Since first emerging in the late 1970s, the field of human genetics has advanced with extraordinary speed. In just thirteen years (1990 to 2003), the human genome project deciphered the code of life. Today, by detecting genetic predisposition to certain diseases, we can anticipate their appearance even before the onset of symptoms, and progress is being made toward creating so-called “personalized drugs” designed to fit an individual’s genetic profile.
Yet, these developments are far beyond the reach of the vast majority of people. Few countries have transformed the giant steps in human genetics into national policies, programs and services accessible to the general population.
Furthermore, widespread application of new therapeutic approaches to diseases of genetic origin lags behind the rapid development of diagnostic methods and technologies. At the same time, the technologies themselves open up new possibilities that raise ethical questions about their appropriate use when weighed against the obligation to preserve human dignity-cloning as a case in point.
Snapshot: The National Medical Genetics Center, Havana
Inaugurated by President Fidel Castro on August 5, 2003, the National Medical Genetics Center belongs to the Higher Institute of Medical Sciences of Havana and the Western Havana Scientific Pole. As the national reference center for medical genetics, it coordinates the national medical genetics network, human resources training, research, and health services. Internationally, it participates in joint research projects with institutions in Denmark, the United Kingdom and China. Since 1986, it has been a World Health Organization Collaborating Center for the Development of Genetic Approaches to Health Promotion.
The Center includes five state-of-the-art laboratories for cytogenetics, molecular biology, biochemical genetics, oxidative stress and immunogenetics, which conduct over 40,000 diagnostic studies annually.
Staff Profile
Total staff: 182
Researchers and technicians: 107
Average age: 41
Women: 73%
PhD: 9
MS: 19
Faculty in genetics, biochemistry and immunology, Higher Institute of Medical Sciences of Havana: 26
This, then, is the global context within which Cuba has developed a national program for the diagnosis, management, and prevention of genetic diseases and congenital malformations. The program was initiated in the 1980s as an integral part of the country’s universal health services, which emphasize community-based primary care linked to secondary and tertiary care.
The National Medical Genetics Network
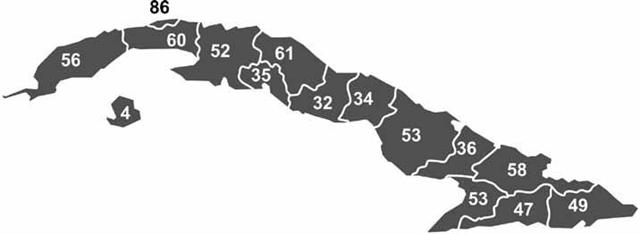
For the last seven years, based on the results of a national study in total population on prevalence of major disabilities and mental retardation in Cuba, training of personnel has been stepped up to meet the demand for medical genetics services at all levels of care. Over 1,600 technicians and university-level professionals are involved in the network; of these, 105 are clinical geneticists, and 736 have earned master’s degrees in genetic counseling. The majority (729) of these genetic counselors work at the primary care level. Municipal genetics centers were also established in Cuba’s 169 municipalities, as well as provincial centers in all 14 provinces (Figure 1). The national program is coordinated by the National Medical Genetics Center in Havana- the national reference center also responsible for undergraduate and postgraduate training, research, and introduction of new technologies in the field.
Figure 1: Distribution of Specialists with Master’s Degrees in Genetic Counseling by Province, Cuba, 2007

Human resources, National Medical Genetics Network
1,612 staff nationwide
736 with master’s degrees in genetic counseling
98 master’s degree candidates
Municipal distribution of professional genetic counselors (master’s degree)
27 municipalities with 2 genetic counselors
67 municipalities with 3 genetic counselors
28 municipalities with 4 genetic counselors
38 municipalities with 5-9 genetic counselors
9 municipalities with 10 or more genetic counselors
Source: National Medical Genetics Center, Havana.
The National Medical Genetics Network operates at all levels of care, beginning in the community polyclinic, where patients are referred by their family doctor. Each municipality has at least two professional genetic counselors who make the rounds of all polyclinics. This approach allows for genetic risk detection, community-level follow-up of screening and diagnostic programs, genetic counseling, and research on the causes and prevalence of genetic diseases and/or the role of genetic risk factors in common diseases.
The municipal genetics centers function as reference centers at the primary care level. Here, clinical diagnoses are confirmed by geneticists; prenatal diagnostic sonograms are performed to confirm results of prior screenings; and collection of diagnostic samples for screening programs is coordinated, carried out, and monitored. These programs include neonatal screening for genetic diseases and congenital malformations, and prenatal screening for maternal serum alpha-fetoprotein (MSAFP), sickle cell anemia risk, and fetal chromosome abnormalities. The municipal centers keep registries of people with disabilities for continued follow-up, as well as registries of genetic diseases and congenital malformations in their coverage areas.
Secondary level care is provided at the provincial centers, which serve as reference centers for clinical diagnosis, fetal sonogram and echocardiogram confirmation of congenital malformations, as well as pre- and postnatal diagnosis of chromosome abnormalities, laboratory tests for hemoglobin electrophoresis studies, and supervision of neonatal metabolic disease screenings.
At the tertiary care level, the national reference center is the National Medical Genetics Center where the most specialized laboratory research is conducted, and consulting is provided to other national medical research institutes. State-of-the-art equipment is concentrated at this site for use in research benefiting the entire population. All medical genetics services in Cuba are voluntary and provided free of charge.
Prevention, Diagnosis and Management
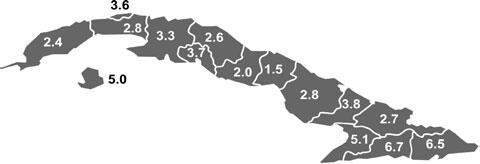
Prenatal screening. Screening programs offered to all pregnant women include: detection of sickle cell anemia carriers (Figure 2, Table 1); MSAFP testing to detect neural tube defects; genetic ultrasound tests at 20 and 22 weeks of gestation; and detection of Down Syndrome and other fetal chromosome abnormalities in pregnant women aged ≥37.
Figure 2: Percentage of Sickle Cell Trait Carriers among Pregnant Women in Cuba by Province, 2007

Source: National Medical Genetics Center, Havana.
When a problem is detected, a full explanation is given to the woman or couple, including the options of continuing or terminating the pregnancy. Prenatal diagnosis of such congenital malformations gives the woman or couple the opportunity to make a timely, informed decision about how they wish to proceed with a pregnancy involving a fetus with a detected anomaly and also provides the health care system with the necessary information to receive a sick newborn when a woman or couple chooses to continue pregnancy.
Table 1: Sickle Cell Trait Carriers among Pregnant Women in Cuba, 2005 to 2007
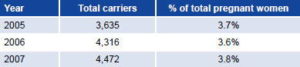
Source: Annual statistical reports, National Medical Genetics Center, Havana.
Neonatal screening. The program to prevent mental retardation and severe congenital disorders through early detection of treatable diseases was initiated in the early 1980s with phenylketonuria (PKU) screening. In 2005, the program was broadened to include screening for biotinidase deficiency, galactosemia, and congenital adrenal hyperplasia (Figure 3).
Clinical genetics. Clinical diagnosis of genetic diseases is made by clinical geneticists in collaboration with professional genetic counselors. In the last two years, the numbers have nearly tripled for both patients in follow-up care and those in diagnosis or counseling. As medical genetics services have become more accessible at the primary care level, demand for these services has grown.
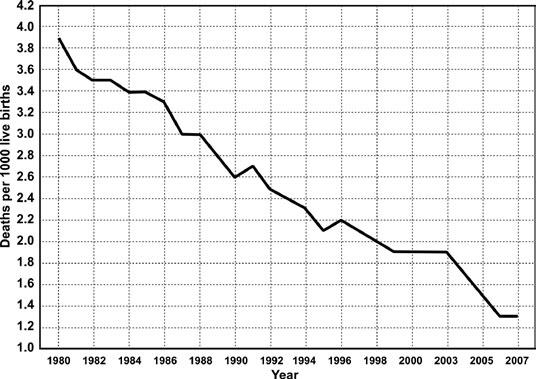
Infant mortality from congenital malformations. Congenital anomalies were the primary cause of death of 143 children aged <1 year in Cuba in 2007, a rate of 1.3 deaths from congenital anomalies per 1,000 live births (Figure 4). Congenital malformations account for about 25% of deaths among children aged <1 year.
Innate errors of metabolism and molecular diagnosis. Cases that test positive in neonatal screening are confirmed and followed up in National Medical Genetics Center laboratories. Diagnostic tests for 53 genetic diseases resulting from innate errors of metabolism are also available. The Center’s molecular biology laboratory carries out diagnostic DNA analysis for diseases such as hemophilia A and B, sickle cell anemia, cystic fibrosis, Fragile X syndrome, PKU, Huntington’s chorea, prenatal diagnosis of X chromosomelinked disorders, and others.
Care for people with disabilities. Care and follow-up of health problems and living conditions of people with disabilities is carried out in the community in collaboration with local social workers. A registry of people with disabilities is maintained at the national level and updated with information from the municipal genetics centers. The registry currently includes some 360,000 people.
Figure 3: Neonatal Screening Program Coverage, Cuba, 1990 to 2007

Source: Annual statistical reports, National Medical Genetics Center, Havana.
Figure 4: Infant Mortality Due to Congenital Malformations, Cuba, 1980 to 2007

Source: Annual statistical reports, National Medical Genetics Center, Havana.
Human Resource Capacity-Building and Research
Medical Genetics is taught as a 54-hour fourth-semester course in all Cuban medical schools. In post-graduate study, 32 residents are now training at the National Medical Genetics Center in clinical genetics, and another 20 in immunology. The Center also offers master’s degrees in genetic counseling and medical genetics.
Throughout the country, over 50 research projects are underway on the causes, prevalence, follow-up and management of genetic diseases and congenital malformations. The network is also involved in a multidisciplinary program of 23 studies on the causes of disabilities in Cuba, which includes experts from the Ministries of Public Health and Education as well as the Western Havana Scientific Pole. A national registry of families with multiple members affected by common diseases-such as asthma, high blood pressure, ischemic heart disease, diabetes mellitus, dementia, depression, schizophrenia, bipolar disorder, cancer, alcohol addiction, and mental retardation-has been kept since 2004 as part of a study on the role of genetic factors in the origin of these conditions. Over 43,000 families are thus far included in this registry.
Based on a national study involving other Western Havana Scientific Pole research institutes, the Ministry of Public Health and the Ministry of Education, a national registry of twins has also been created, identifying 55,000 pairs during the initial stage, which concluded in early 2006. Twins born since that year are added to the registry annually, upon their parents’ consent.
Conclusion
The Cuban Medical Genetics Program has made its greatest strides in the last five years. This includes accelerated training of professional genetic counselors through the master’s degree program; provision of infrastructure to set up all 184 centers in the network and equip them with information and communication technology; and construction of high-tech diagnostic and research laboratories at provincial centers and the National Medical Genetics Center.
The dedication and commitment of national network staff are also factors in the program’s development. The recognition we receive for our work and the gratitude of thousands of families who have benefited from the program’s systematic and prioritized care, strengthen our resolve to ease the pain experienced by families affected by genetic diseases and the severe disabilities they can cause.
We continue to work toward overcoming many challenges, including the need to expand our capacity for diagnosing genetic diseases. We also need to better inform and educate the public about our services and the effectiveness of medical genetics as part of health promotion and disease prevention strategies benefiting the entire population. Integration of the network with other medical fields and scientific institutions should also be improved. In the meantime, we are working toward digitizing the genetic disease and congenital malformations registries, and we continue to advance research on the role of genetic factors in the origin of diseases in Cuba, using an approach that gives weight to both biological and social factors.