYs in Central Latin America (includes Colombia, Mexico and Venezuela).[8] In fact, CKD-attributable DALYs virtually doubled (increased by 99%) in this region between 1990 and 2010, their rank as DALY causes ascending from 18th to 7th. The increase in CKD-attributable DALYs during the period was 6% globally and 46% in Central Asia, the latter the second greatest increase of any region in the world. In Central Latin America, CKD-attributable DALYs present a more serious problem among men, although with notably high rates in women, which have increased by 80% over the 20-year period, compared to 123% among men.[8]
The type of CKD described in Central Latin America disproportionately affects young male farmworkers, although rates are also high in women and nonfarmworkers living in agricultural communities.[4] In fact, according to IHME, in persons aged 15–49 years—rarely seen with renal complications from diabetes or hypertension—CKD ranked 17th in DALYs among all diseases affecting this age group in the region, having increased 132% since 1990.[8]
This paper examines several methodological and conceptual challenges to addressing this serious health problem, emphasizing the role of epidemiology and its connection to public health, as well as the pitfalls encountered by both disciplines related to research hypotheses proposed thus far concerning the CKD epidemic in Central American agricultural communities.
THE HYPOTHESES
Deaths of young people from CKD, health services overwhelmed by hundreds of patients and the many demands of civil society have given rise to alarming news articles[9–11] and numerous studies, scientific conclaves and political declarations. Among the latter, the one that most completely sums up this grave situation is the San Salvador Declaration, adopted at the High-level Meeting on Chronic Kidney Disease of Nontraditional Causes in Central America [CKDnc] held in El Salvador (April, 2013). The Declaration described CKD as having “catastrophic” effects associated with toxic-environmental and occupational factors, dehydration and behaviors harmful to renal health. In it, the Ministers of Health of the Central American Integration System (SICA, the Spanish acronym) declared their commitment to address CKDnc comprehensively and to “strengthening scientific research in the framework of the prevention and control of chronic noncommunicable diseases.”[12] The Declaration was subsequently endorsed by the 52nd session of PAHO’s Executive Committee.[2]
From results of investigations on the CKDnc epidemic in Central America, we perceive emergence of two nonexclusive hypotheses to explain the problem; our vision is summarized in Table 1.
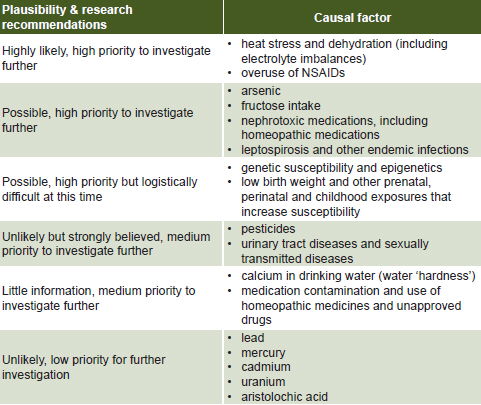
In 2012, Heredia National University in Costa Rica organized an international workshop at the behest of the Program on Work, Environment and Health in Central America (SALTRA, the Spanish acronym).[13] Inspired by studies defending the hypothesis of the impact of heat and dehydration on kidney physiology,[14–17] the predominant view was that the epidemic could be attributed primarily to repeated episodes of dehydration resulting from exposure to high ambient temperatures while performing heavy labor, such as farm work, especially manual sugarcane harvesting. Excessive use of NSAIDs and fructose-containing rehydration fluids were also recognized as possible cofactors. Inorganic arsenic, leptospirosis, pesticides and hard water were considered possible contributors to the epidemic. However—minimizing considerable evidence indicating damaging health effects of agrochemicals as a longstanding problem in the region[18,19]—participants put pesticides in the “possible cause” category of “unlikely but strongly believed,” and relegated their “further research” category to “medium priority” (Table 2).[13]
Table 1: Etiological hypotheses on chronic kidney disease not attributable to traditional causes

The El Salvador conference, influenced by older work (e.g., Morgan),[20] more recent studies[21–23] and as yet unpublished clinical, histopathologic and toxicologic findings presented at the conference itself, supported a hypothesis pointing to multifactorial origins of the epidemic, but stressing the role of agrochemicals, either from direct and prolonged exposure, or from longstanding residual contamination of soil, water and crops, compounded by harsh working conditions, exposure to high temperatures and insufficient water intake.[12]
Table 2: Conclusions about causes by degree of plausibility at international workshop on “Mesoamerican nephropathy”
Source: Based on Mesoamerican Nephropathy: Report from the First International Research Workshop on MeN, San José, 2012 [13]
Dismantling the false dichotomy of “proven” versus “not proven” The fundamental task of environmental epidemiology is to make judgments about the causal nature of empirical associations observed between exposure to environmental agents and occurrence of disease.[24] Effectively, its job is to discover what has come to be called the “etiology of population health.”[25] A landmark in this endeavor was Bradford Hill’s proposed list of nine conditions to guide inference when it is unfeasible or ethically unacceptable to experiment to determine whether or not an observed association is causal.[26]
But only one of these criteria is a sine qua non, temporality: that the putative cause must take place before the effect of interest; that is, in this case, exposure before outcome. The remaining eight conditions have been the object of critical review, and consensus is that they are not all equally important.[27] And over the past 15 years increasing concern has been expressed about limitations of the risk-factor approach implicit in Hill’s criteria, leading to various alternative approaches.
For decades, Hill’s criteria represented “the gold standard,” ignoring his own statement: “All scientific work is liable to be upset or modified by advancing knowledge.” Furthermore, he also maintained, “[This] does not confer upon us a freedom to ignore the knowledge we already have, or to postpone the action that it appears to demand at a given time.”[26]
In other words, knowledge is always provisional and perfectible. In contrast, actions—the making of laws and policies, the design of health measures and interventions—are indeed dichotomous: they are enacted or not. Decisions are made in an environment of uncertainty and amidst of a web of constraints; but this does not mean that action to address a health problem—especially a grave one—can be put off indefinitely, waiting for definitive confirmation that may never come. As Michaels warned, “It is vital that those charged with protecting the public’s health understand that the alleged desire for absolute scientific certainty is both counterproductive and futile. To wait for certainty is to wait forever.”[28]
Attempting to stave off action using arguments such as, “the effect of this product has not been fully demonstrated,” is an old ruse used by those who would neutralize advances in knowledge they find contrary to their interests. Treating causality as dichotomous was the tobacco industry’s strategy to buy time: tobacco company spokesmen were careful not to deny outright hypotheses about tobacco’s harmful effects, but over and over again, simply insisted that the studies were inconclusive and that further research was necessary to definitively prove cause.
The same fallacy of dichotomous causality also permeates the current CKD debate. A recent news article in El Salvador reported nephrologists criticizing the actions of the Ministry of Health in banning some pesticides, and arguing the need for “conclusive proof” of possible causal agents, chemical by chemical, before taking any action (other than improving detection and treatment).[29]
In summary, the consequences of addressing causality as dichotomous or attributable to isolated agents, not as the result of a multifactorial process that gradually develops, are especially problematic. Public health cannot be held hostage to a sophism conceptually dismantled long ago. Public health authorities are called upon to provide operational closure to the findings of epidemiology, eliminating the gulf that frequently divides knowledge—provided by epidemiology—from preventive intervention, the purview of public health.[30]
Conflicts of interest and manufacturing doubt Powerful interests at stake cannot be ignored as investigations proceed to elucidate the CKDnc epidemic’s causes. We must be vigilant in anticipating potential conflicts of interest that can affect research agendas and interpretation of research results.[31]
The most reprehensible of these conflicts occurs when there are financial connections—and the more hidden, the more serious—between an evaluator or decisionmaker and the companies whose products are under scrutiny. Such cases are a natural breeding ground for ethical breaches.[32,33] Conflicts of interest can be so enveloping that expertise alone is not always immune to its effects. For example, Sir Ronald Fisher, who revolutionized 20th century science with his substantial contributions to biometrics,[34] became entangled in the controversy over the effects of smoking on cancer. While employed by tobacco companies as a consultant, he published an article, several years after Doll and Hill,[35] in which he stated categorically: “There is, in fact, no reasonable ground to associate the secular increase in lung cancer with the increase in smoking as has been done with dramatic eloquence.”[36] Fisher barricaded himself behind the position that “correlation does not guarantee causality.” This argument loses relevance when brandished against those who, far from claiming to contradict it, accompany the necessary condition of correlation with a wealth of solid arguments.
Three facts must be acknowledged, all of which are lessons from history and relate to the CKDnc epidemic. First, the fundamental purpose of corporations is to maximize their profits, which is only natural (and inherent to the logic of the market). But in their efforts to ensure such profits, some companies may unleash powerful forces to boycott research and dissemination of research results. Michaels masterfully documented how industry reacted by discrediting or trying to cover up investigations that one after another were closing in on tobacco, asbestos, lead and other toxic substances.[28] Second, when scientific progress collides with their business expectations, corporations will attempt, at a minimum, to delay the emergence of the truth. Finally, when evidence is the basis for proposed action—whether a law, health program or other sensitive initiative—it can constitute a serious threat to corporate interests.
THE NEED FOR MORE RIGOROUS METHODS
One methodological weakness underlying much of the research into the CKDnc epidemic in Central America is the assumption that if patients have hypertension or diabetes or have used NSAIDs for some time, then the cause of their kidney disease is known. These three conditions are risk factors for CKD, so it is frequently assumed that alternative causal explanations (dehydration, heat stress, pesticides, etc.) should be sought only when none of these factors is present.[1] But persons with any of these conditions can also be subject to additional risks.
The vast majority of the millions of hypertension sufferers, for instance, never develop CKD. At the same time, being hypertensive with CKD does not preclude involvement—occasionally decisive—of other factors harmful to the kidneys. In fact, it is obvious that chronic exposure to pesticides or dehydration is much more likely to produce or hasten CKD progression if, for example, the exposed person is hypertensive or diabetic.[1,29] The argument that such co-factors do not affect diabetics or hypertensives[29] has pernicious methodological implications already apparent in the literature: most of the published studies on CKDnc in Central America fail to emphasize the potential synergy of coexisting hypertension, diabetes, NSAID use and agrochemical exposure.[3–5,14,15]
Another critical weakness that compromises some studies’ validity[4,15] is failure to meet the requirement that a possible cause must have occurred before the supposed effects were produced. The methodological implication is that status with respect to the putative cause must be determined for a time prior to the appearance of its presumed effects; failure to do so is an error that cannot be overcome by simply noting it as a limitation.[37] For example, any model that includes hypertension as a CKDnc causal agent essentially will be invalidated if it fails to consider history of hypertension before disease onset. If, in addition, as in the case of CKDnc, the disease itself can cause hypertension, the problem is even more serious. It is better not to include a variable suffering from this crucial limitation. As noted, mentioning the limitation is not enough, as has been done in some studies,[4] since its effect may be misleading and methodologically disastrous.
Violation of the temporality requirement is even less excusable, if at all, in the case of self report. The question is not what is happening “now,” but rather what happened before the patient fell ill. For instance, in some studies, to determine occupational exposure, current but not previous occupation was recorded,[15] overlooking the possibility of illness leading to a change in work. In such cases, the result would be to blur association between exposure—occupation—and outcome, and therefore any possible contribution of occupation or occupational conditions to the disease.
In summary, to continue progressing in research and in actions to halt the CKDnc epidemic in Central America, we need a model that allows us to rule out controvertible results and rationally integrate valid ones. In fact, “in the final analysis, assessment of evidence and causal inferences depend on accumulating all potentially relevant evidence and making a subjective judgment about the strength of the evidence.”[38] However, we should not stop aspiring to objectivity; biases and preconceptions that work against it are pernicious. Only an integrative model that includes all rigorously obtained knowledge, that properly nuances knowledge displaying discernible methodological limitations, and that, furthermore, dispenses with whatever hinders more than it contributes, will make it possible to produce syntheses that are rational and productive.
Research proposals The search for the causes of CKDnc in Central America demands a broader, more integrated approach, following Pearce’s suggestion: “It has been argued that there has been an overemphasis on aspects of individual lifestyle, and little attention paid to the population-level determinants of health…There is an increasing recognition of the importance of taking a more global approach to epidemiologic research.”[39]
Such an approach demands explanatory studies, without abandoning descriptive ones. Since experiments with human subjects to directly test whether an exposure produces the disease are unacceptable, randomized trials are not an option. But community-based prevention trials are: for example, introducing actions in some communities to prevent pesticide exposure or introducing specific occupational health measures. It is also unreasonable to prioritize longitudinal studies demanding a long time to obtain results. Case-control studies, on the other hand, are badly needed, and none of the studies conducted in the region so far has taken that approach. Such studies could provide important insights into the potential causal roles of the type, intensity and duration of various exposures, whether related to contaminants and environmental pollutants, or to the conditions of work itself. In this context, we cannot stress too strongly the importance of consensus on a clinical and epidemiological case definition.
Epidemiologic surveillance must play a fundamental role. The most immediate and straightforward act would be to create robust registries to provide information on morbidity and mortality, thus enabling estimation of the magnitude, distribution, trends, response to interventions, health care service needs, case survival rates, etc. Studies of specific groups (e.g., children) can be especially informative. To provide useful comparisons, surveillance can be developed in sentinel communities, both high- and low-risk. And surveillance should go beyond just detecting and characterizing the disease; it should also monitor such things as occupational health and safety (working conditions), and governments’ signing and compliance with international agreements on agrochemical use.
Such a pluralistic approach should include qualitative studies to gather opinions of key informants—[40] which would be revealing, in an epidemic with such strong social dimensions—and ecological studies[41] of environmental contamination in communities both affected and relatively unaffected by the epidemic.
As for statistical assessment of associations, it is important, even in studies using multivariate methods, not to limit analysis to significance testing[42] and to avoid its purely ‘ceremonial’ use.[43] To make solid judgments, the reductionism of classical statistics should be complemented by procedures such as counterfactual reasoning,[44] multilevel analysis,[45] Bayesian approximation[46] and approaches associated with directed acyclic graphs.[47]
PUBLIC HEALTH: TAKING THE LEAD
The purpose of this article is not to take a position on either of the hypotheses in play, because they have notable points in common, both containing important plausible elements. However, this article can prove useful insofar as it helps decisionmakers anticipate implications of prioritizing one approach over the other, and, above all, warns against continuing to delay urgently needed health actions to curb the epidemic.
For example, if we steer research toward heat stress and dehydration, investigators will continue on the trail of renal physiology under extreme conditions, the influence of dehydration and the novel role of fructose in producing the disease. This will probably contribute very important scientific knowledge, but above all, it will provide good arguments for improving working conditions to eliminate heat stress and dehydration. These conditions constitute a major determinant that can be modified to protect workers’ health and rights, and, probably, help bring the epidemic under control.
However, if we only follow recommendations suggesting that the primary culprits of the epidemic are heat stress and dehydration, we risk relegating agrochemicals to “medium priority” for further investigation and intervention.[13] This would mean delaying study of the role of agrochemicals, which is unreasonable, given that the alarming magnitude of CKDnc increase over recent years is substantially greater than any demonstrable change in temperature or working conditions. It would also unreasonably postpone necessary regulatory action that, furthermore, all Central American countries have committed to adopting to ensure environmental and human health protection.
The hypothesis that puts agrochemicals front and center is highly plausible, given the documented harmful effects of these products.[48–50] Nevertheless, going forward, it would be imprudent for any research to pose the predominance of agrochemicals as CKDnc causal factors without a methodology designed to promote in-depth investigation into the quite possibly synergistic involvement of suspected co-factors.
Health risks from environmental toxins have been a continuous cause for alarm in developed countries ever since 1962, when Carson’s Silent Spring described the role of pesticides.[51] Also documented are the dangers of agrochemicals and how they are used in the most affected Central American communities ever since cotton growing burgeoned there several decades ago.[18,19]
This hypothesis also gives broader range to public health considerations and action, since it puts more emphasis on determinants that are both social (economic and social vulnerability of entire farming communities) and environmental (use and abuse of agrochemicals with little or no enforcement of existing internationally accepted regulations), with attention also paid to labor rights in the context of occupational health and safety.
Obviously, the agrochemical-centered hypothesis is the most controversial, colliding head-on as it does with the more powerful transnational economic and (hence) political interests, and providing decisionmakers the opportunity to invoke the precautionary principle,[52] which lies at the heart of international commitments adopted at the 1992 UN Conference on Environment and Development (Earth Summit). According to the conference declaration, “In order to protect the environment, the precautionary approach shall be widely applied by States according to their capabilities. Where there are threats of serious or irreversible damage, lack of full scientific certainty shall not be used as a reason for postponing cost-effective measures to prevent environmental degradation.”[53]
The position taken on the CKDnc epidemic also has implications for governments’ and health authorities’ adoption of risk communication strategies to mobilize communities to defend their health and rights. While science proceeds to elucidate disease mechanisms, people in affected communities have a right to know that poverty, agrochemicals and working conditions are high on the list of prime suspects, that there are regulations on the books to protect human health and the environment (including laws on occupational health and safety),[54,55] and that agrochemicals that are prohibited or heavily regulated elsewhere (and in some cases, in their own countries) are still in use in their communities.[56–58] They should also know how to protect themselves and minimize the effects of agrochemicals, and be educated about alternatives to chemical fertilizers and pesticides that can help maintain crop yields while protecting their health.
Finally, the urgent need for a research agenda should be interpreted as an opportunity to develop a comprehensive and holistic theoretical framework that would take into account the economic, political and social context of the epidemic. Such a framework would enable us to distinguish between the causes of the causes (social, economic and environmental determinants), intermediate causes (related to working conditions and behavior) and the proximate causes (physiological mechanisms) of the disease. This would facilitate optimization of both research questions and methods to address them, in order to most effectively and efficiently get to the root of the problem and halt the epidemic.
Disclaimer: Opinions expressed in this article are solely those of the authors and do not reflect the positions of any organization with which they are affiliated.
References

- García R, Aguilar R, Reyes C, Ortiz M, Leiva R. Nefropatía terminal en pacientes de un hospital de referencia en El Salvador. Rev Panam Salud Pública. 2002; 12(3):202–6. Spanish.
- Pan American Health Organization. Resolution CD52.R1. Chronic kidney disease in agricultural communities in Central America [Internet]. Washington, DC: Pan American Health Organization; 2013 [cited 2013 Jun 13]. 2 p. Available from: www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=23222&Itemid=270&lang=en
- Torres C, Aragón A, González M, López I, Jakobsson K, Elinder CG, et al. Decreased kidney function of unknown cause in Nicaragua: a community-based survey. Am J Kidney Dis. 2010 Mar;55(3):485–96.
- Orantes CM, Herrera R, Almaguer M, Brizuela EG, Hernández CE, Bayarre H, et al. Chronic Kidney Disease and associated risk factors in the Bajo Lempa region of El Salvador: Nefrolempa study. MEDICC Rev. 2011 Apr;13(4):14–22.
- Brooks DR, Ramirez O, Amador JJ. CKD in Central America: A hot issue. Am J Kidney Dis. 2012 Apr;59(4):481–4.
- Correa R, Wesseling C, Johnson RJ. CKD of unknown origin in Central America: the case for a Mesoamerican nephropathy. Am J Kidney Dis. 2014 Mar;63(3):506–20.
- Pan American Health Organization [Internet]. Washington, DC: Pan American Health Organization; c2014. Visualizing renal failure and chronic kidney diseases age-standardized mortality rate in countries of the Americas, 2000–2009. Non-communicable Diseases and Mental Health; 2014 [cited 2014 Mar 13]; [about 1 screen]. Available from: http://ais.paho.org/phip/viz/nmh_renalfailure_ckd_visualization.asp
- Institute of Health Metrics and Evaluation 2012. Global Burden of Diseases [Internet]. Seattle: Institute of Health Metric and Evaluation; 2013 Mar [cited 2013 Oct 20]; [about 1 screen]. Available from: http://www.healthmetricsandevaluation.org/gbd/visualizations/gbd-arrow-diagram
- International Consortium of Investigative Journalists [Internet]. Washington, DC: Center for Public Integrity; c2012–2014. Thousands of sugar cane workers die as wealthy nations stall on solutions; 2011 Dec 12 [cited 2014 Mar 14]; [about 5 screens]. Available from: http://www.icij.org/project/island-widows/thousands-sugar-cane-workers-die-wealthy-nations-stall-solutions
- Salinas C. La muerte acecha a los cañeros. Periódico El País (Spain) [Internet]. 2012 Feb 11 [cited 2014 Mar 2]; Portada: [about 3 p.]. Available from: http://internacional.elpais.com/internacional/2012/02/11/actualidad/1328991118_487033.html. Spanish.
- Sheehy K. Mystery kidney disease in Central America. BBC News [Internet]. 2011 Dec 13 [cited 2014 Mar 4]; Home: [about 3 p.]. Available from: http://www.bbc.co.uk/news/magazine-16007129
- Declaración de San Salvador. Abordaje integral de la enfermedad renal túbulo-intersticial crónica de Centroamérica (ERTCC) que afecta predominantemente a las comunidades agrícolas [Internet]. San Salvador: Ministry of Health of El Salvador; 2013 Apr [cited 2014 Mar 2]. 6 p. Available from: http://www.salud.gob.sv/archivos/comunicaciones/archivos_comunicados2013/pdf/Declaracion_San%20Salvador_ERCnT_26042013.pdf. Spanish.
- Wesseling C, Crowe J, Hogstedt C, Jakobsson K, Lucas R, Wegman D, editors. Mesoamerican Nephropathy. Report from the First International Research Workshop on MeN [Internet]. San Jose (CR): SALTRA; 2012 [cited 2014 Mar 2]. 255 p. Available from: http://www.regionalnephropathy.org/wp-content/uploads/2013/04/Technical-Report-for-Website-Final.pdf
- Crowe J, Moya JM, Román B, Robles A. Heat exposure in sugarcane workers in Costa Rica during the non-harvest season. Glob Health Action. 2010 Nov 29;3.
- Peraza S, Wesseling C, Aragon A, Leiva R, García RA, Torres C, et al. Decreased kidney function among agricultural workers in El Salvador. Am J Kidney Dis. 2012 Apr;59(4):531–40.
- Crowe J, Wesseling C, Solano BR, Umaña MP, Ramírez AR, Kjellstrom T, et al. Heat exposure in sugarcane harvesters in Costa Rica. Am J Ind Med. 2013 Oct;56(10):1157–64.
- Roncal CA, Ishimoto T, Lanaspa MA, Rivard CJ, Nakagawa T, Ejaz AA, et al. Fructokinase activity mediates dehydration-induced renal injury. Kidney Int. 2013 Dec 11. doi: 10.1038/ki.2013.492. [Epub ahead of print]
- Aragón A, Aragón C, Thörn Å. Pests, peasants, and pesticides on the Northern Nicaraguan Pacific Plain. Int J Occup Environl Health. 2001 Oct–Dec;7(4):295–302.
- McConnell R, Pacheco AF, Magnotti R. Crop duster aviation mechanics: high risk for pesticide poisoning. Am J Public Health. 1990 Oct:80(10):1236–9.
- Morgan DP, Roan CC. Renal function in persons occupationally exposed to pesticides. Arch Environ Health. 1969 Nov;19(5):633–6.
- Jayatilake N, Mendis S, Maheepala P, Mehta FR; CKDu National Research Project Team. Chronic kidney disease of uncertain aetiology: prevalence and causative factors in a developing country. BMC Nephrol. 2013 Aug 27;14:180.
- Jayasumana MACS, Paranagama PA, Amarasinghe MD, Wijewardane KMRC, Dahanayake KS, Fonseka SI, et al. Posible link of chronic arsenic toxicity with chronic kidney disease of unknown etiology in Sri Lanka. J Nat Sci Res. 2013;3(1):64–73.
- Ferraro PM, Costanzi S, Naticchia A, Sturniolo A, Gambaro G. Low level exposure to cadmium increases the risk of chronic kidney disease: analysis of the NHANES 1999–2006. BMC Public Health. 2010 Jun 3;10:304.
- Botti C, Comba P, Forastiere F, Settimi L. Causal inference in environmental epidemiology: the role of implicit values. Sci Total Environ. 1996; 84:97–101.
- Morabia A, editor. Epidemiology: an epistemological perspective. In: A history of epidemiologic methods and concepts. Basel (CH): BirkhauserVerlag; 2004.
- Hill AB. The environment and disease. Association or causation? Proc R Soc Med. 1965 May;58(5):295–300.
- Grimes DA, Schulz KF. Bias and causal associations in observational research. Lancet. 2002 Jan 19;359(9302):248–52.
- Michaels D. Doubt is their product. How industry’s assault on science threatens your health. Oxford: Oxford University Press; 2008 May. 388 p.
- Ramírez M. Nefrólogos no apoyan tesis de tóxicos y mal renal. Estudios sobre exposición de pesticidas no han encontrado relación entre los tóxicos con la insuficiencia renal crónica. Periódico El diario de hoy (San Salvador). 2013 Aug 29. Spanish.
- Rodríguez CA. La salud de los trabajadores: entre la ciencia y la ética. Salud Colectiva. 2013;9(2):133–7. Spanish.
- Smith R. Conflict of interest and the BMJ. Time to take it more seriously. Br Med J. 1994; 308 (6920):4–5.
- Angell M. The truth about the drug companies: how they deceive us and what to do about it. New York: Random House; 2005 Aug 9. 319 p.
- Gøtzsche PC. Deadly medicines and organized crime: how big pharma has corrupted healthcare. London: Radclife Medical Press; 2013 Aug 31. 310 p.
- Salsburg D. The lady tasting tea: how statistics revolutionized science in the twentieth century. New York: Henry Holt & Co.; 2002 May. p. 38.
- Doll RA, Hill AB. Smoking and carcinoma of the lung: preliminary report. Br Med J. 1950 Sep 30;2(4682):739–48.
- Fisher RA. Cigarettes, cancer and statistics. Centen Rev. 1958;2:151–66.
- Silva LC, Benavides A. Causalidad e inobservancia de la premisa de precedencia temporal. Revista Metodológica. 1999;7:1–14. Spanish.
- Kassirer JP, Cecil JS. Inconsistency in evidentiary standards for medical testimony: disorder in the courts. JAMA. 2002 Sep 18;288(11):1382–7.
- Pearce NA. Short Introduction to Epidemiology. Occasional Report Series No 2. Wellington (NZ): Centre for Public Health Research Massey University; 2003. 130 p.
- Denzin NK, Lincoln YS. Handbook of qualitative research. 2nd ed. London: Sage; 2000 Mar 18. 1143 p.
- Morgenstern H. Ecologic studies in epidemiology: concepts, principles, and methods. Ann Rev Public Health. 1995;16:61–81.
- Nuzzo R. P values, the ‘gold standard’ of statistical validity, are not as reliable as many scientists assume. Nature. 2014 Feb 12;506(7487):150–2.
- Silva LC. Una ceremonia estadística para identificar factores de riesgo. Revista Salud Colectiva. 2005;1(3):309–22. Spanish.
- Höfler M. Causal inference based on counterfactuals. BMC Med Res Methodol. 2005 Sep 13;5:28.
- Diez AV. Next steps in understanding the multilevel determinants of health. J Epidemiol Community Health. 2008 Nov;62(11):957–9.
- Williamson J. Bayesian nets and causality. Philosophical and Computational Foundations. Oxford: Oxford University Press; 2005 Feb 24. 250 p.
- Shrier I, Platt RW. Reducing bias through directed acyclic graphs. BMC Med Res Methodol. 2008 Oct 30;8:70.
- Kaur B, Khera A, Sandhir R. Attenuation of cellular antioxidant defense mechanisms in kidney of rats intoxicated with carbofuran. J Biochem Mol Toxicol. 2012 Oct;26(10):393–8.
- Li Q, Peng X, Yang H, Wang H, Shu Y. Deficiency of multidrug and toxin extrusion 1 enhances renal accumulation of Paraquat and deteriorates kidney injury in mice. Mol Pharm. 2011 Dec 5;8(6):2476–83.
- Siddharth M, Datta SK, Bansal S, Mustafa M, Banerjee BD, Kalra OP, et al. Study on organochlorine pesticide levels in chronic kidney disease patients: association with estimated glomerular filtration rate and oxidative stress. J Biochem Mol Toxicol. 2012 Jun;26(6):241–7.
- Carson R. Silent Spring. Boston: Houghton Mifflin; 1962.
- Raffensperger C, Tickner J, editors. Public health and the environment: implementing the precautionary principle. Washington, DC: Island Press; 1999.
- United Nations Environment Program. Agenda 21, Rio Declaration on environment and development, and the statement of principles for the sustainable management of forests. United Nations Conference on Environment and Development (UNCED) [Internet]. Rio de Janeiro: United Nations Environment Program; 1992 Jun [cited 2014 Feb 6]; [about 4 p.]. Available from: http://www.unep.org/Documents.Multilingual/Default.asp?documentid=78&articleid=1163
- Stockholm Convention [Internet]. Stockholm: Secretariat of Stockholm Convention; c2008 [cited 2014 Feb 6]. Available from: http://chm.pops.int/Countries/StatusofRatifications/PartiesandSignatories/tabid/252/Default.aspx
- Rosenthal E. Who’s afraid of national laws? Pesticide corporations use trade negotiations to avoid bans and undercut public health protections in Central America. Int J Occup Environ Health. 2005 Oct–Dec;11(4):437–43.
- Wesseling C, Corriols M, Bravo V. Acute pesticide poisoning and pesticide registration in Central America. Toxicol Appl Pharmacol. 2005 Sep 1;207(2 Suppl):S697–705.
- Bravo V, Rodríguez T, van Wendel de Joode B, Canto N, Calderón GR, Turcios M, et al. Monitoring pesticide use and associated health hazards in Central America. Int J Occup Environ Health. 2011 Jul–Sep;17(3):258–69.
- elfaro.net [Internet]. San Salvador: elfaro; 2014. Entre los 11 pesticidas por los que aboga Funes hay nefrotóxicos y cancerígenos; 2013 Dec 9 [cited 2014 Mar 6]; [about 4 p.]. Available from: http://www.elfaro.net/es/201312/noticias/14070/. Spanish.
THE AUTHORS
Luis Carlos Silva Ayçaguer Corresponding author: lcsilva@infomed.sld.cu), mathematician and biostatistician. Full professor and senior researcher, National Medical Sciences Information Center, Havana, Cuba.
Pedro Ordúñez García, nternist specializing in public health with a doctorate in health sciences, Department of noncommunicable diseases and mental health, PAHO, Washington, DC, USA.
Submitted: November 8, 2013 Approved: March 23, 2014 Disclosures: None