INTRODUCTION Unlike most high-income countries where subtype B viruses predominate, the Cuban HIV-1 epidemic is characterized by a great diversity of subtypes and circulating recombinant forms. Some studies have shown that HIV variants exhibiting a preference for the CXCR4 co-receptor (X4-tropic) could have impacts on disease pathogenesis, with clinical implications for antiviral treatment plans. Determination of HIV co-receptor tropism is crucial for clinicians in deciding whether maraviroc is an appropriate antiviral.
OBJECTIVE Characterize V3 sequence variability and its relation to viral tropism across different subtypes circulating in Cuba and explore how this may affect treatment success with maraviroc.
METHODS We designed a cross-sectional study that included 72 plasma samples obtained at the Pedro Kourí Tropical Medicine Institute in Havana, Cuba. We sequenced the C2V3 env region and assessed subtype based both on env and pol sequences; tropism was predicted by Geno2pheno analysis.Additionally, 35 V3-loop Cuban sequences, obtained from a previous study, were incorporated into the analysis. Statistical associations among virological, clinical and epidemiological variables were assessed by a chi-square test.
RESULTS Tropism prediction for 72 variants revealed that CRF19_cpx was associated with dual-tropic R5X4 viruses (p = 0.034). Moreover, when 35 sequences from a former study were added, the association was significant not only for R5X4 (p = 0.019) but also for X4-tropic variants (p = 0.044). Alignment of 107 V3-loop sequences showed wide diversity among the different HIV-1 subtypes circulating in Cuba.
CONCLUSIONS In accordance with G2P, CRF19_cpx is a genetic variant with a high proportion of X4 and R5X4-tropic viruses. The results from the present study suggest that the Cuban recombinant could be a more pathogenic variant and that maraviroc may not be suitable for patients infected with CRF19_cpx.
KEYWORDS HIV, CCR5 receptor antagonists, maraviroc, HIV envelope glycoprotein gp120, Cuba
ABSTRACT INTRODUCTION Unlike most high-income countries where subtype B viruses predominate, the Cuban HIV-1 epidemic is characterized by a great diversity of subtypes and circulating recombinant forms. Some studies have shown that HIV variants exhibiting a preference for the CXCR4 co-receptor (X4-tropic) could have impacts on disease pathogenesis, with clinical implications for antiviral treatment plans. Determination of HIV co-receptor tropism is crucial for clinicians in deciding whether maraviroc is an appropriate antiviral.
OBJECTIVE Characterize V3 sequence variability and its relation to viral tropism across different subtypes circulating in Cuba and explore how this may affect treatment success with maraviroc.
METHODS We designed a cross-sectional study that included 72 plasma samples obtained at the Pedro Kourí Tropical Medicine Institute in Havana, Cuba. We sequenced the C2V3 env region and assessed subtype based both on env and pol sequences; tropism was predicted by Geno2pheno analysis.
Additionally, 35 V3-loop Cuban sequences, obtained from a previous study, were incorporated into the analysis. Statistical associations among virological, clinical and epidemiological variables were assessed by a chi-square test.
RESULTS Tropism prediction for 72 variants revealed that CRF19_cpx was associated with dual-tropic R5X4 viruses (p = 0.034). Moreover, when 35 sequences from a former study were added, the association was significant not only for R5X4 (p = 0.019) but also for X4-tropic variants (p = 0.044). Alignment of 107 V3-loop sequences showed wide diversity among the different HIV-1 subtypes circulating in Cuba.
CONCLUSIONS In accordance with G2P, CRF19_cpx is a genetic variant with a high proportion of X4 and R5X4-tropic viruses. The results from the present study suggest that the Cuban recombinant could be a more pathogenic variant and that maraviroc may not be suitable for patients infected with CRF19_cpx.
KEYWORDS HIV, CCR5 receptor antagonists, maraviroc, HIV envelope glycoprotein gp120, Cuba
INTRODUCTION During entry into the host cell, HIV-1 surface glycoprotein gp120 interacts with the CD4 receptor and, generally, with one of two chemokine co-receptors: CCR5 (chemokine [C-C] motif receptor 5) or CXCR4 (CXC chemokine receptor 4). This interaction defines viral tropism in R5-tropic or X4-tropic strains, respectively.[1,2] Co-receptor selectivity is determined by genetic sequences within the HIV-1 gp120, particularly in a highly variable and structurally flexible region called the ‘V3 loop’, which is involved in co-receptor binding.[3,4]
Viral tropism has been proposed as an influence on HIV-1 pathogenesis and replication, with implications for treatment. R5-tropic variants have shown predominance during early stages of the disease, are generally not syncytium-inducing and have low replication capacity.[5,6] It is believed that during the course of infection, R5 viruses experience a switch in tropism and thus, X4 variants emerge, characterized by syncytium induction and higher replication capacity. In addition, a third group of viruses has been classified as dual-tropic or R5X4-tropic variants, referring to their ability to interact with both CCR5 and CXCR4 co-receptors.[2,7]
IMPORTANCE CRF19_cpx is one of the most prevalent HIV-1 subtypes circulating in Cuba. X4- and dual-tropic viruses prevail in CRF19_cpx-infected patients, which suggest this may be a more pathogenic variant and less susceptible to treatment with maraviroc.
Determining viral tropism is important when choosing antivirals like maraviroc, the first CCR5 inhibitor approved for treatment of R5-tropic HIV-1 infection in both treatment-naive and treatment-experienced adult patients. However, maraviroc does not inhibit entry of X4-tropic or dual-tropic HIV-1 viruses and a test that predicts HIV-1 co-receptor use is highly recommended before treatment prescription.[1,8,9]
Two different methods are employed to predict co-receptor use. Phenotypic assays have greater accuracy; however, they are expensive, time-consuming, and require special facilities and trained personnel. On the other hand, genotypic assays rely on bioinformatic tools to predict co-receptor use based mainly on the sequence of the gp120’s V3 loop.[10,11] These latter methods are rapid and easier to use; however, their development has been based mostly on sequences from HIV-1 subtype B isolates, without considering the viral diversity of the epidemic within countries.[1,12–14]
In Cuba, the HIV-1 epidemic is atypical when compared to the rest of the Latin American and Caribbean region. Cuba has a great diversity of HIV-1 subtypes including many recombinant forms (CRFs) such as BG recombinants (CRF20_BG, CRF23_BG and CRF24_BG) and complex CRFs, such as CRF18_cpx and CRF19_cpx.[15,16]
A Cuban study identified that in patients harboring CRF19_cpx viruses, CXCR4-using variants prevailed and disease progression to AIDS occurred more rapidly than in patients harboring subtype B viruses.[15] An association between HIV-1 subtype and co-receptor use has also been demonstrated in other studies.[2,6,17]
The objective of this study was to characterize V3 sequence variability across different Cuban HIV-1 subtypes and its relation to viral tropism in the context of the Cuban epidemic, in order to achieve a more complete understanding of HIV-1 pathogenesis and improved management of antiviral treatment for Cuban patients.
METHODS Study Design We analyzed additional plasma samples from Cuban HIV-1–infected patients in order to extend our previous analysis on prevalent subtypes[18] and include data on viral tropism. Samples were selected from HIV-1–infected patients who were tested for antiretroviral resistance at the Pedro Kourí Tropical Medicine Institute (IPK) in Havana, Cuba, from January 2015 through July 2016. Those patients infected with the following subtypes and recombinant forms (classified regarding pol sequence employed in resistance testing) were selected: subtype B, CRF_BG (for the purpose of this study CRF20_BG, CRF23_BG and CRF24_BG were grouped together as CRF_BG), CRF18_cpx and CRF19_cpx.[15,16,19] After selection, a total of 72 patients were included and C2V3 sequences of the glycoprotein gp120 were obtained and employed to assess viral subtype regarding env region and predict co-receptor use.
An additional group of 35 V3-loop sequences from Cuban patients[18] was included for analysis of association between viral subtype and tropism, to better characterize V3 sequence variability. We decided to include these sequences because they corresponded to a similar study performed by our group from January 2014 through January 2015.[18] For sequence selection, the same criteria mentioned above were applied. We included a total of 14 sequences from subtype B, 13 from CRF_BG, 2 from CRF18_cpx and 6 from CRF19_cpx, classified according to pol sequence.
Epidemiological, clinical, virological and immunological information Epidemiological and clinical data were collected at sampling as well as from a screening of selected databases stored at IPK (SIDATRAT). Patient viral load and CD4+ cell counts were performed as previously described.[18]
HIV sequencing and subtype assignment RNA extraction from plasma samples, C2V3 amplification and sequencing were obtained as previously described.[18] Sequences were edited with Sequencher 4.9 (Gene Codes Coorporation, USA) employing the HXB2 strain (Genbank access number K03455.1, at https://www.ncbi.nlm.nih.gov/genbank) as the reference sequence. Subtype was assessed via COMET version 2 (Luxembourg Institute of Health, Luxembourg) and REGA version 3 (Stanford University, USA).[20,21] In addition, subtype assignment was confirmed by manual phylogenetic analysis employing PhyML/One Click software (Institut Pasteur, France).[22] Sequences and HIV-1 subtype in the pol region were obtained from antiretroviral resistance testing routinely performed in our laboratory at IPK.[23]
Prediction of co-receptor use Tropism prediction based on V3-loop sequence was performed using the Geno2pheno (G2P) algorithm (Max Planck Institute, Germany). The false positive rate (FPR) that defines the probability of classifying an R5 virus (incorrectly) as an X4 virus was set at a cut-off value of 5% following German guidelines.[15,24,25] Patients with FPR ≤5% were considered infected with X4 viruses; patients with FPR ≥20% were predicted to harbor R5 viruses; and patients with FPR values >5% and <20% were considered to have dual-tropic R5X4 virus infections. Additionally, V3 net charge and 11/25 rule were employed in predicting viral tropism.[26]
Statistical analysis Comparison of FPR values among groups was performed using GraphPad Prism version 5 software (GraphPad, USA) and the non-parametric Kruskall Wallis Test and Dunn Test for post-hoc comparisons. Analysis of the association between co-receptor use, subtype, clinical, virological and immunological variables was performed via a chi-square test using SPSS v.22 (IBM, USA). For all comparisons, a p-value ≤0.05 was considered statistically significant.
Ethics Study protocols were designed in accordance with the Helsinki Declaration and approved by the IPK Ethics Committee.
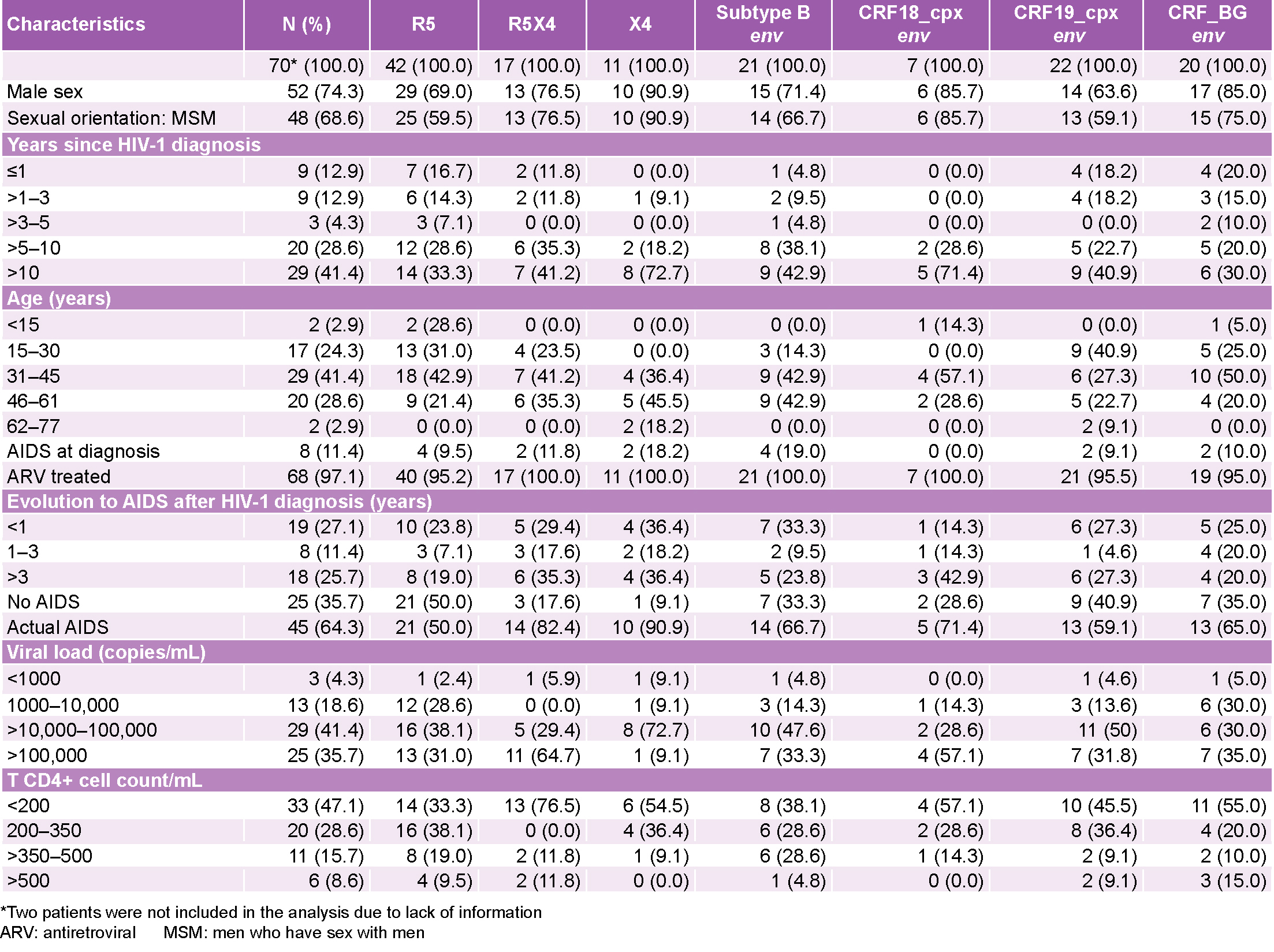
RESULTS Study population characteristics The study universe consisted of 72 plasma samples corresponding to the same number of patients. Two patients lacked clinical and epidemiological information, and were therefore only included in the analysis of co-receptor tropism prediction and its association with HIV-1 subtype. For the remaining 70 patients, epidemiological, virological and immunological information demonstrated that the majority were male (74.3%), men who have sex with men (MSM, 68.6%), aged 31–45 years (41.4%) who had been diagnosed with HIV-1 >10 years ago (Table 1); 11.4% of patients had AIDS at the time of HIV-1 diagnosis and 64.3% had AIDS at the time of sampling. For 41.4% of patients, viral load at sampling was 10,000–100,000 copies/mL and 47.1% had a T CD4+ cell count ≤200 cells/mL. These patients had been assigned a previous HIV-1 subtype based on the pol sequence. Twenty patients were infected with subtype B, 24 with CRF19_cpx, 9 with CRF18_cpx and 19 with CRF_BG.
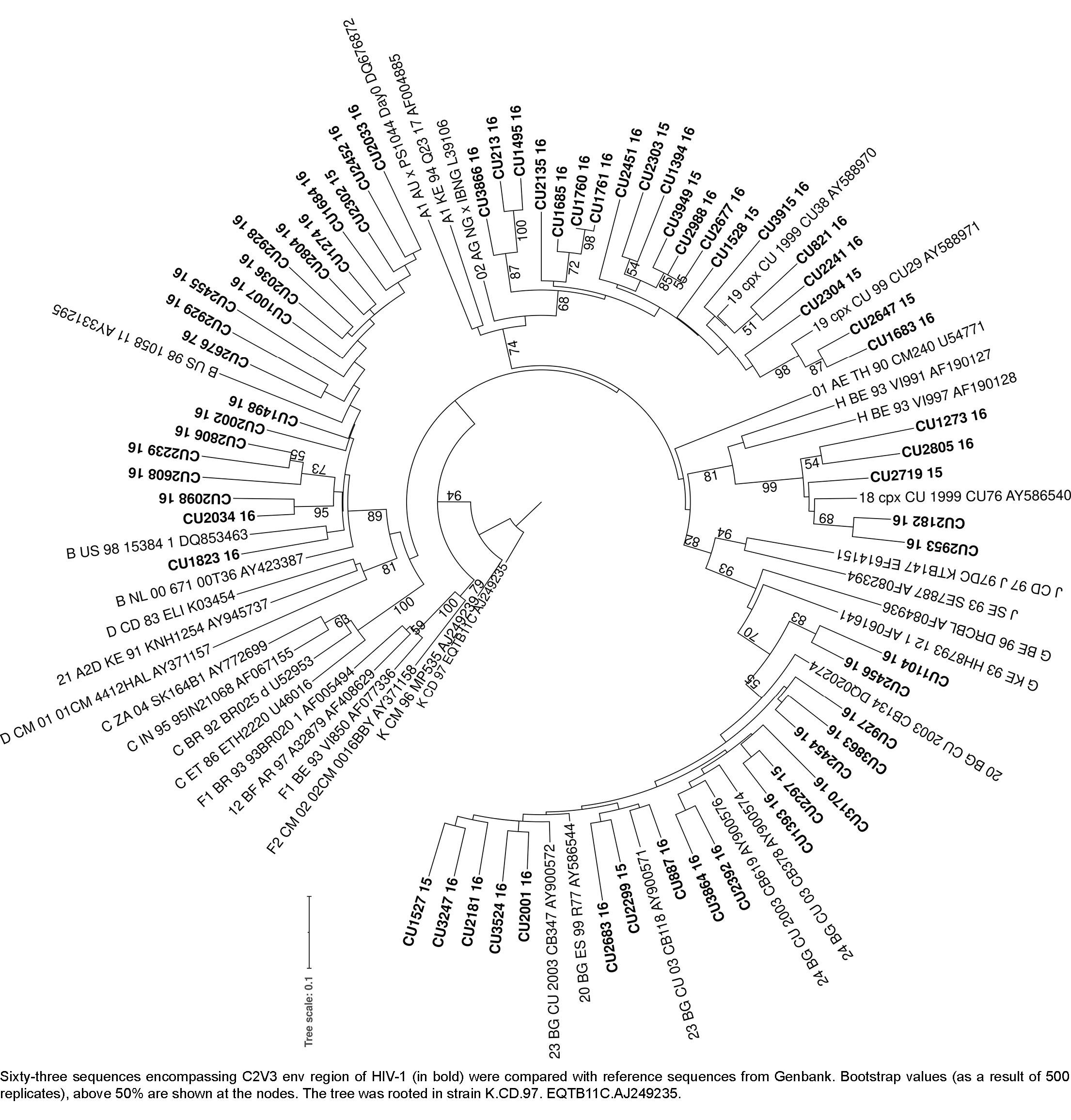
Env subtyping Samples were processed to obtain partial env sequences. Of these, 12.5% (9/72) samples had a C2V3 region too short for phylogenetic subtyping (Figure 1), but were still able to be subtyped using REGA version 3 and COMET version 2 bioinformatics platforms.
After env subtyping, 21 sequences were subtype B, 23 were CRF19_cpx, 7 were CRF18_cpx, and 21 were CRF_BG. Considering both pol and env sequences, an overall subtype was assigned to samples, resulting in 19 classified as subtype B, 21 as CRF19_cpx, 7 as CRF18_cpx, 18 as CRF_BG and 7 as unique recombinant forms (URF) since they had different subtypes in pol and env sequences.
Co-receptor use prediction Co-receptor use was analyzed based on G2P algorithm, 11/25 rule and V3 net charge. Co-receptor prediction by G2P showed that 59.7% (43/72) of analyzed samples were R5-tropic viruses, 16.7% (12/72) were X4-tropic viruses, 23.6% (17/72) were classified as dual tropic viruses and 40.3% (29/72) were predicted to be dual-tropic or X4 variants (Table 2). There was a 42.9% agreement in predicting X4-tropic viruses between G2P and the 11/25 rule for subtype B, while there was 50.0% agreement for non-B subtypes. Calculation of V3-loop net charge showed a 42.9% agreement with G2P for subtype B and 50.0% agreement for non-B subtypes.
Figure 1: Phylogenetic tree constructed by PhyML/One Click software[22]
Analysis of co-receptor use by G2P showed that CRF19_cpx viruses were more likely to be R5X4-tropic (p = 0.034; OR = 3.295; CI: 1.065–10.191) than other subtypes. This statistical difference was strengthened when we analyzed R5X4 and X4 together using variants (p = 0.015; OR = 3.526; CI: 1.253–9.921). No other statistical association was found for remaining subtypes. A comparison of FPR values across subtypes also showed that CRF19_cpx had the lowest mean value (Figure 2), even though the difference was only significant with regard to CRF18_cpx and CRF_BG.
Patient epidemiological, virological and immunological information was analyzed in relation to co-receptor use and viral env subtype (Table 3). Nevertheless, few statistical associations were found.
X4-tropic viruses were associated with >10 years since diagnosis (p = 0.022), with a viral load at >10,000–100,000 copies/mL (p = 0.022) and with AIDS at the time of sampling (p = 0.045). R5-tropic viruses prevailed in non-AIDS patients (p = 0.002), in those with viral loads at 1,000–10,000 copies/mL (p = 0.008) and a T CD4+ cell count at 200–350 cells/mL (p =0 .031). R5X4 viruses corresponded to patients with a viral load >100,000 copies/mL (p = 0.004) and with T CD4+ cell counts <200 cells/mL (p = 0.005). CRF19_cpx prevailed in patients who were 15–30 years old (p = 0.028).
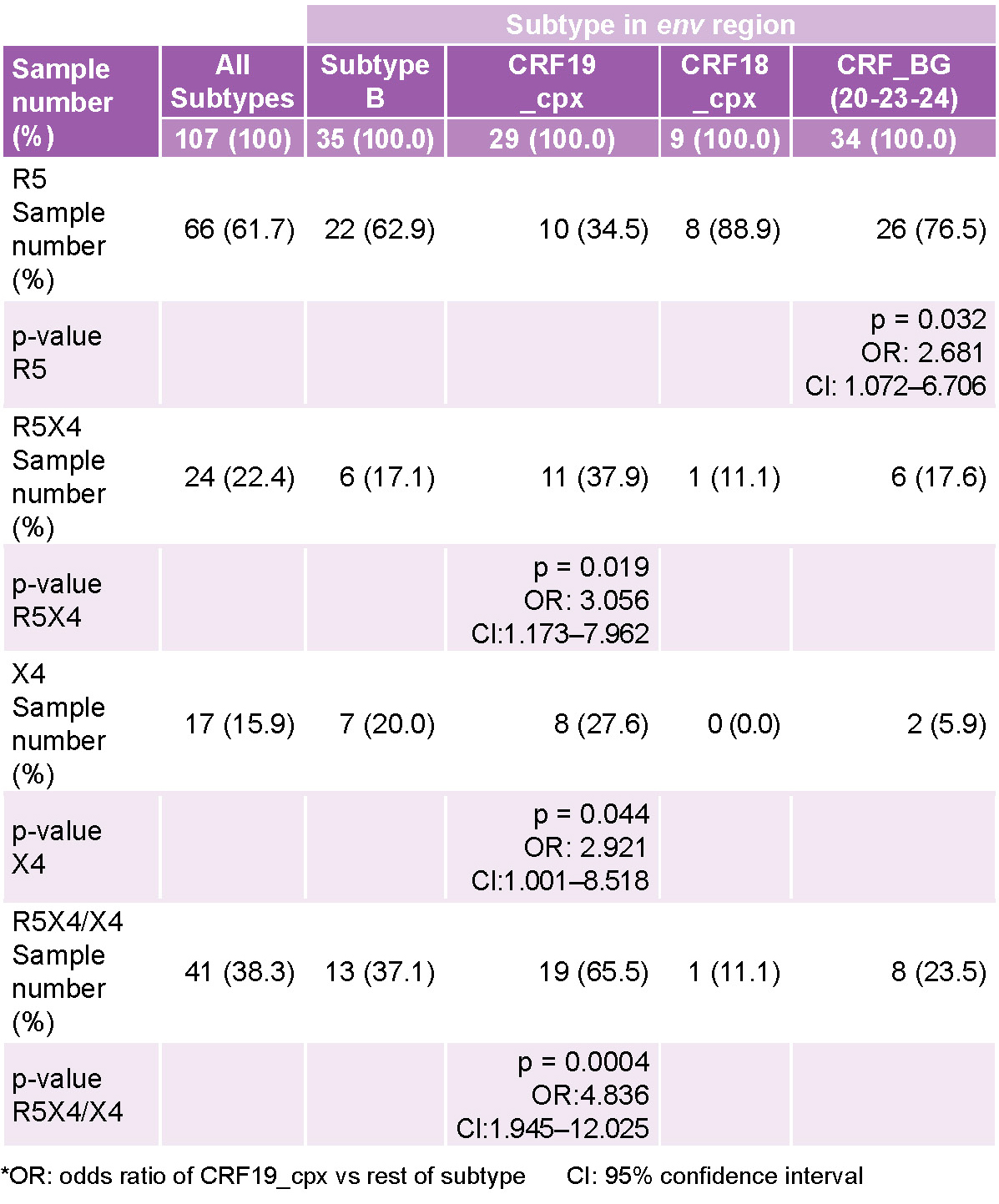
Our analysis incorporated an additional 35 HIV-1 V3-loop sequences from Cuban patients, obtained from January 2014 through January 2015 under the same criteria outlined above. Thus, this set of 107 sequences spanned a period from January 2014 through July 2016. Determination of co-receptor use in this group of viruses (Table 4) revealed an association of CRF19_cpx with X4-tropic viruses (p = 0.044), R5X4-tropic viruses (p = 0.019) or either R5X4 or X4 (p = 0.0004). Additionally, most CRF_BG were R5-tropic viruses (p = 0.032).
Genetic diversity of V3 loop After alignment of 107 V3-loop sequences, we identified some differences in aminoacidic patterns expressed among subtypes. Arginine (R) at position 13 was more prevalent in CRF_BG (p ≤0.0001) and CRF19_cpx (p ≤0.0001) than in subtype B (Supplementary Figure 3).
Valine (V) at positions 12 and 19 prevailed in CRF19_cpx compared to subtype B (p ≤0.0001). On the other hand, for non-B subtypes (CRF19_cpx, CRF18_cpx and CRF_BG), the sequence GPGQ in the tip of the V3 loop was more frequent than GPGR, characteristic of subtype B (p <0.0001). Some motifs found at the tip of the loop other than GPG were RPA/G, APG, GAG, DAG, GRG and GLG. All sequences with APG motifs were R5-tropic, while all CRF19_cpx sequences with substitution 34Y were either X4- or R5X4-tropic strains. However, these differences were not significant.
DISCUSSION CRF19_cpx is currently one of the most prevalent subtypes circulating in Cuba. This recombinant is thought to be of African origin, resulting in a mosaic of subtypes A1, D and G; though the virus has spread most successfully in Cuba. An earlier study performed in our laboratory showed an association between infection with CRF19_cpx and rapid progression to AIDS.[15] These results led us to hypothesize that this recombinant virus may be a more pathogenic form of HIV-1. Although it has not been demonstrated whether X4 viruses are a cause or rather a consequence of immune system deterioration, many studies reported co-receptor use preference based on the subtype.[6,17] Based on G2P prediction, we found that CRF19_cpx had preferential tropism towards R5X4, which has been described as capable of using both CCR5 and CXCR4 co-receptors for entry into the host cell.[4]
When we expanded our analysis to 107 samples, we found CRF19_cpx to be associated with dual-tropic forms of the virus and also ratified our previous observations about a link between these viruses and X4-tropic variants.
Since dual-tropic viruses have been considered an intermediate stage during the switch from R5 to X4 variants that may even result from intrapatient recombination once X4 viruses emerge in the host, CRF19_cpx association is expected not only with X4 but also with R5X4 viruses. In addition, understanding that some patients never experience this switch in tropism and continue harboring R5 viruses,[7,27] we speculate that some HIV-1 subtypes or CRFs, such as CRF19_cpx, are likely to evolve towards dual-tropic and X4 variants during the course of infection. Whether this evolution is faster with respect to other subtypes or is actually related to HIV-1 pathogenesis has yet to be demonstrated. Furthermore, the cause of this subtype-dependent co-receptor use may be explained by intrinsic virological properties of each subtype (i.e. enhanced replicative capacity, antigenic diversity) or by the differential effects of viruses on host immune systems, which may eventually lead to expansion of the X4 virus population.[27]
Even though we measured no direct association between CRF19_cpx and disease progression stage, R5X4 viruses were related to a CD4+ cell count ≤200 cells/mL. Characteristically, X4 viruses have been correlated with advanced disease stage and low levels of CD4+ T cell count.[28–30] Nevertheless, it has been hypothesized that dual-tropic viruses could represent variants with the same potential as R5 viruses to evade immune response and also infect cells expressing CXCR4. The broadening in cell tropism of the viral population to include CXCR4-expressing cells would result in increased CD4+ T cell death and further immune impairment.[7]
Figure 1: Phylogenetic tree constructed by PhyML/One Click software[22]
Table 2: Co-receptor use and subtype distribution prediction
Figure 2: Alignment of 107 V3-loop amino acid sequences obtained from Cuban HIV-1 patients
Table 3: Clinical, virological and immunological variable distribution according to co-receptor prediction and subtype
Table 4: Co-receptor use prediction distributed across different subtypes in 107 HIV-1 Cuban sequences
To our knowledge, this is the first report on the association of CRF_BG viruses and R5 tropism. Previously, a link between CRF18_cpx viruses and R5 tropism had been reported.[15] We found no significant relationship between those variables in the current study.
We also observed some changes in the aminoacidic sequence of the V3 loop among different subtypes. Particularly, some motifs other than GPG were found at the tip of the loop. In accordance with previous observations, GPGR motifs prevailed in subtype B, while the GPGQ motif was predominant among Cuban recombinants.[31,32] The GPGR motif is a very important target of neutralizing antibodies in subtype B viruses, so its difference with other subtypes should be considered for assessing monoclonal antibodies and peptide vaccine design.
In 1997, Milich et al. reported a high frequency of valine (V) at position 19 in syncytium-inducing viruses. According to these authors, the interaction between 19V and phenylalanine (F) at position 20 would contribute to a switch in tropism from non-syncytium–inducing to syncytium-inducing viruses.[33] This hypothesis could also explain the association between CRF19_cpx viruses and R5X4 and X4 tropism found in the current study. Considering that almost all sequences analyzed had V19, we could ask ourselves if this recombinant is capable of evolving to a change in tropism faster than other subtypes.
This study has some limitations. The number of sequences we have obtained so far is still small for ascertaining an association between co-receptor tropism and subtype; hence results need to be confirmed by future research including a greater number of patients. Additionally, currently-employed tools for HIV-1 tropism prediction, including G2P, were developed on the basis of a restricted set of subtypes, mainly subtypes B and C.[1] Therefore, their accuracy in predicting tropism for other subtypes and recombinant forms including the ones circulating in Cuba have to be assessed in the future based on their correlation with phenotypic methods. A phenotypic test was not performed due to restricted availability.
In Cuba, maraviroc could be a treatment alternative for patients experiencing failure with other HIV-1 drugs or be considered an option in combination with other regimens; however determining HIV-1 co-receptor use is mandatory before its prescription.[1,8,34] A more thorough understanding of the possible associations between co-receptor tropism and subtypes circulating in Cuba, together with phenotypic assays and the possible creation of new bioinformatic algorithms more suitable for Cuban HIV-1 recombinants’ tropism prediction would facilitate proper decisions regarding treatment choice with maraviroc or other co-receptor inhibitors.
CONCLUSION In the current study, 72 subtypes obtained from Cuban HIV-1 infected patients were sequenced and tropism was predicted employing a G2P bioinformatic tool.
Additionally, 35 other viruses that were sequenced in a former study were included for analysis. An association between CRF19_cpx and X4 and R5X4 tropism was found, which suggests that patients infected with this recombinant are probably less suitable to receive maraviroc than those infected with other HIV-1 subtypes. The study reinforces findings from previous studies on this subject and highlights the importance of HIV-1 diversity when considering pathogenesis and treatment options.[1,35,36]
ACKNOWLEDGMENTS Thanks to Dr Ursula Dietrich for reviewing the manuscript and for her helpful comments.
SEQUENCE DATA AND SUPPLEMENTARY MATERIAL Sequences obtained in the present study are deposited in Genbank under access numbers MT785557–MT785663.
Supplementary Figure 3 : Alignment of 107 V3 loop amino acid sequences obtained from Cuban HIV-1 patients. Supplementary Figure 3 is available upon request from the corresponding author.
Riemenschneider M, Cashin KY, Budeus B, Sierra S, Shirvani-Dastgerdi E, Bayanolhagh S, et al. Genotypic Prediction of Co-receptor Tropism of HIV-1 Subtypes A and C. Sci Rep [Internet]. 2016 [cited 2020 Dec 3];6:24883. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4850382/pdf/srep24883.pdf
Woollard SM, Kanmogne GD. Maraviroc: a review of its use in HIV infection and beyond. Drug Des Devel Ther [Internet]. 2015 Oct 1 [cited 2020 Dec 2];9:5447–68. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/26491256/
Mild M, Esbjornsson J, Fenyo EM, Medstrand P. Frequent intrapatient recombination between human immunodeficiency virus type 1 R5 and X4 envelopes: implications for coreceptor switch. J Virol [Internet]. 2007 Apr [cited 2020 Dec 16];81(7):3369–76. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1866041/pdf/1295-06.pdf
Phuphuakrat A, Phawattanakul S, Pasomsub E, Kiertiburanakul S, Chantratita W, Sungkanuparph S. Coreceptor tropism determined by genotypic assay in HIV-1 circulating in Thailand, where CRF01_AE predominates. HIV Med [Internet]. 2014 May [cited 2020 Dec 15];15(5):269–75. Available at: https://onlinelibrary.wiley.com/doi/epdf/10.1111/hiv.12108
Asin-Milan O, Chamberland A, Wei Y, Haidara A, Sylla M, Tremblay CL. Mutations in variable domains of the HIV-1 envelope gene can have a significant impact on maraviroc and vicriviroc resistance. AIDS Res Ther [Internet]. 2013 Jun 7 [cited 2020 Dec 20];10(1):15. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3700831/pdf/1742-6405-10-15.pdf
Recordon-Pinson P, Soulie C, Flandre P, Descamps D, Lazrek M, Charpentier C, et al. Evaluation of the genotypic prediction of HIV-1 coreceptor use versus a phenotypic assay and correlation with the virological response to maraviroc: the ANRS GenoTropism study. Antimicrob Agents Chemother [Internet]. 2010 Aug [cited 2020 Dec 3];54(8):3335–40. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2916345/pdf/0148-10.pdf
Dina J, Raymond S, Maillard A, Le Guillou-Guillemette H, Rodalec A, Beby-Defaux A, et al. Algorithm-based prediction of HIV-1 subtype D coreceptor use. J Clin Microbiol [Internet]. 2013 Sep [cited 2020 Dec 15];51(9):3087–9. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3754628/pdf/zjm3087.pdf
Kourí V, Khouri R, Alemán Y, Abrahantes Y, Vercauteren J, Pineda-Pena AC, et al. CRF19_cpx is an evolutionary fit HIV-1 variant strongly associated with rapid progression to AIDS in Cuba. EBioMedicine [Internet]. 2015 Jan 28 [cited 2020 Dec 16];2(3):244–54. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4484819/pdf/main.pdf
Pérez L, Kouri V, Alemán Y, Abrahantes Y, Correa C, Aragones C, et al. Antiretroviral drug resistance in HIV-1 therapy-naive patients in Cuba. Infect Genet Evol [Internet]. 2013 Jun [cited 2020 Dec 15];16:144–50. Available at: https://www.sciencedirect.com/science/article/abs/pii/S1567134813000361
Fenyö EM, Esbjörnsson J, Medstrand P, Jansson M. Human immunodeficiency virus type 1 biological variation and coreceptor use: from concept to clinical significance. J Intern Med [Internet]. 2011 Dec [cited 2020 Dec 17];270(6):520–31. Available at: https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1365-2796.2011.02455.x
Kourí V, Alemán Y, Pérez L, Pérez J, Fonseca C, Correa C, et al. High frequency of antiviral drug resistance and non-B subtypes in HIV-1 patients failing antiviral therapy in Cuba. J Clin Virol [Internet]. 2012 Dec 5 [cited 2020 Dec 2];55(4):348–55. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4225368/pdf/JIAS-17-19754.pdf
Lemoine F, Correia D, Lefort V, Doppelt-Azeroual O, Mareuil F, Cohen-Boulakia S, et al. NGPhylogeny.fr: new generation phylogenetic services for non-specialists. Nucleic Acids Res [Internet]. 2019 Apr 27 [cited 2020 Dec 3];47(W1):W260–W5. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6602494/pdf/gkz303.pdf
Alemán Y, Vinken L, Kouri V, Pérez L, Álvarez A, Abrahantes Y, et al. Performance of an in-house human immunodeficiency virus type 1 genotyping system for assessment of drug resistance in Cuba. PLoS One [Internet]. 2015 Feb 11 [cited 2020 Dec 14];10(2):e0117176. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4324769/pdf/pone.0117176.pdf
Lengauer T, Sander O, Sierra S, Thielen A, Kaiser R. Bioinformatics prediction of HIV coreceptor usage. Nat Biotechnol [Internet]. 2007 Dec [cited 2020 Dec 4];25(12):1407–10. Available at: https://www.nature.com/articles/nbt1371
Matume ND, Tebit DM, Gray LR, Hammarskjold ML, Rekosh D, Bessong PO. Next generation sequencing reveals a high frequency of CXCR4 utilizing viruses in HIV-1 chronically infected drug experienced individuals in South Africa. J Clin Virol [Internet]. 2018 Jun [cited 2020 Dec 17];103:81–7. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7229640/pdf/nihms-1584881.pdf
Hayashida T, Tsuchiya K, Kikuchi Y, Oka S, Gatanaga H. Emergence of CXCR4-tropic HIV-1 variants followed by rapid disease progression in hemophiliac slow progressors. PLoS One [Internet]. 2017 May 4 [cited 2020 Dec 16];12(5):e0177033. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5417636/pdf/pone.0177033.pdf
Gupta S, Neogi U, Srinivasa H, Banerjea AC, Shet A. HIV-1 coreceptor tropism in India: increasing proportion of X4-tropism in subtype C strains over two decades. J Acquir Immune Defic Syndr [Internet]. 2014 Apr 1 [cited 2020 Dec 17];65(4):397–404. Available at: https://journals.lww.com/jAIDS/Fulltext/2014/04010/HIV_1_Coreceptor_Tropism_in_India Increasing.3.aspx
Guo JL, Yan Y, Zhang JF, Ji JM, Ge ZJ, Ge R, et al. Co-receptor tropism and genetic characteristics of the V3 regions in variants of antiretroviral-naive HIV-1 infected subjects [Internet]. Epidemiol Infect. 2019 Jan [cited 2020 Dec 18];147:e181. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6518647/pdf/S0950268819000700a.pdf
Morgado MG, Guimaraes ML, Gripp CB, Neves Junior I, Costa CI, dos Santos VG, et al. Polymorphism of the predictive antigenic sites on the V3 loop of Brazilian HIV-1 subtype B strains. HEC/FIOCRUZ AIDS Clinical Research Group. Mem Inst Oswaldo Cruz [Internet]. 1996 May–Jun [cited 2020 Dec 18];91(3):339–42. Available at: https://www.scielo.br/pdf/mioc/v91n3/15.pdf
Milich L, Margolin BH, Swanstrom R. Patterns of amino acid variability in NSI-like and SI-like V3 sequences and a linked change in the CD4-binding domain of the HIV-1 Env protein. Virology [Internet]. 1997 Dec 8 [cited 2020 Dec 18];239(1):108–18. Available at: https://linkinghub.elsevier.com/retrieve/pii/S0042-6822(97)98821-8
Heera J, Valluri SR, Craig C, Fang A, Thomas N, Meyer RD, et al. First prospective comparison of genotypic versus phenotypic tropism assays in predicting virologic responses to maraviroc in a phase 3 study. New Microbiol [Internet]. 2019 Apr [cited 2020 Dec 19];41(2):101–7. Available at: http://www.newmicrobiologica.org/PUB/allegati_pdf/2019/2/101.pdf
Esbjörnsson J, Månsson F, Martínez-Arias W, Vincic E, Biague AJ, da Silva ZJ, et al. Frequent CXCR4 tropism of HIV-1 subtype A and CRF02_AG during late-stage disease–indication of an evolving epidemic in West Africa. Retrovirology [Internet]. 2010 Mar 22 [cited 2020 Dec 18];7:23. DOI: 10.1186/1742-4690-7-23. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2855529/pdf/1742-4690-7-23.pdf
THE AUTHORS Yenisleidys Martínez-Montesino, microbiologist with a master’s degree in virology. Specialist in chemical, physical and mechanical assays. Virology Department, Pedro Kourí Tropical Medicine Institute (IPK), Havana, Cuba. https://orcid.org/0000-0001-8183-3685
Vivian Kourí-Cardellá (Corresponding author: vkouri@ipk.sld.cu), physician specializing in microbiology with a master’s degree in virology and infectious diseases, a doctorate in virology and an advanced doctorate in science. Full professor and senior researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0001-7878-7542
Lissette Pérez-Santos, microbiologist with a master’s degree in virology and a doctorate in health sciences (virology). Associate professor and senior researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-5127-2167
Yanet Pintos-Saavedra, microbiologist with a master’s degree in virology. Assistant researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-9814-3477
Yoan Alemán-Campos, biochemist with a master’s degree in virology. Assistant professor and adjunct researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0001-7389-1535
Yudira Soto-Brito, microbiologist with a master’s degree in virology and a doctorate in health sciences (virology). Associate professor and senior researcher, Virology Department, IPK, Havana, Cuba. https://orcid.org/0000-0003-2426-9517
Submitted: July 13, 2021 Approved: July 21, 2021 Disclosures: None
Martínez-Montesino Y, Kourí-Cordellá V, Pérez-Santos L, Han R, Pintos-Saavedra Y, Alemán-Campos Y, et al. Subtype-dependent co-receptor tropism in Cuban HIV-1–infected patients: implications for Maraviroc treatment. MEDICC Rev. 2021 Jul-Oct;23(3):29–36. DOI: 10.37757/MR2021.V23.N3.6
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.