Another conceivable explanation for such severe hypoxemia occurring in otherwise compliant lungs is hypoxic vasoconstriction and loss of perfusion regulation. Several authors contend that diffuse pulmonary microvascular thrombosis might be the cause of hypoxemia in early SARS-CoV-2–induced pneumonia. Histologic and immunohistochemical studies suggest that catastrophic, complement-mediated thrombotic microvascular injury happens in severe SARS-CoV-2 infection, with continuous activation of the lectin pathway cascade, leading to the recommendation that anticoagulants, specifically low molecular-weight heparin, be employed early in disease progression.[26,27]
COVID-19 respiratory distress pathophysiology has been described as inflammation-induced pulmonary vasculitis, causing varying degrees of lung collapse secondary to edema and microthrombosis, which is characterized by bilateral ground-glass opacities on CT scan, resulting in ventilation-perfusion ratio (V/Q) mismatching and a significant shunt fraction.[28]
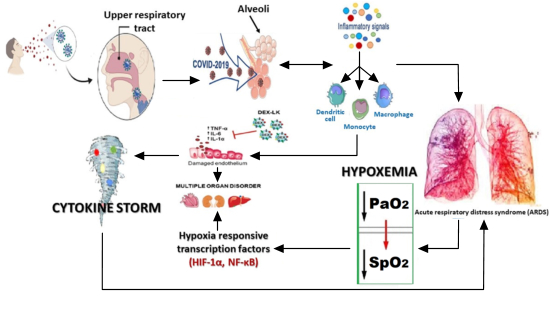
Cytokine-mediated lung endothelial and epithelial cell injury may damage the integrity of the blood–air barrier, thus promoting vascular permeability in addition to alveolar edema, infiltration by inflammatory cells, and hypoxemia. In COVID-19, as tissue breaks down, the walls of the lungs’ tiny air sacs become leaky and fill with fluid, causing pneumonia and starving the blood of oxygen. These phenomena also lead to a lack of oxygen supply in tissues and organs due to blood hypoperfusion. Moreover, proinflammatory cytokines overwhelm mitochondrial oxygen utilization, resulting in a change of metabolic pathway from oxidative phosphorylation to glycolysis, consequently triggering cells to change their mode of metabolism to glycolytic or anaerobic.[29]
Experimental rat models demonstrated that in hypoxemic micro-environmental conditions favored by enhanced HIF-1α activity, suppression of HIF-1 transcription or inhibition of its activity are perhaps effective in ameliorating inflammation caused by viral infection, such as in the lungs of COVID-19 patients.[24]
Systemic intermittent hypoxia is a life-threatening condition that happens in many diseases and situations, including chronic obstructive pulmonary disease, congestive heart failure and obstructive sleep apnea syndrome, all of which may coexist with SARS-CoV-2 infection in some patients.[30]
As previously discussed, hypoxemia can appear in early stages of COVID-19. Hypoxia is a common feature in inflammatory sites, which can eventually result in hypoxemia, leading in turn to induction of factors like HIF-1α. HIF-1α regulates important cellular processes, including cell proliferation, metabolism and angiogenesis. HIF-1α is activated during the immune response and plays an important role at the inflammation site by inducing pro-inflammatory cytokine production, leading to CS.[10,20,23–25,30] All the evidence connecting hypoxemia with CS highlights the importance of avoiding the former in COVID-19 patients as early as possible, to prevent development of the latter, by using non-invasive ventilation (NIV), as described in the following section.
Invasive or non-invasive ventilation in COVID-19 patients Over the past decade, NIV use has gained popularity in acute manifestations of chronic obstructive pulmonary disease (COPD).[31] Treatment for severe respiratory failure in COVID-19 patients has included early intubation and invasive ventilation, as this was deemed preferable and more effective than non-invasive options. Nevertheless, evolving evidence has shown that NIV may have a more significant and helpful role than first thought. NIV avoids the need for sedation, allows easier communication with patients and requires less intensive nursing care.[31]
There are three types of NIV: high-flow nasal oxygen (HFNO), BiPAP (bi-level positive airway pressure) and continuous positive airway pressure (CPAP).[31]
High-flow nasal oxygen HFNO therapy, administered through nasal cannulae, is a technique whereby heated and humidified oxygen is delivered at high flow rates. Such rates generate low levels of positive pressure in the upper airways, and the fraction of inspired oxygen (FIO2) levels can be attuned by varying the oxygen amount in the driving gas. High flow rates may also reduce physiological dead space by flushing expired CO2 from the upper airway, a process that may possibly explain the observed decline in respiration. In patients with acute respiratory failure, high-flow oxygen has been shown to result in better comfort and oxygenation than standard oxygen therapy delivered through a face mask.[32] This method may be useful to assure oxygenation during the time needed to prepare a ventilator.[4]
The 2012 Berlin definition of ARDS provided validated support for three levels of initial arterial hypoxemia that correlated with mortality in ventilated patients.[32] Since 2015, HFNO has become widely used as effective therapeutic support for ARDS, most recently in patients with severe COVID-19. It is noteworthy that the Berlin criteria propose the use of HFNO to treat ARDS, and not to prevent hypoxemia in the early stages of the disease.[32]
Nonetheless, HFNO use remains controversial in suspected and confirmed severe cases of COVID-19. As a result, the current national guidance in the UK does not recommend HFNO in COVID-19, citing lack of evidence proving its efficacy, high oxygen usage and risk of infection.[33]
Bilevel positive airway pressure BiPAP is commonly used in the care of patients with chronic respiratory disease, so it may be useful in COVID-19 patients. In COVID-19, BiPAP may have clinical use in improving the work of breathing. However, it carries the risk that inappropriate settings may allow the patient to take an excessively large tidal volume causing baro- and volutrauma. BiPAP allows for high driving pressure coupled with low driving pressure. Before commencing BiPAP, the patient must be assessed for pneumothorax, ideally by a chest x-ray or ultrasound. Due to the need for chest auscultation in COVID-19 patients, BiPAP is not recommended as it increases the risk of viral transmission to healthcare personnel.[34]
Continuous positive airway pressure CPAP is a simple and cost-effective intervention. Its use has been established for the care of other respiratory disorders but not for COVID-19 respiratory failure. At the beginning of the pandemic, international guidelines, including those from WHO, did not address the use of CPAP in COVID-19 patients, focusing instead on HFNO and invasive mechanical ventilation following intubation. In contrast, the UK National Institute for Health and Care Excellence guidance recommended the use of CPAP on April 9, although admitting evidence was lacking on its effectiveness.[33]
Nowadays, with CPAP equipment improved and commercially available, there is growing indication that it may be advantageous for avoiding hypoxemia in COVID-19 patients and thus halting disease progression, while reducing the need for invasive ventilation.[35,36] Ventilation systems have been developed in Cuba, CPAP among them, with the devices necessary for preventing aerosol dissemination, thus significantly reducing the possibility of contaminating health workers and other patients.[4]
Brusasco has recommended using CPAP in all patients presenting with signs of a severe intrapulmonary shunt (PaO2/FiO2 <200 or PaO2 <60/mmHg on Ventimask 50%) or increased effort in breathing (BF >30/min or dyspnea) before considering invasive ventilation.[37]
Furthermore, negative results found for CPAP patients are not directly related to its use, as shown by evidence that reports that the failure of CPAP to avert death or invasive mechanical ventilation was related to amplified blood levels of thrombo-inflammatory and cardiac injury/dysfunction biomarkers occurring in the intensive care unit (ICU).[38]
CPAP is usually initiated at a higher level than normal intrinsic pressure (approximately 5 cm H2O). For most ARDS patients, it is secondary to conditions that either collapse the alveoli or widen the gap between alveoli and surrounding blood vessels, thereby reducing gaseous exchange. Application of positive end expiratory pressure (PEEP) assists in maintaining patient airway pressure, thus preventing alveolar collapse and, in turn, increasing lung volumes and distending the lungs, reducing distance between alveoli and blood vessels, and improving gaseous exchange.[37] In severe COVID-19, initial CPAP settings have been suggested to begin at 10 cm H2O and 60% oxygen.[39,40]
Some authors have demonstrated that the use of CPAP through a helmet mask in ARDS has prevented intubation in a significant number of patients,[41] although this methodology is a more complex use of CPAP.
Nonetheless, an important caveat is the possibility of aerosol dissemination, spreading the virus to health workers and other patients.[41] Two European countries heavily affected by the pandemic, Spain and Italy, tried to quickly develop safe NIV systems to treat COVID-19 patients, and created an emergency CPAP mask. This device has a positive end-expiratory pressure (PEEP) valve and a Venturi connector fitted to a facial snorkel interface.[42,43] Other alternatives have been proposed such as simple face masks, Venturi masks, non-rebreather (NRB) masks, and masks with reservoir bags. It has been argued that CPAP, as non-invasive ventilation (delivered by a mask with air diffusers), has low risk of aerosolization, provided that there is good mask fit. Of course, it is important to follow step-by-step instructions on cleaning CPAP devices and masks.[18,23,43,44] These guidelines for health worker protection are documented in detail in the Cuban Protocol for COVID-19.[4]
Persistent cough and shortness of breath in early COVID-19 stages can lead to periods of hypoxemia and subsequently to CS. This may cause worsening in a substantial proportion of patients over a short period, leakproof clinical states, and lead to death from ARDS. In the case of COVID-19 patients suffering ARDS in ICUs, invasive ventilation is preferred and recommended.[4] Some authors have proposed that CPAP is a reasonable and effective therapeutic strategy that may potentially delay or even avert the need for intubation in many patients.[44]
As has already been discussed, there is a close interrelationship between hypoxemia and CS. CS generates additional hypoxia in tissues and organs, leading to a chain reaction between hypoxemia and CS.[15–18] Hence, our proposal is the use of CPAP as an NIV method, outside the ICU, as early as possible in the disease’s clinical evolution, when the first respiratory symptoms begin, to prevent periods of hypoxemia.[6,7,23] In Cuba, particularly, it is possible to use CPAP for these purposes, as COVID-19 protocols assure early admission of patients to isolation centers or hospitals, even when they are still asymptomatic,[4] and moreover, national production of ventilation systems has been initiated, including production of NIV equipment. Hence, clinicians can promptly detect the onset of respiratory symptoms, and are able to prescribe early CPAP use in these patients. This NIV method can be individually adjusted, depending on the intensity and frequency of respiratory symptoms, but it is crucial to consider times when patients are sleeping. According to the Cuban Protocol for COVID-19, the main complications of the disease generally occur after the second week of clinical evolution,[4] so there is time to prevent hypoxemia’s triggering of CS.
CONCLUSIONS
Based on the relationship between hypoxemia and CS, we recommend evaluating the use of CPAP in the early stages of COVID-19 disease, at the onset of first respiratory symptoms (persistent cough and/or shortness of breath) as a personalized treatment to avert hypoxemia in patients evaluated by pulse oximetry or arterial gasometry. This would prevent hypoxemia’s triggering effect on CS, thus potentially avoiding ARDS, multi-organ failure and death.