INTRODUCTION Bile acids are signaling molecules with immune, metabolic and intestinal microbiota control actions. In high serum concentrations they increase inflammatory response from the liver-gut axis, until causing multiorgan failure and death; therefore, they may be associated with COVID-19’s clinical progression, as a consequence of tissue and metabolic damage caused by SARS-CoV-2. While this topic is of considerable clinical interest, to our knowledge, it has not been studied in Cuba.
OBJECTIVES Study and preliminarily characterize patients admitted with a diagnosis of COVID-19 and high levels of serum bile acids.
METHODS A preliminary exploratory study was carried out with descriptive statistical techniques in 28 COVID-19 patients (17 women, 11 men; aged 19–92 years) who exhibited high levels of serum bile acids (≥10.1 µmol/L) on admission to the Dr. Luis Díaz Soto Central Military Hospital in Havana, Cuba, from September through November 2021.
RESULTS On admission patients presented hypocholesterolemia (13/28; 46.4%), hyperglycemia (12/28; 43.0%) and hyper gamma-glutamyl transpeptidase (23/28; 84.2%). Median blood glucose (5.8 mmol/L) and cholesterol (4.1 mmol/L) were within normal ranges (3.2‒6.2 mmol/L and 3.9‒5.2 mmol/L, respectively). Severe or critical stage was the most frequent (13/28) and median serum bile acids (31.6 µmol/L) and gamma-glutamyl transferase (108.6 U/L) averaged well above their respective normal ranges (serum bile acids: 0‒10 µmol/L; GGT: 9‒36 U/L). Arterial hypertension was the most frequent comorbidity (19/28; 67.9%).
CONCLUSIONS Severe or critical stage predominated, with serum bile acids and gamma-glutamyl transferase blood levels above normal ranges. The study suggests that serum bile acid is toxic at levels ≥10.1 µmol/L, and at such levels is involved in the inflammatory process and in progression to severe and critical clinical stages of the disease. In turn, this indicates the importance of monitoring bile acid homeostasis in hospitalized COVID-19 patients and including control of its toxicity in treatment protocols.
KEYWORDS COVID-19, SARS-CoV-2, bile acids and salts, gamma-glutamyl transferase, pregnant women, postpartum, Cuba
ABSTRACT INTRODUCTION Bile acids are signaling molecules with immune, metabolic and intestinal microbiota control actions. In high serum concentrations they increase inflammatory response from the liver-gut axis, until causing multiorgan failure and death; therefore, they may be associated with COVID-19’s clinical progression, as a consequence of tissue and metabolic damage caused by SARS-CoV-2. While this topic is of considerable clinical interest, to our knowledge, it has not been studied in Cuba.
OBJECTIVEStudy and preliminarily characterize patients admitted with a diagnosis of COVID-19 and high levels of serum bile acids.
METHODSA preliminary exploratory study was carried out with descriptive statistical techniques in 28 COVID-19 patients (17 women, 11 men; aged 19–92 years) who exhibited high levels of serum bile acids (≥10.1 µmol/L) on admission to the Dr. Luis Díaz Soto Central Military Hospital in Havana, Cuba, from September through November 2021.
RESULTS On admission patients presented hypocholesterolemia (13/28; 46.4%), hyperglycemia (12/28; 43.0%) and hyper gamma-glutamyl transpeptidase (23/28; 84.2%). Median blood glucose (5.8 mmol/L) and cholesterol (4.1 mmol/L) were within normal ranges (3.2‒6.2 mmol/L and 3.9‒5.2 mmol/L, respectively). Severe or critical stage was the most frequent (13/28) and median serum bile acids (31.6 µmol/L) and gamma-glutamyl transferase (108.6 U/L) averaged well above their respective normal ranges (serum bile acids: 0‒10 µmol/L; GGT: 9‒36 U/L). Arterial hypertension was the most frequent comorbidity (19/28; 67.9%).
CONCLUSIONSSevere or critical stage predominated, with serum bile acids and gamma-glutamyl transferase blood levels above normal ranges. The study suggests that serum bile acid is toxic at levels ≥10.1 µmol/L, and at such levels is involved in the inflammatory process and in progression to severe and critical clinical stages of the disease. In turn, this indicates the importance of monitoring bile acid homeostasis in hospitalized COVID-19 patients and including control of its toxicity in treatment protocols.
KEYWORDSCOVID-19, SARS-CoV-2, bile acids and salts, gamma-glutamyl transferase, pregnant women, postpartum, Cuba
INTRODUCTION Toxic action of bile acids has been reported since 1933 and their biological activities were described in the late 1990s. Bile acids are signaling molecules and, when interacting with nuclear receptors and cellular transporters, express a sequence of actions linked to physical-chemical properties, conjugation with glycine or taurine, primary or secondary synthesis, and hepatic and intestinal transport, among others.[1,2] These properties explain their pleiotropic activities, such as intestinal absorption of fats and fat-soluble vitamins, and control of energy, lipid, glycemic, cholesterol and immune-system metabolism. This would also explain their influence on the specific activity of organs such as the heart, lungs, kidneys and nervous system. [3,4] These concepts offer a comprehensive view of their biological activities within the framework of novel approaches in human physiology.[5]
IMPORTANCE This is the first report in Cuba of COVID-19 cases with high levels of serum bile acids on hospital admission. Its findings suggest disease progression could be linked to the toxic effect of bile acids, such as worsening of the clinical stage and high levels of gamma-glutamyl transferase. The study establishes several premises for further research related to serum bile acids in management and follow-up of COVID-19 patients.
In vivo and in vitro studies show that high levels of bile acids maintained on plasma membranes and cellular DNA generate an inflammatory sequence that increases oxidative stress, protein denaturation and misfolding, decreased calcium and iron ion levels, and formation of secondary structures in DNA, as well as dysfunction of mitochondria and other organelles, responsible for genesis and persistence or amplification of the inflammatory and proinflammatory response.[5,6]
Reference levels considered normal vary according to the different assays and units of measurement used, and may be standardized internationally, regionally, and even by institutions and reagent manufacturers. Thus, the normal range used by the International System of Units (SI) is 10‒19 µmol/L,[7] Chinese researchers use 0‒12 µmol/L,[8] while the German company DiaSys Diagnostic Systems (GmbH) uses a normal range of 0‒10 µmol/L.[9]
Despite reports of digestive and extradigestive toxic effects of serum bile acids and use of new therapeutic interventions, such as ursodeoxycholic acid in various conditions and in pregnancy,[10] there has been virtually no published research on serum levels in COVID-19, the results of which could explain clinical and tissue changes in patients, conditioned by homeostatic decontrol of bile acids.
This is the first report in Cuba of cases with COVID-19 and high serum levels of bile acids (≥10.1 µmol/L) and it aims to describe characteristics of patients on admission, as a first step to considering eventual changes in clinical teaching, care and research regarding this potential association.
METHODS A case study was conducted for reasons of feasibility, its flexible design enabling a preliminary approach to the problem, hypothesis generation and formulation of bases for future studies.
The Dr. Luis Díaz Soto Central Military Hospital is a general hospital that also serves the adjacent civilian population and has a gynecology-obstetrics service. In the pandemic, this Havana facility also received all pregnant COVID-19 confirmed cases in the city.[11] During September–November 2021, 91 PCR-confirmed COVID-19 patients were admitted. On admission, all patients underwent serum bile acid assay, found to be high in 28 patients who comprised the case series studied; all were aged >18 years, and the group included six pregnant and two postpartum women.
Patients were interviewed; physical exams, imaging studies and blood tests were carried out.
Study variables Evaluated were: clinical stage (mild: patient with mild symptoms, such as upper respiratory symptoms, no pneumonia; moderate: patient with mild pneumonia without respiratory failure or inflammatory response; severe: patient presenting pneumonia with acute respiratory failure, and pneumonia with inflammation and hypercoagulability; critical: patient with intubation and assisted ventilation, shock and multiorgan failure),[11] clinical and imaging assessment, blood tests (blood glucose, cholesterol, gamma-glutamyl transferase or GGT, and serum bile acids) and comorbidities.
Bile acid testing at admission was done using a stand-alone clinical chemistry analyzer (Cobas c 311, Roche Diagnostics International Ltd, Switzerland) that fulfilled parameters for calibration and calculation stability with standards in µmol/L established by DiaSys Diagnostic Systems GmbH (Germany), which consider reference values of 0‒10 µmol/L as normal and ≥10.1 µmol/L as high.[9] For blood glucose, cholesterol and GGT, methods standardized in Cuba’s clinical laboratories and approved by the country’s Ministry of Public Health were used.[12]
Results were presented in frequency tables.
Ethics This study followed the principles of the Declaration of Helsinki.[13] Patients or legal guardians (in cases of critical and disabled patients) provided written informed consent and patient anonymity was maintained.
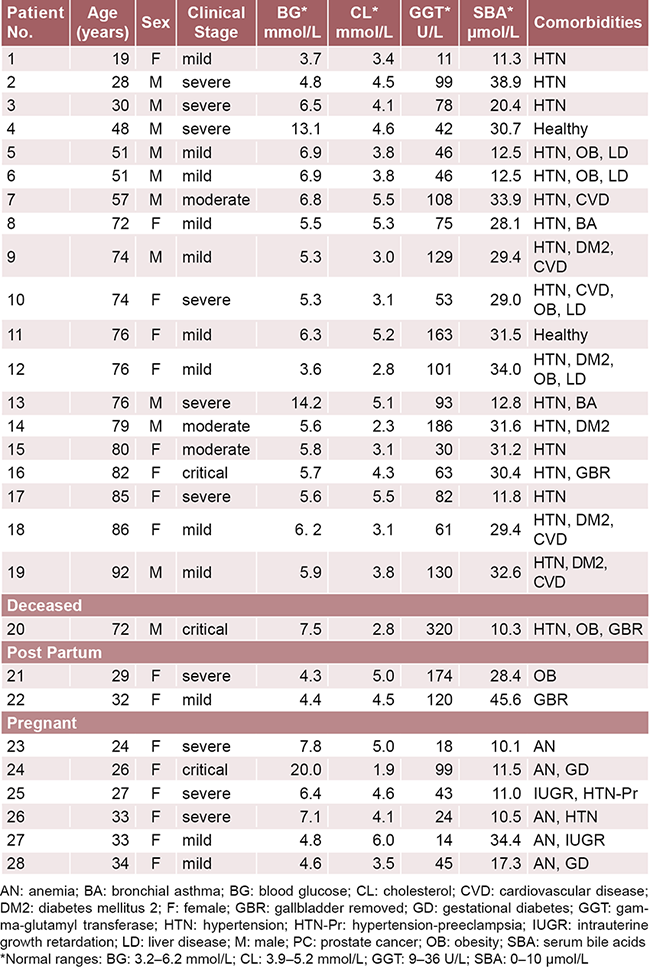
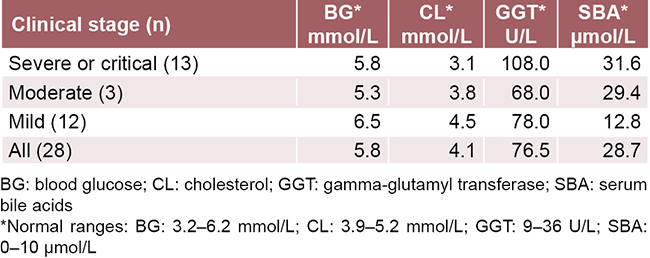
RESULTS Table 1 shows the results of the case series. Of the total admitted cases, 30.8% (28/91) had high serum bile acids at admission. Ages ranged from 19 to 92 years, and 60.7% of cases (17/28) were women. The series had a mean serum bile acid of 23.9 µmol/L, with a median of 28.7 µmol/L. Values were higher the more severe the clinical picture (Table 2). GGT figures were the furthest from the normal range, with a median of 76.5 U/L, higher in patients at the severe or critical stages (108.0 U/L). All cases had a clinical and imaging diagnosis of pneumonia or bronchopneumonia on admission. There was a remarkable abundance of comorbidities.
Table 1: Case series of patients with COVID-19 and high serum bile acid levels on admission to the Dr. Luis Díaz Soto Central Military Hospital, Havana, 2021
Table 2: Medians for blood chemistry variables, serum bile acids and gamma-glutamyl transferase, by clinical stage
Hypertension was the most frequent, present in 67.9% (19/28) of patients; 6 were diabetic and 6 were obese (21.4%; 6/28). Five (17.9%; 5/28) had 4 or more comorbidities and only 2 (7.1%; 2/28) previously had no comorbidities.
DISCUSSION High rates of mortality, morbidity and sequelae from COVID-19 are related to immune and metabolic disorders that are the pathophysiological basis of the disease.[14] These disorders involve the release of multiple proinflammatory mediators that trigger an inflammatory response in various organs and tissues. These tissues contain angiotensin-converting enzyme 2 (ACE2) receptors, used by SARS-CoV-2 for cell entry. Once inside the cell, the viral particles cause damage that results in immune intolerance and metabolic dysregulation in general, especially of cholesterol. It should be noted that 50% of derivatives of the end product of hepatic cholesterol catabolism are bile acids.[15]
When SARS-CoV-2 infects susceptible cells in various organs, especially those of the cholangiolar epithelium (cholangiocytes) of the bile canaliculi and bile ducts, it triggers an inflammatory response that results in functional damage and lysis, which impacts bile acid secretion and transport.[16]
The epithelial cells of the terminal ileum have the second highest distribution of ACE2 receptors in the body. Upon infection, the absorption, intestinal microbiota and intracellular transport of bile acids are dysregulated.[17]
In severe and critical COVID-19 patients, clinical manifestations of intestinal failure have been observed, presenting as uncontrolled metabolic homeostasis and proinflammatory mediators released by immune system cells. There is also uncontrolled intestinal motility, mucus secretion and breakdown of the intestinal barrier. This inflammatory process can lead to alterations in intestinal permeability, bacterial translocation, local or systemic sepsis and in extreme cases multiorgan failure and death. Bile acids may influence or be one of the factors that trigger the process.[18]
However, there is a notable absence of reports in the medical literature of patients with COVID-19 whose clinical manifestations (cardiac, renal, pulmonary, hematological, neurological and intestinal) are associated with homeostatic imbalance of bile acids or evidence of the toxic damage they cause.[2,4]
Furthermore, bile acids are neither part of the optional or required blood chemistry in care of COVID-19 patients on admission nor throughout their disease, whether severe or critical. These tests are not included in the followup of patients in intensive care, or in any of the existing national[11] and international protocols,[19] despite all the accumulated evidence of their effect on other diseases that progress to severity and of their importance in the management of pregnancy with cholestasis or fatty liver.
This study has limitations inherent to exploratory designs based on case series, whose purpose is to describe potential clinically relevant findings while not aspiring to signal causal relationships or other types of associations. Nevertheless, these preliminary results suggest the need to design and execute analytical studies that will enable a deeper understanding of the probable role of bile acids in the clinical course of patients with COVID-19.
CONCLUSIONS The patients admitted with COVID-19 and high serum levels of bile acids levels in this case series were primarily women in the severe or critical stage, with GGT above normal for established ranges.
Coupled with the scarce evidence from recent literature, the study suggests at least two considerations: (1) that serum bile acid levels ≥10.1 µmol/L are toxic and are involved in the inflammatory process and in disease progression to unfavorable clinical stages, and (2) that it is important to monitor bile acid homeostasis in hospitalized COVID-19 patients, and to include control of its toxicity in treatment protocols.
ACKNOWLEDGMENTS The authors would like to thank DiaSys Diagnostic Systems GmbH (Germany), Dr Klaus E. Mönkemüller and Dr Enrique Abraham Marcel, suppliers of the diagnostic kits for measuring serum bile acids; Dr Jacinta Otero Iglesias, medical biostatistician, who contributed to the methodological design of the research; Ivet López Rodríguez, representative of the Embassy of the Republic of Cuba in Germany, who helped arrange transportation of the diagnostic kits to Cuba; and to the medical staff of the Dr Luis Díaz Soto Central Military Hospital, for caring for the patients and gathering their information.
Wieland H, Dane E. The constitution of the bile acids. II. The place of attachment of the side chain. Z Physiol Chem. 1933;219:240‒44.
Fiorucci S, Distrutti E, Carino A, Zampella A, Biagioli M. Bile acids and their receptors in metabolic disorders. Prog Lipid Res. 2021 Apr;82:101094. https://doi.org/10.1016/j.plipres.2021.101094
Wang Y, Yutuc E, Griffiths WJ. Cholesterol metabolism pathways – are the intermediates more important than the products? FEBS J. 2021 Jun;288(12):3727‒45. https://doi.org/10.1111/febs.15727
Yang J, Palmiotti A, Kuipers F. Emerging roles of bile acids in control of intestinal functions. Curr Opin Clin Nutr Metab Care. 2021 Mar 1;24(2):127‒33. https://doi.org/10.1097/MCO.0000000000000709
Perino A, Demagny H, Velázquez-Villegas L, Schoonjans K. Molecular physiology of bile acid signaling in health, disease, and aging. Physiol Rev. 2021 Apr 1;101(2):683‒731. https://dx.doi.org/10.1152/physrev Costanzi E, Graziosi L, et al. Bile acid signaling in inflammatory bowel diseases. Dig Dis Sci. 2021 Mar;66(3):674‒93. https://doi.org/10.1007/s10620-020-06715-3
Manzotti C, Casazza G, Stimac T, Nikolova D, Gluud C. Total serum bile acids or serum bile acid profile, or both, for the diagnosis of intrahepatic cholestasis of pregnancy. Cochrane Database Syst Rev. 2019 Jul;7(7):CD012546. https://doi.org/10.1002/14651858
Wang H, Yan D, Li Y, Gong Y, Mai Y, Li B, et al. Clinical and antibody characteristics reveal diverse signatures of severe and non-severe SARS-CoV-2 patients. Infect Dis Poverty. 2022 Feb 2;11(1):15. https://doi.org/10.1186/s40249-022-00940-w
Ácidos biliares. Para la determinación in vitro de ácidos biliares en suero o plasma EDTA fresco en sistema fotométricos [Internet]. Holzheim (DE): DiaSys Diagnostic Systems GmbH; 2007 Jan [cited 2021 Sep 21]. 2 p. Available at: https://www.red-gdl.com/wp-content/uploads/2014/06/Acidos-biliares.pdf. Spanish.
Roy A, Premkumar M, Mishra S, Mehtani R, Suri V, Aggarwal N, et al. Role of ursodeoxycholic acid on maternal serum bile acids and perinatal outcomes in intrahepatic cholestasis of pregnancy. Eur J Gastroenterol Hepatol. 2021 Apr 1;33(4):571‒6. https://doi.org/10.1097/MEG.0000000000001954
Mejías Sánchez Y, Morales Suárez I, Arteaga García A, Alfonso Sánchez I. Estructuración del protocolo cubano de actuación para la atención de casos COVID-19. Rev Cubana Salud Pública [Internet]. 2021 [cited 2021 Sep 21];47(3):e2922. Available at: http://www.revsaludpublica.sld.cu/
Sharma A, Ahmad Farouk I, Kumar Lal S. COVID-19: a review on the novel Coronavirus disease evolution, transmission, detection, control and prevention. Viruses. 2021 Jan 29;13(2):202. https://doi.org/10.3390/v13020202
Kočar E, Režen T, Rozman D. Cholesterol, lipoproteins, and COVID-19: basic concepts and clinical applications. Biochim Biophys Acta Mol Cell Biol Lipids. 2021 Feb;1866(2):158849. https://doi.org/10.1016/j.bbalip.2020.158849
Rojas M, Rodríguez Y, Zapata E, Hernández JC, Anaya JM. Cholangiopathy as part of post-COVID syndrome. J Transl Autoimmun. 2021;4:100116. https://doi.org/10.1016/j.jtauto.2021.100116
Sajdel-Sulkowska EM. A dual-route perspective of SARS-CoV-2 infection: lung- vs. gut-specific effects of ACE-2 deficiency. Front Pharmacol. 2021 Jun 11;12:684610. https://doi.org/10.3389/fphar.2021.684610
Ballanamada Appaiah NN, Boyle K, Rogers D, Stewart J, Baker M. Intestinal failure: epidemiology, catheter-related sepsis and challenges. Cureus. 2021 Jul 1;13(7):e16093. https://doi.org/10.7759/cureus.16093
World Health Organization [Internet]. Geneva: World Health Organization; c2022. Publications. Overview. Living guidance for clinical management of COVID-19; 2021 Nov 23 [cited 2022 Jul 10]; [2.4 MB]. Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2
THE AUTHORS
Felipe Neri Piñol-Jiménez Corresponding author: fpinol@infomed.sld.cu), gastroenterologist with a master’s degree in infectious diseases, a doctorate in medical sciences and an advanced doctorate in sciences. Full professor and senior researcher, National Center of Minimally Invasive Surgery (CNCMA), Havana, Cuba. http://orcid.org/0000-0003-0522-8875
Virginia Capó-de Paz, pathologist with a doctorate in medical sciences and an advanced doctorate in science. Full professor and senior researcher, Pedro Kourí Tropical Medicine Institute (IPK), Havana, Cuba. http://orcid.org/0000-0002-9711-9475
Julián Francisco Ruiz-Torres, gastroenterologist with a doctorate in medical sciences. Full professor and senior researcher, CNCMA, Havana, Cuba. http://orcid.org/0000-0002-0024-6487
Teresita Montero-González, athologist with a doctorate in medical sciences. Full professor and senior researcher, Dr. Luis Díaz Soto Central Military Hospital, Havana, Cuba. http://orcid.org/0000-0003-3372-6791
Sara Amneris Urgellés-Carreras,OB-GYN with a master’s degree in comprehensive women’s care and a doctorate in medical sciences. Full professor, Dr. Luis Díaz Soto Central Military Hospital, Havana, Cuba. http://orcid.org/0000-0002-5832-9250
Armando Amador-Armenteros, clinical biochemist, Dr. Luis Díaz Soto Central Military Hospital, Havana, Cuba. http://orcid.org/0000-0003-1995-1044
María Mercedes Llerena-Mesa, healthcare technologist with a master’s degree in clinical laboratory sciences, Dr. Luis Díaz Soto Central Military Hospital, Havana, Cuba. http://orcid.org/0000-0003-2933-9377
Ana Gloria Galarraga-Lazcano, physician specializing in clinical laboratory practices, with a master’s degree in clinical laboratory sciences, Dr. Luis Díaz Soto Central Military Hospital, Havana, Cuba. http://orcid.org/0000-0002-6492-0012
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.