Globally, SARS CoV-2 omicron variant has led to a notable increase of COVID-19 diagnoses, although with less severe clinical manifestations and decreased hospitalizations. The omicron wave swelled faster than previous waves, completely displacing the delta variant within weeks, and creating worldwide concern about final, successful pandemic control. Some authors contend that symptoms associated to omicron differ from ‘traditional’ symptoms and more closely resemble those of the common cold.
One major COVID-19 symptom frequent with other variants—loss of taste and smell—is rarely present with omicron. This may be of interest, since it has also been suggested that direct SARS-CoV-2 invasion into the brainstem through the olfactory nerves by transsynaptic pathways could provide one explanation for the acute respiratory distress syndrome refractory to treatment. Brainstem infection by SARS-CoV-2 can severely damage the respiratory center, triggering functional deviations that affect involuntary respiration, leading to acute respiratory distress syndrome refractory to treatment, the main cause of death in COVID-19 patients. A shift in the omicron SARS-CoV-2 entry pathway from cell-surface fusion, triggered by TMPRSS2, to cathepsin-dependent fusion within the endosome, may affect transmission, cellular tropism and pathogenesis. Therefore, we can hypothesize that this entrance modification may impact transmission from the olfactory nerve to the brainstem through transsynaptic pathways. A decrement of the virus’s direct invasion into the brainstem could diminish respiratory center dysfunction, reducing acute respiratory distress syndrome and the need for mechanical ventilation.
ABSTRACT Globally, SARS CoV-2 omicron variant has led to a notable increase of COVID-19 diagnoses, although with less severe clinical manifestations and decreased hospitalizations. The omicron wave swelled faster than previous waves, completely displacing the delta variant within weeks, and creating worldwide concern about final, successful pandemic control. Some authors contend that symptoms associated to omicron differ from ‘traditional’ symptoms and more closely resemble those of the common cold.
One major COVID-19 symptom frequent with other variants—loss of taste and smell—is rarely present with omicron. This may be of interest, since it has also been suggested that direct SARS-CoV-2 invasion into the brainstem through the olfactory nerves by transsynaptic pathways could provide one explanation for the acute respiratory distress syndrome refractory to treatment. Brainstem infection by SARS-CoV-2 can severely damage the respiratory center, triggering functional deviations that affect involuntary respiration, leading to acute respiratory distress syndrome refractory to treatment, the main cause of death in COVID-19 patients. A shift in the omicron SARS-CoV-2 entry pathway from cell-surface fusion, triggered by TMPRSS2, to cathepsin-dependent fusion within the endosome, may affect transmission, cellular tropism and pathogenesis. Therefore, we can hypothesize that this entrance modification may impact transmission from the olfactory nerve to the brainstem through transsynaptic pathways. A decrement of the virus’s direct invasion into the brainstem could diminish respiratory center dysfunction, reducing acute respiratory distress syndrome and the need for mechanical ventilation.
INTRODUCTION Globally, the SARS CoV-2 omicron variant has led to a significant increase of COVID-19 diagnoses with less severe clinical manifestations and decreased hospitalizations. The omicron wave has swelled faster than previous waves, completely displacing delta variant within weeks, and creating new worldwide concern about the ability to achieve final pandemic control.[1]
Omicron is the fifth variant to be named as a variant of concern by WHO and the third (after alpha and delta) to achieve global dominance.[2] Omicron was first documented in the city of Tshwane, Gauteng Province, South Africa, on November 9, 2021, in travelers from Hong Kong who were quarantined.[1] At the time of this writing, it had split into three divergent sublineages (BA.1, BA.2, and BA.3), of which BA.1 spread rapidly around the world.[1,2] Several initial reports suggested a less severe disease, including from researchers in South Africa, where the variant spread quickly.[1] In young people, omicron is 40%‒70% less severe than delta variant. Chen studied omicron variant infectivity, vaccine breakthrough, and antibody resistance. The author concluded that omicron variant infects and replicates 70 times faster in the human bronchi than delta variant and the original SARS-CoV-2 virus, which may explain why omicron is more transmissible than previous variants.[3] A recently published study from Hong Kong found that omicron replicates faster in bronchi than all other SARS-COV-2 variants, although less efficiently in the lung parenchyma. This could explain its increased transmissibility, but reduced severity.[4]
IMPORTANCE The SARS-CoV-2 omicron variant’s cell entry pathway differs from that of earlier variants and could explain the lower prevalence of acute respiratory distress, due to diminished invasion of the brainstem through the olfactory nerve. This change could have implications in patient management, as intractable respiratory distress syndrome is less likely to occur.
Some authors have emphasized that symptoms associated with omicron differ from ‘traditional’ COVID-19 symptoms, more closely resembling those of the common cold.[5] One major COVID-19 symptom is rare in omicron patients: loss of taste and smell.[6,7] Some research suggests that 48% of people carrying the original mutation of the novel coronavirus lost smell, and 41% had a loss of taste; these numbers decreased to 23% for loss of taste and 12% for loss of smell among omicron-infected patients.[8] Consequently, many people may not realize they have contracted COVID-19, since fewer experience cough, fever, or loss of taste or smell. A virus in the upper respiratory tract is associated with increased transmissibility, but with a less severe disease, exhibiting similarities with flu strains.[9]
The most deadly syndrome in COVID-19 patients is acute respiratory distress syndrome (ARDS), leading to severe respiratory failure and the need for mechanical ventilation in intensive care units (ICUs). Initial reports from Wuhan hospitals in China revealed that 11.1% received high–flow oxygen therapy, 41.7% received noninvasive ventilation, and 47.2% received invasive ventilation. These data suggest that most COVID-19 ICU patients (about 89%) could not breathe on their own.[10,11]
One explanation for ARDS resistance to treatment could be SARS-CoV-2 direct invasion into the brainstem. Such an invasion can severely damage the respiratory center, triggering functional deviations that affect involuntary respiration, leading to ARDS refractory to treatment, the main cause of death in COVID-19 patients. Evidence accumulated to date has led to a much wider acceptance of the neuroinvasive potential of SARS-CoV-2 for inducing respiratory failure in some patients.[11‒13,15,16]
Nevertheless, there have been conflicting hypotheses, based on the fact that brain damage leading to respiratory failure is usually accompanied by other signs of brain dysfunction, not reported in any of the initial Chinese case series.[14]
It is suspected that cranial nerves (CNs), particularly the olfactory nerve, contribute to the neuroinvasiveness of SARS-CoV-2.[17] The virus has been found in the olfactory mucous membrane, signaling involvement of the olfactory neuroepithelium. It can reach the olfactory bulb through anterograde axonal transport and can subsequently gain access to other neuroanatomical areas, such as the respiratory and cardiovascular centers of the medulla oblongata, via endocytosis and exocytosis for transsynaptic transfers. Numerous neurotropic agents, including parasites, bacteria and viruses, can reach the CNs via the olfactory nerve.[8,11] Other possibilities for neuroinvasion of SARS-CoV-2 are through hematogenous spread via either the blood–brain barrier (BBB) or the blood–cerebrospinal fluid barrier (B-CSFB).[18]
Coronaviruses cell entry depends on the viral spike (S) protein binding to cellular receptors and its priming by host cell proteases. SARS-CoV-2 uses the angiotensin-converting enzyme 2 (ACE2) receptor for entry and the plasma membrane serine protease 2 (TMPRSS2) for protein S priming.[19,20] The virus enters the nasal and mouth tissues through the ACE2 receptor and the proteolytic activation of the spike protein by TMPRSS2 in olfactory epithelia;[21] ACE2 is also expressed in brain locations (choroid plexus and olfactory bulb). Cell types expressing ACE2 include excitatory and inhibitory neurons, and some non-neuronal cells (astrocytes, oligodendrocytes and endothelia). Viral colonization of nose and mouth may cause temporary damage to smell and taste nerves; this damage tends to disappear within one to two weeks after disease onset.[22]
Recently, an alternate mechanism for central nervous system (CNS) entry of SARS-CoV-2 has been proposed, where neurons of the nervus terminalis—also known as cranial nerve ‘0’ at the olfactory epithelium in the nasal cavity—would be the carrier, rather than the olfactory nerve. Nervus terminalis neurons project directly to the hypothalamus in the brain, bypassing the olfactory bulb. Once the hypothalamus is reached, SARS-CoV-2 can cross the blood–brain barrier and reach neural circuits connected to the hypothalamus, including brainstem nuclei involved in respiration. As other cell types in the brain, the nervus terminalis expresses ACE2 but not TMPRSS2. This would favor the omicron variant’s preferential pathway for entering the cells, making this nerve a prime target for brain entry.[23]
SARS-CoV-2 spreads to the brainstem in the area of the medullar respiratory control centers and may produce discoordination of the inspiration–expiration sequence, explaining the appearance of other abnormal respiratory patterns: hyperpnea, tachypnea, hyperventilation, hypoventilation and not necessarily dyspnea.[11‒13] The omicron variant’s spike protein exhibits a series of mutations that affect affinity for the ACE2 receptor. It has been suggested that omicron switched its entry route into human cells, from cell surface fusion to cathepsin-dependent fusion within the endosome.[24] This fundamental shift is likely to influence omicron spread and the types of cells it can hijack. These changes may also affect the pathogenesis and severity of disease, and require further evaluation in population-based studies.[20,24]
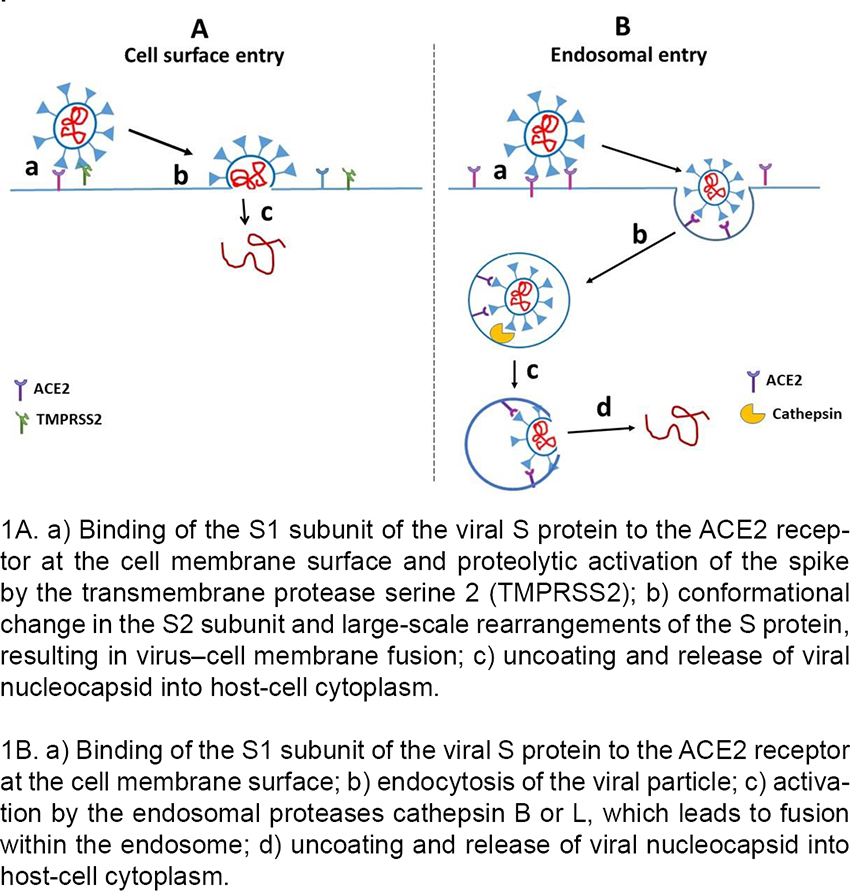
The entry of SARS-CoV-2 and related coronaviruses can proceed via two routes[24] (Figure 1):
Cell surface fusion following proteolysis by TMPRSS2
Fusion in the endosome after endocytosis and activation by the endosomal proteases cathepsin B or L (independent of TMPRSS2).
Figure 1: The entry of SARS-CoV-2 and related coronaviruses can proceed via two routes
The ability of SARS-CoV-2 to achieve cell-surface fusion is dependent on its S1/S2 polybasic cleavage site; this is absent from most closely related sarbecoviruses, which are confined to endosomal fusion.[24] Omicron, like pangolin CoV, has optimal properties for endosomal entry. Therefore, while delta entrance is improved for fusion at the cell surface (Figure 1A), omicron preferentially enters through endosomal fusion (Figure 1B). The previously mentioned modification in omicron’s entry mechanism could impact transmission, cellular tropism and pathogenesis, and offers an explanation for reduced cell fusion or syncytia formation by omicron-infected cells. Syncytia have been reported on autopsy in COVID-19 cases, and the efficient cleavage at the furin site underlying syncytia formation has been associated with enhanced disease severity in animal models.[25] This may explain the decreased disease severity, since these properties can substantially change the virus’s cellular tropism and disease pathogenesis.[24]
Concerning the neuroinvasive potential of SARS-CoV-2, modification of omicron’s biological properties might result in less effective transmission along the olfactory nerve and its projection to the brainstem, reflected clinically in less frequent impairment of smell and taste. We hypothesize that it could preferentially direct transmission from the olfactory nerve to the brainstem through transsynaptic pathways. Hence, decreased viral invasion directly into the brainstem would diminish respiratory center dysfunction, while reducing ARDS complication and the need for mechanical ventilation. Evidence strongly supports the association of neurological involvement with the lethality of SARS-CoV-2 infection, and omicron’s severity and lethality are much lower than those of other previous variants.[26]
Other causes may explain why the omicron variant is related to a milder symptomatology and a reduced viral access to the CNS: 1) omicron infection in the lung is significantly less frequent than that of the original SARS-CoV-2, thus leading to lower severity and, subsequently, lower prevalence of respiratory distress; 2) lower pathogenic effect could generate a lower viral load and less local or systemic inflammation; 3) acquired immunity (by previous infection or vaccination) during more than two years of pandemic.
The possible interpretations proposed here should be reviewed cautiously. Understanding SARS-CoV-2’s entry mechanisms into the CNS is still challenging, despite intense research on this topic. Two years of investigation are insufficient to arrive at definitive conclusions in any area of biological research. In the case of the omicron variant, this is especially so. More studies are required to establish the exact mechanisms of how the SARS-CoV-2 variants reach the brain stem, and to what extent this phenomenon can contribute to inducing ARDS resistant to treatment. We must keep in mind that the route and molecular mechanisms of neuroinvasion are not the only factors involved in ARDS development in COVID-19 patients. Other processes must be considered, such as previous specific immunity and disregulated innate immune responses leading to neuroinflammation.
CONCLUSIONS A shift in the omicron SARS-CoV-2 entry pathway from cell-surface fusion, triggered by TMPRSS2, to cathepsin-dependent fusion within the endosome, may affect transmission, cellular tropism and pathogenesis. Therefore, we can hypothesize that this entrance modification may impact transmission from the olfactory nerve to the brainstem through transsynaptic pathways. Decreased direct viral invasion of the brainstem could diminish respiratory center dysfunction, reducing acute respiratory distress syndrome and the need for mechanical ventilation.
Abdullah F, Myers J, Basu D, Tintinger G, Ueckermann V, Mathebula M, et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in Tshwane, South Africa. Int J Infect Dis. 2021 Mar;116:38–42. https://doi.org/10.1016/j.ijid.2021.12.357
Chen J, Wang R, Gilby NB, Wei GW. Omicron variant (B.1.1.529): infectivity, vaccine breakthrough, and antibody resistance. J Chem Inf Mod. 2022 Jan 24;62(2):412–22. https://doi.org/10.1021/acs.jcim.1c01451
Hui KPY, Ho JCW, Cheung M-C, Ng K-C, Ching RHH, Lai K-L, et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature. 2022 Mar;603(7902):715–20. https://doi.org/10.1038/s41586-022-04479-6
Weir EM, Reed DR, Pepino MY, Veldhuizen MG, Hayes JE. Massively collaborative crowdsourced research on COVID19 and the chemical senses: insights and outcomes. Food Qual Prefer. 2022 Apr;97:104483. https://doi.org/10.1016/j.foodqual.2021.104483
Rodríguez-Sevilla JJ, Güerri-Fernández R, Bertran Recasens B. Is there less alteration of smell sensation in patients with Omicron SARS-CoV-2 variant infection? Front Med (Lausanne). 2022 Apr 12;12;9:852998. https://doi.org/10.3389/fmed.2022.852998
Boscolo-Rizzo P, Tirelli G, Meloni P, Hopkins C, Madeddu G, De Vito A, et al. COVID-19-related smell and taste impairment with widespread diffusion of SARS-CoV-2 Omicron variant. Int Forum Allergy Rhinol. 2022 Mar 14;10.1002/alr.22995. Online ahead of print. https://doi.org/10.1101/2022.02.17.22271116
Fall A, Eldesouki RE, Sachithanandham J, Morris CP, Norton JM, Gaston DC, et al. The displacement of the SARS-CoV-2 variant Delta with Omicron: An investigation of hospital admissions and upper respiratory viral loads. EBioMedicine. 2022 May;79:104008. https://doi.org/10.1016/j.ebiom.2022.104008
Machado-Curbelo C. Silent or ‘happy’ hypoxemia: an urgent dilemma for COVID-19 patient care. MEDICC Rev. 2020 Oct;22(4):85–6. https://doi.org/10.37757/MR2020.V22.N4.9
Machado-Curbelo C. Severe COVID-19 cases: is respiratory distress partially explained by central nervous system involvement? MEDICC Rev. 2020 Apr;22(2):38–9. https://doi.org/10.37757/MR2020.V22.N2.10
Machado C, DeFina PA, Chinchilla M, Machado Y, Machado Y. Brainstem dysfunction in SARS-COV-2 infection can be a potential cause of respiratory distress. Neurol India. 2020 Sep‒Oct;68(5):989‒93. https://doi.org/10.4103/0028-3886.299165. PMID: 33109839.
Bulfamante G, Bocci T, Falleni M, Campiglio L, Coppola S, Tosi D. Brainstem neuropathology in two cases of COVID-19: SARS-CoV-2 trafficking between brain and lung. J Neurol. 2021 Dec;268(12):4486–91. https://doi.org/10.1007/s00415-021-10604-8
Turtle L. Respiratory failure alone does not suggest central nervous system invasion by SARS-CoV-2. J Med Virol. 2020 Jul;92(7):705–6. https://doi.org/10.1002/jmv.25828
Bocci T, Bulfamante G, Campiglio L, Coppola S, Falleni M, Chiumello D, et al. Brainstem clinical and neurophysiological involvement in COVID-19. J Neurol. 2021 Oct;268(10):3598–600. https://doi.org/10.1007/s00415-021-10474-0
Vecchio E, Gallicchio L, Caporusso N, Recchia V, Didonna L, Pezzuto G, et al. Neurophysiological aspects in SARS-CoV-2–induced acute respiratory distress syndrome. Front Neurol. 2022 May 16;13:868538. https://doi.org/10.3389/fneur.2022.868538
Sun T, Guan J, You C. The neuroinvasive potential of severe acute respiratory syndrome coronavirus 2. Brain Behav Immun. 2020 Aug;88:59. https://doi.org/10.1016/j.bbi.2020.05.079
Bauer L, Laksono BM, de Vrij FMS, Kushner SA, Harschnitz O, van Riel D. The neuroinvasiveness, neurotropism, and neurovirulence of SARS-CoV-2. Trends Neurosci. 2022 May;45(5):358–68. https://doi.org/10.1016/j.tins.2022.02.006
Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020 Apr 16;181(2):271–80. https://doi.org/10.1016/j.cell.2020.02.052
Sun Y, Lin W, Dong W, Xu J. Origin and evolutionary analysis of the SARS-CoV-2 Omicron variant. J Biosaf Biosecur. 2022 Jun;4(1):33–7. https://doi.org/10.1016/j.jobb.2021.12.001
Sommerstein R, Kochen MM, Messerli FH, Gräni C. Coronavirus Disease 2019 (COVID-19): do angiotensin-converting enzyme inhibitors/angiotensin receptor blockers have a biphasic effect? J Am Heart Assoc. 2020 Apr 7;9(7):e016509. https://doi.org/10.1161/JAHA.120.016509
Butowt R, von Bartheld CS. The route of SARS-CoV-2 to brain infection: have we been barking up the wrong tree? Mol Neurodegener. 2022 Mar 15;17(1):20. https://doi.org/10.1186/s13024-022-00529-9
Peacock TP, Brown JC, Zhou J, Zhou J, Thakur N, Sukhova K, et al. The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry. bioRxiv [Preprint]. 2022 Jan 3. https://doi.org/10.1101/2021.12.31.474653
Braga L, Ali H, Secco I, Chiavacci E, Neves G, Goldhill D, et al. Drugs that inhibit TMEM16 proteins block SARS-CoV-2 spike-induced syncytia. Nature. 2021 Jun;594(7861):88–93. https://doi.org/10.1038/s41586-021-03491-6
Liu JM, Tan BH, Wu S, Gui Y, Suo JL, Li YC. Evidence of central nervous system infection and neuroinvasive routes, as well as neurological involvement, in the lethality of SARS-CoV-2 infection. J Med Virol. 2021 Mar;93(3):1304–13. https://doi.org/10.1002/jmv.26570
THE AUTHORS
Calixto Machado-Curbelo (Corresponding author: braind@infomed.sld.cu), neurologist and clinical neurophysiologist with a doctorate in medical sciences and an advanced doctorate in sciences. Senior professor and researcher. Department of Clinical Neurophysiology, Institute of Neurology and Neurosurgery (INN), Havana, Cuba. https://orcid.org/0000-0002-0539-5844
Joel Gutierrez-Gil, physician specializing in clinical neurophysiology with a doctorate in medical sciences. Full professor and senior researcher. Head, Department of Clinical Neurophysiology, INN, Havana, Cuba. https://orcid.org/0000-0003-1805-7200
Alina González-Quevedo, physician specializing in clinical neurochemistry with a doctorate in medical sciences. Full professor and senior researcher, Department of Neurobiology, INN, Havana, Cuba. https://orcid.org/0000-0003-1952-4704
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.