ABSTRACT
Introduction Early screening for hearing loss is currently recognized as an international healthcare standard. In Cuba, such a program was initiated in the capital, Havana, in 1983 and scaled up to national coverage in 1991.
Objective Review the development of Cuba’s national hearing screening program over the last 25 years (organizational structure, efficiency, coverage and impact on health), and the science and technology developed to sustain it.
Intervention The program was organized in two steps: Step 1-clinical selection of children at different stages of development with multiple high-risk registers; Step 2-referral to territorial, hospitalbased centers for auditory brainstem evoked response (ABR) testing, diagnostic evaluation, and intervention. Prior to national scaling-up, the efficiency of this multiple targeted screening (MTS) protocol was evaluated in Havana. Technology and equipment were then developed, and personnel were trained to set up the national screening network. In 1996, the multiple auditory steady-state evoked response (MSSR) technique for objective audiogram estimation was introduced using AUDIX equipment, designed and produced in Cuba for this program. A semi-automated version for neonatal screening has been developed more recently. Several studies have been conducted to evaluate the program’s efficiency, coverage, yield, and impact on health.
Results During the first stage of implementation in Havana, the MTS protocol correctly identified 72.5% of children with congenital and preverbal hearing loss. Subsequent studies of different aspects of the program have shown that: 1) the mean age of hearing loss detection/ intervention in one municipality was reduced from 4 years to 10 months; 2) hearing-impaired children who were screened showed improved language and cognitive development compared to those who were not screened; 3) the MSSR technique predicted type and severity of hearing loss more accurately than physiological techniques used previously and was also shown to be an effective screening method (92% to 96% sensitivity, 100% specificity); and 4) program coverage (25-86%), though reasonably high in some regions, is not complete and needs improvement, particularly in the country’s remote and rural areas.
Conclusions The MTS protocol can be considered a valid option for increasing the yield and effectiveness of a hearing screening program operating with limited resources. The MSSR technique provides valuable data for the diagnosis and treatment of children detected through a screening program and, with improvements, may also be useful as a screening method.
Keywords Early intervention, hearing screening, auditory evoked response, evoked potentials, hearing loss, deafness, neonatal screening
INTRODUCTION
Childhood hearing loss is a major health problem worldwide: 1-3 per 1,000 children are born with significant bilateral hearing impairment, and up to 1-3 per 100 children will have mild or moderate hearing loss.[1,2] Additionally, about 30 per 10,000 children will develop a hearing impairment within the first few years of life. [3] The incidence of hearing disorders among high-risk children is 10-14 times greater than that reported for the general population. High-risk children are defined using internationally recommended pre-, peri- and post-natal clinical factors, or through non-specific criteria, such as discharge from an intensive care unit (ICU).[4] In Cuba, the 2000-2003 National Disability Study identified 23,620 hearing-impaired persons, showing a prevalence of 2.1 per 1,000 population, which lies within the range reported internationally.[5] Other studies have confirmed that in Cuba incidence of significant hearing problems among high-risk infants and children (1-5 per 100 children) is higher than in the general population.[6-8]
Total or partial hearing loss at birth or during the first years of life, if unidentified and untreated, has devastating effects on child development. Biologically, there are changes in brain structure, multimodal sensory integration and hemispheric lateralization.[9,10] Psychologically, speech and language do not develop as rapidly or normally as they should. This retards normal intellectual development, creates learning problems, and produces emotional and behavioral problems that impede the child’s adequate adaptation to family and social environments.[11]
These negative effects can be prevented if hearing loss is detected early and appropriate intervention initiated during the first six months of life.[12,13] This requires a comprehensive early screening program that ensures not only initial detection but also follow-up and timely intervention of infants identified.[4] Reports from developed countries show that, in the absence of such a program, the most severe hearing losses are detected late (average age 20-24 months), while mild and moderate disorders are not detected until much later (age ≥4 years).[3] When the opportunity for early intervention-during the years when the brain is most receptive to language acquisition-is missed, treatment and/or rehabilitation is much less effective.[4]
In recent decades, infant hearing screening has been increasingly recognized as a standard of health care worldwide. As a result, many developing countries are adopting legislation to address this issue and taking actions to implement programs for early detection of hearing loss.[14] However, no single screening protocol is the most effective in all situations. In order to guarantee all the necessary components (early detection, diagnosis, and timely intervention), screening protocols must be tailored to fit local health care systems and available resources in each country. Periodic monitoring and evaluation are also needed to ensure continued renovation and improvements in the program.[8,14,15-17]
Several aspects should be taken into account when setting up a screening program, beginning with the choice of appropriate diagnostic tools. The best screening equipment should combine ease of operation, low cost, and high diagnostic efficiency.[ 8] At present, there are valid and reliable methods for identifying hearing problems at birth, which measure specific physiological responses to an acoustic stimulus.[4] The most commonly used are Auditory Brainstem Evoked Responses (ABR), first described in humans in 1970,[18] and Otoacoustic Emissions (OAE), first described in 1978.[19] ABR measurements are obtained from surface electrodes that record neural activity generated in the cochlea or receptor, auditory nerve, and brainstem in response to brief acoustic stimuli delivered via an earphone. This method efficiently detects most cochlear and retrocochlear hearing loss but is less successful detecting mid- and low-frequency hearing impairment.[8] OAEs are obtained from the ear canal using a probe with attached microphone to register cochlear responses to an acoustic stimulus. This measurement reflects the state of the peripheral auditory system but does not detect damage in the neural pathway. Long-term follow-up studies have shown that both methods are quite effective-detecting ≥80% of congenital hearing loss- but this can still be improved.[20]
A screening program must also provide appropriate audiological and medical evaluations for all children who do not pass initial hearing screening and a subsequent confirmation test. This requires a battery of tests, including physiological methods (electric response audiometry) and, when developmentally appropriate, behavioral methods. Since behavioral audiometry is neither accurate nor reliable in infants, physiological measures should be used to estimate residual hearing sensitivity across the speech frequency range, determine the type of hearing loss, and provide information needed to initiate hearing aid fitting. Tone pip ABR has proved to be an effective procedure but with limitations that prevent it from becoming more widely used.[21] More recently, auditory steady-state response (ASSR) audiometry has emerged as a promising method for objectively determining frequency-specific thresholds and is currently a major focus of pediatric audiology research.[14]
Finally, the screening program’s yield and impact on health also depend on the organizational model or protocol adopted. The first hospital-based programs using physiological methods were set up in the late 1970s and early 1980s, and screened only newborns at risk.[22- 24] Given the high cost of this technology at the time, along with the need for trained experts to interpret the ABR test results, these programs targeted for screening those newborns at highest risk of hearing loss. However, the yield of such programs is limited, since about half of the infants with congenital hearing impairment do not present identifiable risk factors.[2] Rapid technological advances over the last decade have produced a variety of low-cost automated devices that are easy to operate with minimal training, providing pass/fail results within minutes. This has facilitated the transition to the more efficient universal neonatal hearing screening protocols (UNHS) currently recommended.[14]
Nevertheless, implementation of UNHS poses new challenges. [15,16] As the number of screenings increases to include all newborns, so do the number of referrals for diagnosis (1-5% of those screened) and the proportion of false positives. The higher over-referral rate makes follow-up more difficult, demands more audiological resources, and may have a negative impact on the families of normal-hearing children who fail initial screening. It is estimated that for every hearing-impaired child correctly identified through targeted neonatal screening, six are referred unnecessarily. With UNHS, the proportion of over-referrals is much higher (100 for each hearing-impaired child detected).[2] Therefore, it has been recommended that UNHS be implemented with caution, particularly in developing countries where resources are limited. Some authors have recommended that transition to UNHS be made only after a high-risk targeted screening program has been in place and can serve as the starting point for developing the necessary professional skills and services to ensure early diagnosis and intervention of all cases detected.[16]
INTERVENTION
Cuba’s Hearing Screening Program began in 1983 with an original development strategy, organizational model, and technological resources-the product of “closed loop” research through which scientific findings and technological developments are part of a combined effort to solve a specific health problem. The program was organized to be incorporated into the existing healthcare system and make the most efficient use of limited resources. A two-step screening model was adopted and initially implemented in Havana. Following an outcome evaluation and preparation of additional human and technological resources, a national hearing screening program was established in 1991.
Two-step multiple targeted screening model (Figure 1): In Step 1, children at different stages of development are clinically selected using multiple high risk registers. Groups targeted for Step 2 screening include newborns identified at maternity hospitals as well as children aged ≤3 years who are referred from Intensive Care Units (ICU), primary health care units, or family doctors. Referral criteria are shown in Table 1. The existence of at least one risk factor is considered sufficient grounds for referral to screening.
Figure 1: Two-Step Multiple Targeted Hearing Screening Model Implemented in Cuba

Table 1: Risk Criteria for Referring Children Aged 0-3 Years for Hearing Screening

*TORCH: Toxoplasmosis, Rubella, Cytomegalovirus, Herpes
For Step 2, diagnostic equipment and skilled professional teams were distributed in territorial hospital-based reference centers. Currently, there are 17 such centers across the country: four in Havana and one in each of the other 13 provinces. Each reference center provides early detection, diagnostic and intervention services for the population of a large geographic area, and receives an average of 1,000 to 1,500 children per year. These centers also provide open referral services any time a doctor or parent is concerned about a child’s hearing or language abilities.[8]
Children at risk and targeted in Step 1 are referred to the nearest reference center for electric response audiometry (ABR or, more recently, ASSR) testing at age ≥3 months. Parental informed consent is obtained, and the test is performed while the child is asleep or under mild sedation if necessary. Specialist teams at the reference centers include an audiologist, neurophysiologist, and speech therapist, plus technicians in various fields. Testing equipment and methods have all been developed and/or standardized in Cuba, thus guaranteeing the program’s consistent implementation throughout the country.
Children who fail initial screening undergo further testing (threshold-seeking audiometry), and those with a confirmed hearing loss are then evaluated by the multidisciplinary team, which makes a diagnosis and prescribes appropriate treatment (medical, hearing aids, and/or surgery). The reference center provides intervention services and systematic follow-up evaluations by audiologists and other specialists if required, as well as parent counseling and psychometric monitoring of each child’s development. Language (re)habilitation and early stimulation for children aged ≤18 months is done basically by parents with periodic follow-ups at the reference center. Parents are supplied with early stimulation programs that have been adapted and/ or designed in Cuba by specialists from various institutions.[25] All hearing-impaired children are also seen by specialists at one of the Ministry of Education’s Diagnosis and Orientation Centers, and they receive specialized services upon entering child care centers or school.
Hearing screening technology developed in Cuba (Figure 2): Since the early 1970s, the Cuban Neuroscience Center has been developing neurodiagnostic equipment with specialized hardware and software for quantitative analysis and interpretation of brain responses. The first quantitative evoked response and electroencephalogram equipment, MEDICID, was manufactured in 1972 in collaboration with the Central Institute for Digital Research (ICID). In 1985, the NEURONICA 02 multimodal evoked response testing equipment became the foundation for national scaling-up of the hearing screening program.[26]
Several innovative procedures for acquiring, analyzing and interpreting evoked responses were included in the diagnostic software developed at the same time. These procedures included various signal-noise statistical indicators used to assess recording quality and to quantitatively aid response detection;[27,28] normative ABR maturation data for Cuban infants and children, and methods for automatic comparison with these databases;[29] and development of an Expert System for Audiological Diagnosis (SEDA) which showed, upon validation, a close correspondence between clinical and automated diagnoses (Kappa Index, 0.83).[30]
The technology initially developed in Cuba, using click ABR as a diagnostic tool, sustained the program for more than 15 years. The efficiency of this equipment is confirmed by the reliability of the results obtained,[6-8] which are consistent with those reported in similar international studies involving highrisk targeted screening.[22-24] Research continued, however, to find an objective method that could more precisely evaluate residual hearing and also determine hearing sensitivity thresholds at different audiometric frequencies (pure-tone audiogram estimation). Although click ABR tests can effectively detect most (high frequency) hearing disorders in young children, due to the acoustic properties of the brief stimulus used and the physiological mechanisms underlying the response generation, this technique misses some mid-to-low-frequency hearing losses. [24] Tone pip ABR is currently recommended as the method of choice for pure-tone audiogram estimation,[14] but it is very time-consuming because each audiometric frequency and each ear has to be tested separately. Moreover, since these responses are more difficult to identify, the accuracy of threshold determination is critically dependent on the expertise of the person evaluating the recordings by visual inspection. This is likely the reason why tone pip ABR audiometry is not widely used, even in developed countries. In Cuba, it was intensively studied from 1985 to 1989;[31] several stimulation and noise masking techniques for frequency-specific audiometry with ABR were implemented using the NEURONICA 02 equipment, and some statistical methods were introduced for automated detection of these responses, but the method was never effectively placed in the screening network.[28,31]
Figure 2: Evoked Response Testing Equipment Developed in Cuba for Hearing Screening
 In the last decade, auditory steady-state response (ASSR) audiometry has emerged as a valid technique for rapid and objective pure-tone audiogram estimation in young children.[32-34] ASSRs are periodic, quasi-sinusoidal responses evoked by various auditory tones presented simultaneously at specific stimulation rates. This technique shares some of the advantages of ABR testing: for example, it is not affected by sleep or sedation, and responses are detectable down to intensities near the hearing threshold.[35] In other respects, its advantages outweigh those of ABR: ASSRs can be evoked by continuous frequency-specific auditory stimuli (typically amplitude and/or frequency-modulated tones) with better acoustic properties than the brief stimuli used for ABR audiometry. ASSR measurement is also very simple and can be automatically calculated by a computer, eliminating the need for an expert interpreter to visually identify each response. Various statistical procedures can be used to efficiently determine whether a response is present or not.[36]
In the last decade, auditory steady-state response (ASSR) audiometry has emerged as a valid technique for rapid and objective pure-tone audiogram estimation in young children.[32-34] ASSRs are periodic, quasi-sinusoidal responses evoked by various auditory tones presented simultaneously at specific stimulation rates. This technique shares some of the advantages of ABR testing: for example, it is not affected by sleep or sedation, and responses are detectable down to intensities near the hearing threshold.[35] In other respects, its advantages outweigh those of ABR: ASSRs can be evoked by continuous frequency-specific auditory stimuli (typically amplitude and/or frequency-modulated tones) with better acoustic properties than the brief stimuli used for ABR audiometry. ASSR measurement is also very simple and can be automatically calculated by a computer, eliminating the need for an expert interpreter to visually identify each response. Various statistical procedures can be used to efficiently determine whether a response is present or not.[36]
The main advantage of this technique, however, is that several modulated tones can be mixed together and presented simultaneously to elicit multiple auditory steady-state responses (MSSR). [37,38] If each tone in the mixed stimuli is modulated at a different rate, each evoked response can be assessed independently. Each carrier tone activates the frequency-specific region of the cochlea or auditory receptor where that particular tone is codified. Using a mathematical procedure such as Fast Fourier Transform (FFT), each steady-state response is represented by a spectral peak at the modulation frequency of the auditory tone that evokes it (Figure 3). In other words, the modulation acts like a label or signature by which each frequency-specific response can be recognized in the FFT-measured activity. The MSSR technique can therefore decrease the duration of audiometric testing by simultaneously determining several frequency-specific thresholds in both ears at the same time. According to our results, complete MSSR audiometric testing to determine hearing thresholds at 0.5, 1, 2 and 4 kHz in both ears may be completed in approximately 35-40 minutes in normal-hearing subjects.[38]
Given the MSSR technique’s potential, the decision was made to analyze its usefulness in the Cuban screening program. Since the NEURONICA 02 equipment had been designed with a wide range of acoustic stimulation possibilities and used a digitally programmable stimulus generator, it served to develop an MSSR recording system prototype (hardware and software), which enabled Cuban participation in the first clinical validation study of this methodology in 1996, in collaboration with the Canadian team led by Professor Terence W. Picton.[32,37]
RESULTS
Pérez Abalo et al. analyzed the program’s effectiveness, coverage and impact on health in a 20-year retrospective study published in 2005.[8] The present review refers to results of that study and also includes more recent data on the program’s yield and coverage, updates results obtained using MSSR audiometry, and describes new equipment developed to introduce the MSSR technique in the screening network. Evaluation of the hearing screening program in Havana: Before the program was scaled up nationally, a retrospective cohort study of children screened between 1986 and 1988 was carried out to assess the diagnostic efficiency and coverage of the program in Havana.[8] A behavioral pure-tone audiometry obtained when each child was old enough to cooperate reliably was used as the gold standard to determine the child’s actual hearing status. The number of hearing-impaired children detected through screening was obtained from the centralized database of the Havana Hearing Screening Program. A second, independent estimate of the number of hearing-impaired children born in the city during the same period (1986-1988) was obtained by reviewing the medical charts of special education schools for the hearing impaired, and the archives of the Ministry of Education’s Diagnosis and Orientation Centers. Statistical data provided by the Cuban Ministry of Public Health were used to estimate the total number of live births and the high-risk population in Havana.
Because the two-step model involves two co-dependent diagnostic decisions (presence of high-risk criteria and results of the ABR test), a new variant of the Receiver Operating Characteristic Curves (ROC) method was developed by researchers at the Cuban Neuroscience Center to evaluate the program’s diagnostic efficiency.[ 39] Results showed that the MTS protocol correctly identified 72.5% of children with congenital and preverbal hearing loss in Havana, with a relatively small proportion of false positives,[8] which is higher than the 50% to 62% reported for neonatal targeted screening alone.[40] The study concluded that this 16.3% increase in overall diagnostic efficiency may have been attributed to targeting other groups of high-risk children aged <3 years, which allowed for the detection of late onset and/or preverbal acquired hearing losses. These results support the MTS model and are consistent with the Joint Committee on Infant Hearing’s recent guidelines on the need to screen children at other ages, even with UNHS operating in maternity hospitals.[14]
Figure 3: Multiple Auditory Steady-State Evoked Response (MSSR) Technique
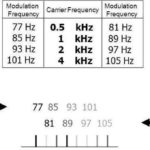 Simultaneous testing of audiometric thresholds at 0.5, 1, 2 and 4 kHz. A complex acoustic signal comprised of four amplitude-modulated carrier tones of 0.5, 1, 2 and 4 kHz mixed together is presented to each ear. Distinct modulation frequencies for each tone and each ear are used. Left ear tones were modulated at 77, 85, 93 and 101, and right ear tones at 81, 89, 97 and 105. The FFT recording shows the MSSR as eight spectral peaks at each of the modulation frequencies used for the different tones. Each spectral peak represents the frequency-specific steady-state response evoked by activation of the carrier tone modulated at that frequency.
Simultaneous testing of audiometric thresholds at 0.5, 1, 2 and 4 kHz. A complex acoustic signal comprised of four amplitude-modulated carrier tones of 0.5, 1, 2 and 4 kHz mixed together is presented to each ear. Distinct modulation frequencies for each tone and each ear are used. Left ear tones were modulated at 77, 85, 93 and 101, and right ear tones at 81, 89, 97 and 105. The FFT recording shows the MSSR as eight spectral peaks at each of the modulation frequencies used for the different tones. Each spectral peak represents the frequency-specific steady-state response evoked by activation of the carrier tone modulated at that frequency.
Analysis of the National Hearing Screening Program’s yield and coverage: In 2005, a retrospective analysis of the program’s yield and coverage was carried out in five representative provinces. The reference centers in each province reported annual statistical data for a three-year period on the population screened annually, the proportion screened relative to the total child population in the province, and the number detected with hearing loss. Results showed that 9-10 per 100 children screened had some type of hearing loss, and about one-third of these had severe bilateral hearing impairments (Table 2). Total incidence was comparable to the 5-15% incidence (10% average) reported in the international literature.[40,41]
As Table 2 shows, program coverage was uneven in the provinces analyzed, ranging from <50% at-risk children screened in Las Tunas and Villa Clara to >80% coverage in Havana City. The lowest coverage was found in sparsely-populated rural areas. In the provinces with low screening coverage, however, the incidence of hearing loss was relatively high and comparable to that reported in other provinces with better coverage. It is difficult to tell if these figures are overestimated or if they reflect local differences in population characteristics. Clinical genetic research carried out as part of the 2001-2003 National Disability Study found regional differences in the incidence of genetic mental retardation, consanguinity index and alcohol intake during pregnancy, all of which might also increase the probability of other neurological development problems, including hearing loss.[42] The consanguinity index, for example, was relatively higher in Las Tunas province, and mental retardation prevalence was relatively higher in parts of Villa Clara and Las Tunas provinces. Further studies are needed to clarify these issues.
Impact of the hearing screening program on health: The main goal of a hearing screening program is to effectively prevent disability and ensure the optimum development of all children with early hearing loss. Two studies have been conducted to assess the impact of the program on child development. The first, in 1991, examined a convenience sample of 35 children aged 6-9 years who attended the Lina Odena Special Education School for hearing-impaired children in Havana. A Cuban-standardized psychometric test of basic learning skills was applied to assess their language and cognitive development, and to evaluate the correlation between test scores (mental coefficient) and age at hearing loss detection (Figure 4).[43]
Table 2: Hearing Screening Program Coverage and Incidence of Hearing Disorders in Children at Risk in Five Cuban Provinces, 1998 to 2000

SBSN: Severe bilateral sensorineural hearing loss
NR: Not reported
*Source: Cuban Ministry of Public Health
Figure 4: Correlation Between Hearing Loss Detection/Intervention Age and Cognitive Development

* The mental age coefficient (vertical axis) is calculated as the difference between the child’s mental age as scored by the psychometric test[13] and his/her chronological age. Source: Reigosa V, et al. Revista CENIC/Ciencias Biológicas 2002;33:99-105. User with permission.
The strong correlation found between the cognitive development (mental age) of children with hearing loss and the mean detection/intervention age indicates that early detection of hearing loss by the screening program in children as young as three months improved their cognitive development. Although few children in the study had normal cognitive development (mental age equal to or above their chronological age), those who did were precisely the children who had received early, effective intervention.
A second, more epidemiologically significant study was carried out as part of the 2001-2003 National Disability Study.[5] Through home visits, a family physician and a speech therapist identified a total of 199 hearing-impaired persons (2.4 per 1000 population) in Cotorro Municipality on the outskirts of Havana. All responded to a structured interview created specifically for the study, and they were also given language and cognitive development tests. To assess the comparative impact of the screening program on several health indicators, two groups of subjects were constructed: (1) Screened (n=23), all hearing-impaired persons in the municipality who were born after the screening program had been put in place (November 1983 to September 2000); and (2) Not screened (n=29), all those born between 1970 and 1983.
It may be assumed that both groups had equal access to free health care and education, so possible differences would be mostly attributable to implementation of the screening program. Effects of the screening program on the detection/intervention age and on other measures of psychosocial development, such as cognitive test scores, progress at school, language skills and self-esteem were compared. (Tables 3 and 4).[8]
These results indicate that even in a periurban community, the hearing screening program made a positive impact on health by reducing the mean age of hearing loss detection/intervention and benefiting the child’s overall development. As Table 4 shows, psychosocial development scores were higher among the screened group. The most striking differences between the groups were in their language development and self-esteem scores. Although all subjects (screened and not screened) showed certain retardation in language development, this was most severe in subjects who were not screened (all subjects in this group showed language development >10 years below the expected level for their chronological age).[8]
Table 3: Effect of the Hearing Screening Program on Mean Detection/Intervention Age

*The screened group was divided into two periods: before and after the economic crisis of the 1990s.
Table 4: Long-term Effects of the Hearing Screening Program on Psychosocial Development

It should be noted that when the screening program was functioning optimally (1983-1991), the mean age for hearing loss detection was reduced from 4 years to 10 months. Unfortunately, it increased to 21 months during the economic crisis of the early 1990s. Lack of transportation during that time may be one factor affecting this indicator, since it was more difficult for people to reach the reference centers for screening.
Evaluation of the MSSR technique: The role and potential utility of the MSSR technique in hearing screening is currently a topic of much research and scientific debate that is beyond the scope of this article.[33,34,37,44,45] In Cuba, however, several studies have been conducted to evaluate this technology and its potential use in the Cuban hearing screening program.[46,47,48-50] The first of these efforts was the 2000-2001 maturation study that examined a representative sample of risk-free newborns and infants to define changes in the MSSR during the first year of life.[48] It was found that different frequency responses were detectable at intensity levels near the hearing threshold from birth, providing the first normative MSSR data (amplitude and detectability) for children in that age range. This corroborates previous findings at early ages with single tone ASSR.[33,34] Similar results using MSSR with normal-hearing newborns have been reported more recently by other authors.[44]
A second long-term clinical follow-up study (2001 to 2004) examined the predictive value of MSSR audiometry for young children and its diagnostic efficiency as a screening method.[46] The study evaluated 513 children who presented high risk factors as infants and were screened at age 3 months using click ABR and MSSR. All those who failed the initial screening test were given a more detailed electric response audiometry confirmation test using both techniques and were followed up periodically by the multidisciplinary team. At age 3-4 years, when the children in the sample were old enough to provide a reliable behavioral response, conventional tone audiometry was performed, and the results of this test were compared with the results of the objective click ABR and MSSR tests performed at age 3 months. The MSSR technique was found to adequately predict pure-tone audiogram configuration and severity of hearing loss, and to predict these more accurately than click ABR, particularly at low frequencies (<2 kHz). The same study also evaluated the diagnostic efficiency of MSSR as a screening method compared to click ABR. For the MSSR screening test, two amplitude modulated tones (0.5 and 2 kHz) were simultaneously presented at a fixed intensity near the hearing threshold. Both methods (click ABR and MSSR) proved highly effective for screening, showing comparable sensitivity and a diagnostic specificity of 100% and 92%, respectively. However, MSSR also identified a newborn with possible hearing loss at predominantly low frequencies who passed the click ABR test. This infant did not appear for final audiometric follow-up and therefore was not included in the diagnostic efficiency analysis.
The fact that the MSSR technique’s diagnostic efficacy is similar to that of an already established method like click ABR supports its use for early detection of hearing disorders in very young atrisk children. Moreover, the possibility of identifying disorders at middle and low frequencies that are not detected by click ABR is a potential advantage of MSSR that should be corroborated by further research. In addition, a study using the ROC curves method showed that automated detection of the threshold response was more efficient with MSSR than with click ABR.[49]
These favorable results served as a basis for continued improvement of the MSSR technique and equipment, with the goal of introducing it for UNHS in maternity hospitals. New types of stimulation have been developed, and recording analysis and processing methods were optimized to make MSSR testing quicker and more efficient. A new software application called BABY SCREEN is already available and included with the AUDIX 5 equipment.[47,50] Preliminary evaluation of this software was conducted with a group of 50 risk-free newborns found to have normal hearing thresholds according to a previous click ABR test. Each infant was screened at the maternity hospital using MSSR and the BABY SCREEN system. In each case, one recording was made with no stimuli to simulate deafness. Results show that duration of the MSSR test could be reduced to 2.6±1.2 minutes on average while preserving adequate diagnostic efficiency (100% sensitivity, 96% specificity), equivalent to that previously reported in at-risk infants.[46] The system did not produce any false negatives (all recordings without stimuli were correctly classified positive), and there were only four recordings with stimuli (4%) in which MSSR was not detected and that were considered false positives. Research continues toward achieving more effective use of MSSR for UNHS, and new forms of stimulation and automated equipment are being developed to that end.
CONCLUSIONS
The two-step targeted screening model employed in Cuba’s hearing screening program for the last 25 years has proved to be a valid, resource-efficient method for the early detection and intervention of children with hearing impairment. Cuba’s hearing screening program was designed to take full advantage of available technical and professional resources, and conditions were created to provide effective follow-up and intervention of identified cases. Studies have shown that, under optimum operating conditions, the National Hearing Screening Program has had a positive impact on health by significantly lowering the mean detection/ intervention age and thereby improving the psychosocial development of screened children with detected hearing loss. Nevertheless, the protocol should be improved and expanded to provide UNHS in maternity hospitals and to guarantee full coverage in all communities, particularly in rural areas.
Results obtained using the MSSR technique and the successive generations of AUDIX equipment over the last decade validate their use for pure-tone audiogram estimation at the most important speech frequencies (0.5-4 kHz) and for providing valuable data for diagnosing and treating cases identified through the screening program. Applied as a screening method, the MSSR technique also proved effective for testing at-risk infants and children aged ≥3 months, and, with improvement, may be useful for UNHS in maternity hospitals.
Close cooperation between Cuba’s scientific research institutions, public health and education systems ensured the sustainability of the hearing screening program and facilitated systematic evaluation of its scope and efficacy. Ongoing research and technological development are aimed at increasing the screening program’s coverage and impact by facilitating greater involvement of the primary health care system and the family doctor network at all stages: detection, intervention, follow-up, and (re)habilitation.
ACKNOWLEDGMENTS
We would like to thank all those who have contributed to the success of our work, especially Dr Blanca Carrillo Suárez, audiologist and Chief of the Clinical Audiology and Neurophysiology Service at the William Soler Pediatric Teaching Hospital, Havana; Teresa M. Morales, disability specialist and MS in Special Education, also with the Clinical Audiology and Neurophysiology Service at the William Soler Pediatric Teaching Hospital; and technicians Eduardo Eimil, Teresa López, Margarita Aguiar, Miriam Lombida and Liser Cabrera.
References

- Davidson J, Hyde ML, Alberti PW. Epidemiologic patterns in childhood hearing loss: a review. Int J Pediatr Otorhinolaryngol. 1989;17:226-39.
- Mauk GW, Cags MA, Behrens TR. Historical, political and technological context associated with early identification of hearing loss. Ear Hear. 1993;14:2-10.
- Stein LK, Jabaley T, Spitz R, Stoakley D, McGee T. The hearing-impairment infants: patterns of identification and habilitation revisited. Ear Hear. 1990;11:201-5.
- Joint Committee on Infant Hearing: Year 2000 position statement: principles and guidelines for early hearing detection and intervention programs. Pediatrics. 2000;106:798-816.
- Colectivo de Autores. Por la Vida. Havana: Abril, 2003.
- Pérez MC, Rodríguez C, Ponce de León M, Viera C, Aguiar M, Eimil E. Pesquisaje auditivo en niños egresados de unidades de cuidados intensivos pediátricas. Estudios Avanzados de Neurociencias. CENIC. 1987; Suppl:560-71.
- Pérez MC, Perera M, Bobes M, Valdés M, Sánchez M. Ensayo de pesquisaje auditivo en Ciudad Habana. Rev Cub Invest Biomed. 1988;7:60-74.
- Pérez MC, Gaya J, Savio G, Ponce de León M, Perera M, Reigosa V. Diagnóstico e intervención temprana de los trastornos de la audición: Una experiencia cubana de 20 años. Rev Neurol. 2005;41:556-63.
- Kurtzer D, Hilpert P, Kreutzer J, Vaugham H. Differential maturation of cortical auditory evoked potential to speech sounds in normal full term and very low birth weight infants. Dev Med Child Neurol. 1984;26:466-75.
- Webster D. Auditory neural sizes after a unilateral conductive hearing loss. Exp Neurol. 1983;79:130-40.
- Davis JM, Elfebeim J, Schum R, Bentler RA. Effects of mild and moderate hearing impairments on language educational and psycho-social behaviour of children. J Speech Hear Disord. 1986;51:53-62.
- Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Language of early and later identified children with hearing loss. Pediatrics. 1998;102:1161-71.
- Reigosa V, Pérez MC, Hernández D, de la Osa M, Savio G, Rodríguez M, et al. Efectos de la detección temprana sobre el desarrollo psicosocial y lingüístico de niños con pérdidas auditivas permanentes. Revista CENIC/Ciencias Biológicas. 2002;33:99-105.
- Joint Committee on Infant Hearing. Year 2007 position statement: principles and guidelines for early hearing detection and intervention programs. Pediatrics. 2007;120:898-921.
- Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S. A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment. Health Technol Assess. 1997;1:1-176.
- Mencher GT, Davis AC, DeVoe S, Beresford D, Bamford J. Universal Neonatal Hearing Screening: past, present and future. Am J Audiol. 2001;10:1-10.
- Nelson HD, Bougatsos C, Nyren P. Universal newborn hearing screening: systematic review to update the 2001 US preventive services task force recommendation. Pediatrics. 2008;122:266-76.
- Jewett DL, Romano MN, Wilson JS. Human auditory evoked potentials: Possible brainstem components detected on the scalp. Science. 1970;167:1517-8.
- Kemp D. Stimulated acoustic emissions from within the human auditory system. J Acoust Soc Am. 1978;64:1386-9.
- Norton SJ, Gorga MP, Widen JE. Identification of neonatal hearing impairment: Evaluation of transient evoked otoacoustic emission, distortion product and auditory brainstem response test performance. Ear Hear. 2000;21:508-28.
- Stapells DR, Picton TW. Technical aspects of brainstem evoked potentials audiometry using tones. Ear Hear. 1981;2:20-9.
- Galambos R, Hicks G, Wilson M. The auditory brainstem response reliably predicts hearing loss in graduates of a tertiary intensive care nursery. Ear Hear. 1984;5:254-60.
- Hyde ML, Riko K, Malizia K. Audiometric accuracy of click ABR in infants at risk for hearing loss. J Am Acad Audiol. 1990;1:59-66.
- Durieux-Smith A, Picton TW, Edwards JT, Mac- Murray B, Goodman JT. Brainstem electric response audiometry in infants of a neonatal intensive care unit. Audiology. 1987; 26:284-97.
- Manzano M, Piñeiro A, Perera M. Asimilación y modificación de un test de pesquisaje para detectar tempranamente trastornos del lenguaje. Rev Cubana Psicol. 1997;14:120-8.
- Martín V, Báez O, Jiménez JC. Neuronica: sistema para la adquisición y análisis de señales bioeléctricas. In: Gutiérrez C, editor. Estudios Avanzados en Neurociencias. Havana: CENIC;1987. p.134-41.
- Valdés M, Bobes M, Pérez MC, Perera M, Carballo JA, Valdés P. Comparison of auditoryevoked potential detection methods using signal detection theory. Audiology. 1987;722:166-78.
- Bobes M, Valdés M, Pérez MC. Efecto de diferentes métodos de extracción de potenciales evocados sobre la relación señal ruido. Rev Cubana Ciencias Biolog. 1988;(1)2.
- Pérez MC, Perera M, Bobes M, Valdés M, Sánchez M. Caracterización de los potenciales evocados auditivos de tallo cerebral en lactantes cubanos. Rev Cubana Invest Biomed. 1986;5:419-29.
- Sanabria C, Pérez MC, Padrón O. Uso de la programación lógica en la interpretación de potenciales evocados auditivos de tallo cerebral. Rev Cubana Ciencias Biolog. 1988;19:189-91.
- Pérez MC, Valdés M, Bobes M, Galán L, Biscay R. Different functional properties of ON and OFF components in the auditory brainstem to tonebursts. Audiology. 1988;27:249-59.
- Lins OG, Picton TW, Boucher BL, Durieux-Smith A, Champagne SC, Moran LM, et al. Frequencyspecific audiometry using steady-state responses. Ear Hear. 1996;17:81-96.
- Cone-Wesson B, Parker J, Swiderski N, Rickards F. The auditory steady-state response: full-term and premature neonates. J Am Acad Audiol. 2002;13:260-9.
- Rance G, Roper R, Symons L, Moody LJ, Poulis C, Dourlay M, et al. Hearing threshold estimation in infants using auditory steady-state responses. J Am Acad Audiol. 2005;16:291-300.
- Pérez MC, Torres A, Savio G, Eimil E. Los potenciales evocados auditivos de estado estable a múltiples frecuencias y su valor en la evaluación objetiva de la audición. AUDITIO Revista Electrónica de Audiología. 2003 Nov;2(2):42-50.
- Valdés JL, Pérez MC, Martin V, Savio G, Sierra C, Rodriguez E, et al. Comparison of statistical indicators for the automatic detection of 80 Hz auditory steady state responses. Ear Hear. 1997;18:420-9.
- Lins OG, Picton TW. Auditory steady-state responses to multiple simultaneous stimuli. Electroencephalogr Clin Neurophysiol. 1995;96:420-32.
- Pérez MC, Savio G, Torres A, Martin V, Rodriguez E, Galan L. An optimized method to test frequency specific thresholds in hearing impaired children and normal subjects. Ear Hear. 2001;22:200-11.
- Biscay LR, Clark DI, Pérez MC. Maximum likelihood estimation of signal detection model parameters for the assessment of two stage diagnostic strategies. Int J Biomed Comput. 1992;31:117-26.
- Mauk GW, White KR, Mortensen LB. The effectiveness of screening programs based on high risk characteristics in early identification of hearing loss. Ear Hear. 1991;12:312-9.
- Parving A. Looking for the hearing-impaired child: Past, present and future. In: Seewald RC, Gravel J, editors. A sound foundation through early amplification 2001. Proceedings of the Second International Conference, sponsored by Phonak; 2001. p. 251-9.
- Lantigua Cruz A, Portuondo Sao M, Collazo Mesa T, Lardoyet Ferrer R. Epidemiology of prenatal genetic and enviromental factors of mental retardation in Cuba. MEDICC Review. 2008;10(1):29-36.
- Valett ER. Evaluación del Desarrollo de las Aptitudes Básicas para el Aprendizaje. Madrid: TEA;1987.
- Luts H, Desloovere C, Kumar A, Vandermeersch E, Wouters J. Objective assessment of frequency-specific hearing thresholds in babies. Int J Pediatr Otorhinolaryngol. 2004;68:915-26.
- Rance G, Tomlin D. Maturation of auditory steady-state responses in normal babies. Ear Hear. 2006;27:20-9.
- Savio G, Pérez MC, Gaya J, Hernández O, Mijares E. Test accuracy and prognostic validity of multiple auditory steady state responses for targeted hearing screening. Int J Audiol. 2006;45:109-20.
- Santos E, Pérez MC. Sistema semi-automático para el pesquisaje auditivo en recién nacidos sobre el electroaudiómetro Audix V. In: Book Series IFBM. Part I. Berlin/Heidelberg: Springer;2008. p.122-6.
- Savio G, Cárdenas J, Pérez MC, González A, Valdés J. The low and high frequency auditory steady state responses mature at different rates. Audiol Neurootol. 2001;6:279-87.
- Savio G, Mijares E, Pérez MC, Vega M, Lage A, Hernández D. Eficiencia de la detección automática de Potenciales Evocados Auditivos de Estado Estable a Múltiples Frecuencias evaluada mediante la metodología ROC. Rev Logop Fon Audiol. 2007;27:12-23.
- Savio G, Pérez-Abalo MC. The Auditory Steady- State Response: generation, recording and clinical application. In: Rance G, editor. ASSRs and Hearing Screening. San Diego: Plural Publishing;2007. p.185-99.
THE AUTHORS
María Cecilia Pérez Abalo (Corresponding Author: marilyn@cneuro.edu.cu), specialist in clinical neurophysiology. Senior researcher and head of the Speech and Hearing Sciences Department, Cuban Neuroscience Center, Havana.
José Antonio Gaya Vázquez, specialist in clinical neurophysiology. Speech and Hearing Sciences Department, Cuban Neuroscience Center.
Guillermo Savio López, specialist in clinical neurophysiology. Speech and Hearing Sciences Department, Cuban Neuroscience Center.
Maritza Perera González, MS in special education, Clinical Audiology and Neurophysiology Service, William Soler Pediatric Teaching Hospital, Havana.
Maribel Ponce de León Mola, ENT specialist. Otorhinolaryngologist and audiologist, Clinical Audiology and Neurophysiology Service, William Soler Pediatric Teaching Hospital, Havana.
Manuel Sánchez Castillo, electronics engineer, biotechnologist. Neurotechnology Department, Cuban Neuroscience Center.
Submitted: February 29, 2008 Approved: September 17, 2008









