INTRODUCTION The Cuban national program for childhood immunizations began in 1962 and has included a surveillance system for monitoring adverse events following immunization since 1999. The expected rate of adverse events following childhood immunization in Cuba is 50 per 100,000 vaccine doses administered. In 2017, Pinar del Río Province reported higher-than-expected rates of adverse events, which motivated this study on their frequency and types.
OBJECTIVE Characterize adverse events following immunization reported in children in Pinar del Río Province in 2017.
METHODS We examined reports of adverse events following immunization in children from 2 months through 14 years of age in Pinar del Río Province, Cuba, from January 1, 2017 through December 31, 2017. We found 487 adverse events that met the criteria established by the national surveillance system. Information was obtained from epidemiological surveys of adverse events following immunization in Pinar del Río Province municipalities. Recorded were age, municipality, signs and symptoms, vaccine type, number of doses, anatomical site and route of vaccine administration, and the institution where the child was vaccinated. We estimated proportions for intensity and frequency related to vaccination, and calculated rates for 100,000 vaccine doses administered. We then compared the rates of observed adverse events with those of expected events.
RESULTS The overall rate of adverse events was 305.6 per 100,000 doses administered. Highest rates were reported in children aged <1 year (580.9 per 100,000 doses administered); in Guane Municipality (610 per 100,000 doses), for the pentavalent (DTwP-HB-Hib) vaccine (1567.7 per 100,000 doses), and in applications to the anterolateral quadrant of the thigh (772.5 per 100,000 doses). Symptoms classified as moderate, common, and general occurred more often, with fever being the most frequent. Severe induration, hypotonic and hyporesponsive episodes, persistent crying and rashes were observed more frequently than expected.
CONCLUSIONS The rate of adverse events following childhood immunization is similar to that reported in other provinces and elsewhere in the world. Of all childhood vaccines, the pentavalent vaccine is the most reactogenic. The absence of serious adverse events demonstrates the safety of childhood immunization in Cuba.
KEYWORDS Immunization programs, vaccination, surveillance system, adverse events, Cuba
ABSTRACT INTRODUCTIONThe Cuban national program for childhood immunizations began in 1962 and has included a surveillance system for monitoring adverse events following immunization since 1999. The expected rate of adverse events following childhood immunization in Cuba is 50 per 100,000 vaccine doses administered. In 2017, Pinar del Río Province reported higher-than-expected rates of adverse events, which motivated this study on their frequency and types.
OBJECTIVECharacterize adverse events following immunization reported in children in Pinar del Río Province in 2017.
METHODSWe examined reports of adverse events following immunization in children from 2 months through 14 years of age in Pinar del Río Province, Cuba, from January 1, 2017 through December 31, 2017. We found 487 adverse events that met the criteria established by the national surveillance system. Information was obtained from epidemiological surveys of adverse events following immunization in Pinar del Río Province municipalities. Recorded were age, municipality, signs and symptoms, vaccine type, number of doses, anatomical site and route of vaccine administration, and the institution where the child was vaccinated. We estimated proportions for intensity and frequency related to vaccination, and calculated rates for 100,000 vaccine doses administered. We then compared the rates of observed adverse events with those of expected events.
RESULTSThe overall rate of adverse events was 305.6 per 100,000 doses administered. Highest rates were reported in children aged <1 year (580.9 per 100,000 doses administered); in Guane Municipality (610 per 100,000 doses), for the pentavalent (DTwP-HB-Hib) vaccine (1567.7 per 100,000 doses), and in applications to the anterolateral quadrant of the thigh (772.5 per 100,000 doses). Symptoms classified as moderate, common, and general occurred more often, with fever being the most frequent. Severe induration, hypotonic and hyporesponsive episodes, persistent crying and rashes were observed more frequently than expected.
CONCLUSIONSThe rate of adverse events following childhood immunization is similar to that reported in other provinces and elsewhere in the world. Of all childhood vaccines, the pentavalent vaccine is the most reactogenic. The absence of serious adverse events demonstrates the safety of childhood immunization in Cuba.
KEYWORDSImmunization programs, vaccination, surveillance system, adverse events, Cuba
INTRODUCTION With the exception of access to potable water, no other preventive or therapeutic measure has done more than vaccines to reduce morbidity and mortality from communicable diseases worldwide. As a direct result of immunization, diseases like poliomyelitis, diphtheria, pertussis, tetanus, measles, rubella, mumps, and serious complications from neonatal tetanus, congenital rubella syndrome, tuberculosis meningitis or post-parotitis, have ceased to be health problems in Cuba, their transmission rates declining to <0.1 per 100,000 vaccine doses.[1] Despite these benefits, adverse events following immunization must be monitored and recorded to ensure vaccine safety.
The term ‘immunization’ in this text refers to the use of preventive vaccines for the purpose of conferring protection against certain diseases. This term includes all processes that occur after a vaccine product leaves its place of manufacture and packaging, including handling, prescription and administration.
IMPORTANCE This paper reviews and analyzes data from a Cuban province that reported higher-than-expected adverse events following childhood immunization in 2017. Evaluation offers further evidence of vaccine safety for children in the Cuban National Immunization Program.
Safe vaccination is an essential component of immunization programs, which are responsible for regulating vaccine quality; transportation and storage at appropriate temperatures (2 °C–8 °C); inoculation practices that pose minimal risks to recipients, health workers administering the vaccine and the environment; as well as surveillance of adverse events attributable to vaccination or immunization.[1–3]
An adverse event following immunization (AEFI) is defined as any untoward medical occurrence which follows vaccination or immunization, even if it does not have a causal relationship with the vaccine.[4–7] WHO specifies that any signs, symptoms, diseases, altered laboratory results, or other unfavorable events can be considered AEFIs. These also include application of megadoses, changes in vaccines or vaccine diluents, and administration at the wrong site or via the wrong route—whether or not these events have a later clinical manifestation.[6]
In 2016, WHO classified AEFIs as follows: according to intensity of clinical presentation (mild, moderate or severe); whether the event was localized or general; by frequency of occurrence; and according to the event’s clinical implications (serious or not serious). AEFIs are classified in five categories according to their cause or origin: whether the event is related to vaccine components; with defects in its quality; with errors in vaccine administration; with manifestations of anxiety in the vaccinated child; or as coincidental, defined as an event not included in the previous four categories.[6,8]
An AEFI is considered non-serious when it does not represent a potential risk to the recipient’s health, although it must be monitored carefully because it may indicate a potential problem with the vaccine or with the immunization process, and thus may impact vaccination acceptance in general. An AEFI is considered serious if it causes death; endangers life; requires hospitalization or prolongs existing hospitalization; causes a persistent or significant disability or incapacity; results in a congenital abnormality or defect; or requires intervention to prevent deterioration or permanent damage.
An event is classified as coincidental if it coincides temporarily with immunization, which sometimes implies mistakenly attributing the event to the vaccine. Examples of coincidental events include: manifestation or complication of an underlying congenital or hereditary disease or birth injury; manifestation or complication of an underlying acquired disease that may or may not have been diagnosed prior to vaccination; psychogenic disease; adverse reactions to recent or concomitant medications or use of illicit substances; allergic reactions and other hypersensitivity reactions due to exposure to allergens other than those present in the vaccine; injury from exposure to environmental toxins; and injuries attributable to trauma, including surgery.[6,8]
It is important that health personnel involved in vaccination be aware of adverse events that may occur after vaccine administration, to be able to protect the vaccinated as well as to respond to public concerns about immunization and reducing the influence of anti-vaccine movements. Disinformation spread by these movements has contributed to a decrease in vaccine coverage in some countries, resulting in re-emergence of communicable diseases that were once eliminated.[9]
The AEFI passive surveillance system was implemented in Cuba in 1999 at the primary care level with the purpose of identifying and reporting all adverse events in accordance with methodology established by the Center for State Control of Medicines and Medical Devices (CECMED), the Cuban regulatory authority.[10–13]
AEFI surveillance is carried out in all Cuban provinces, but there are differences in notification rates.[11,14] In 2017, as in previous years, Pinar del Río Province reported higher AEFI rates in the child population than those expected (the expected AEFI rate in Cuba is 50 per 100,000 doses administered); however, these AEFI had not been characterized with the purpose of comparing them with other territories and with reports made in subsequent years as part of vaccine post-marketing surveillance.
This study was aimed at characterizing AEFI in children in Pinar del Río Province, Cuba, in 2017 and identifying factors related to their occurrence. The results of this research are part of a larger project that includes several years of monitoring and characterization of AEFI in the Cuban National Immunization Program.
METHODS Study design and participants We examined 585 AEFI notifications for children in Pinar del Río Province from January 1 through December 31, 2017. This study was carried out as part of a project examining provinces with the highest rates of AEFIs in years prior to 2019.
We included 487 AEFI reports in children aged 2 months to 14 years who met the case definitions established by the Cuban surveillance system[15] and the Brighton Collaboration.[16–21] AEFIs were not reported in children younger than 2 months or older than 14 years.
Information on sociodemographic and clinical data, the type of vaccine and vaccination procedures, and the AEFI in question were obtained through a document review of primary sources (an epidemiological survey of adverse events to vaccination).[11]
We collected the following sociodemographic variables: age (≥2 months and <1 year; 1–4 years; 5–9 years; 10–14 years) and municipality (Sandino, Mantua, Minas de Matahambre, Viñales, La Palma, Los Palacios, Consolación del Sur, Pinar del Río, San Luis, San Juan y Martínez, and Guane).
AEFIs considered in the study were: reports of pain, mild redness and induration; cellulitis or severe induration at injection site (induration in the puncture area that lasted more than 72 hours, or presented with edema past the nearest joint); fever; persistent crying; rash; episodes of hyporesponsive hypotonia (EHH); irritability; and general malaise. These criteria were established according to guidelines published by the Medical University of Havana.[11]
We recorded the following variables related to vaccines and vaccine administration procedures:
type of vaccine: pentavalent (DTwP: diptheria–tetanus–whole cell pertussis; HB: hepatitis B; Hib (Haemophilus influenzae type b); OPV (oral polio vaccine); IPV (intramuscular polio vaccine); AM-BC (meningococcal–BC); MMR (measles–mumps–rubella); DTwP (diptheria–tetanus–whole cell pertussis); DT (diptheria–tetanus); AT (typhoid fever); TT (tetanus toxoid); and AG (influenza)
ordinal number of vaccine does: first dose or single dose, second dose, third dose, and reactivation or booster
route of administration: oral, subcutaneous, intradermal or intramuscular
anatomical region of application: by mouth, deltoid or middle third of the anterolateral quadrant of the thigh
location of application: vaccination center of a community polyclinic, school, or hospital
We classified AEFIs into the following frequencies of those vaccinated:
very common: >10%
common: ≥1%–10%
infrequent: ≥0.1%–<1%
rare: ≥0.01%–<0.1%
very rare: <0.01%
We classified AEFIs according to their location as follows:
local: pain, redness and induration; cellulitis; or severe induration at the injection site
general: fever; malaise; irritability; rash; persistent crying; and EHH
We classified AEFIs according to the intensity of the clinical picture:
mild: pain, redness and slight induration at or near the injection site <5 cm2, lasting 24–48 hours; fever of 38 °C–38.9 °C; general malaise; irritability; and rash
moderate: cellulitis in the deltoids or anterolateral quadrant of the thigh 5–10 cm2, lasting 48–72 hours; fever of 39 °C–39.9 °C; and persistent crying
severe: severe induration of the puncture area >10 cm2, or induration that went past the nearest joint, lasting >72 hours; fever ≥40 °C; and EHH
AEFIs were classified according to the following clinical implications:
serious: symptoms and signs resulted in prolonged hospitalization, in persistent or significant disability, if they endangered life, or if they resulted in the death of the child
not serious: symptoms and signs did not result in any of the above consequences
Hospitalizations that were not prolonged were excluded from the serious category, because according to the regulations of Cuba’s Maternal–Child Health Program, children under one year of age who are seen by emergency services are evaluated and hospitalized regardless of the AEFI in question.
Finally, AEFIs were classified according to cause or origin as follows:
related to vaccine components (mild pain, redness and induration at the injection site, fever, general malaise, irritability, rash, persistent crying, EHH)
related to procedural errors (cellulitis and severe induration at the injection site)
coincidental: any event not included in the previous categories
Data analysis Observed AEFI rates were calculated per 100,000 vaccine doses administered (DA) to compare them with expected rates, in accordance with methodology recommended by WHO.[22] The observed rates are the sum of the average rates plus the effect of the vaccine, and the expected rate is the rate described for each vaccine according to the WHO Global Manual for Adverse Events Surveillance.[6]
Ethics This project was approved by the research ethics committees of the Pedro Kourí Tropical Medicine Institute in Havana and Pinar del Río Provincial health authorities. Anonymity and confidentiality of information were assured.
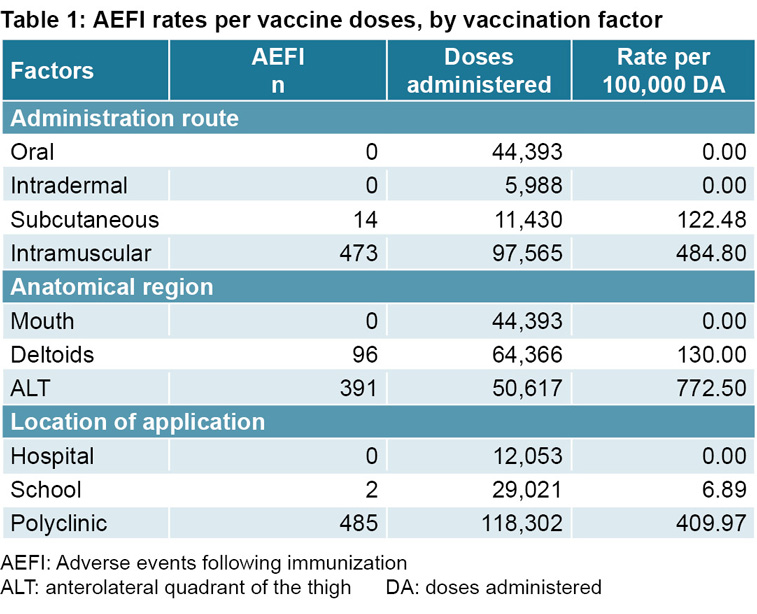
RESULTS In 2017, Pinar del Río Province reported 585 AEFIs in children to the national surveillance system. Of these, 487 were complete and useful for our analysis. In 2017, 159,376 doses of vaccines were given to children in the province, so the general AEFI rate was 305.6 per 100,000 DA. AEFI rates were broken down by administration route, anatomical region, and location where the vaccines were administered (Table 1).
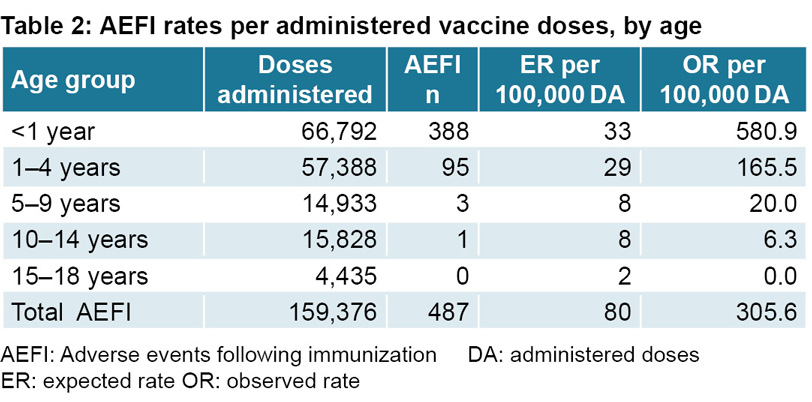
The observed AEFI rate was higher than expected in children aged <5 years, and the greatest difference between observed and expected rates occurred in children aged <1 year.
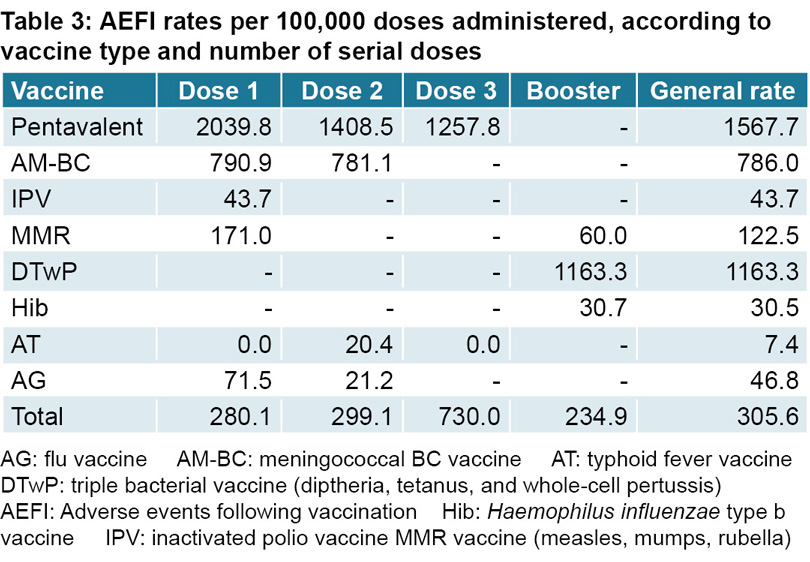
By municipality (data not tabulated), Guane Municipality had the highest AEFI rate at 715.5 per 100,000 DA. Mantua (570.7 per 100,000 DA), Minas de Matahambre (561.7 per 100,000 DA), La Palma (485.9 per 100,000 DA) and Los Palacios (608.4 per 100,000 DA) registered values above the provincial average of 305.6 per 100,000 DA. Sandino (298.2 per 100,000 DA), Pinar del Río (207.6 per 100,000 DA) and Consolación del Sur (193.7 per 100,000 DA) remained below that value. Viñales and San Juan y Martínez municipalities did not report AEFIs. An increase in the general rate to 336.9 AEFI per 100,000 DA was reported in Pinar del Río province for seven vaccines within the national vaccine program and for the influenza vaccine given to pediatric groups at risk for influenza-like illness. Rates higher than the provincial average were found for the pentavalent vaccines (in each of its three doses and in total), the DTwP reactivation booster and AM-BC (in both its two doses and in the total). For OPV, PRS, Hib, AT, and AG, rates below the provincial average were recorded, and no events were reported for BCG, HB, OPV, DT, and TT (Table 3).
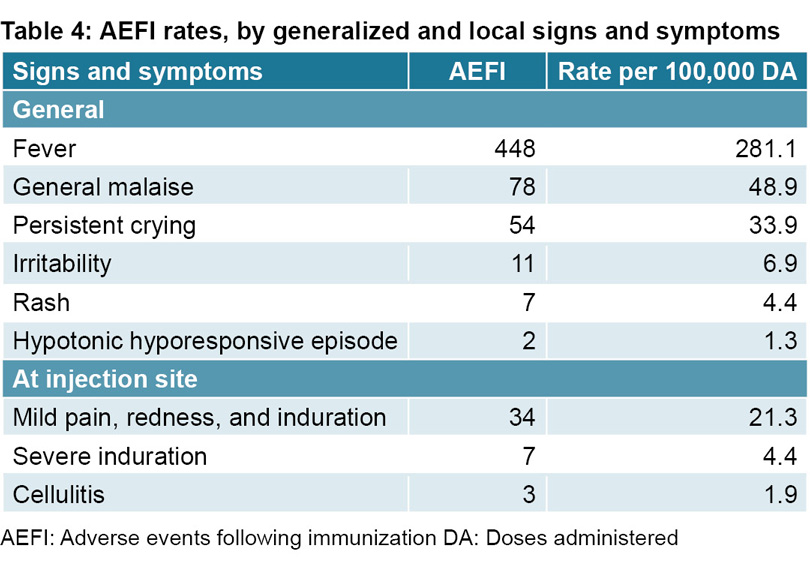
A total of 644 signs or symptoms were identified, an average of 1.3 for each reported AEFI (487). General signs and symptoms were the most common (93.1%). Fever was the most frequently reported sign or symptom, and EHH the most infrequent. The remaining 6.9% of signs or symptoms were local, with the highest rates corresponding to pain, redness and mild induration, followed by severe induration and cellulitis (Table 4).
Of all reported signs and symptoms, 71.5% were classified as moderate (mainly fever), 26.3% as mild, and 2.0% as severe. No serious events were reported. Three children were hospitalized for fever, their average length of stay was two days, and they had no other complications.
No AEFI was classified as very common; 53.1% were classified as common, 36.8% as infrequent, 9.7% as rare and 0.3% as very rare. The most commonly categorized AEFI was fever, and EHH was categorized as a very rare event.
Vaccine components caused 92.3% of reported AEFI, 6.1% were coincidental and 1.5% were classified as errors in vaccine administration. Cellulitis and severe induration were both considered the result of errors in vaccine administration. Fever secondary to the PRS vaccine was considered to be coincidental, since the reported febrile episodes appeared in the first 72 hours after vaccination and could not be attributed to known causes.
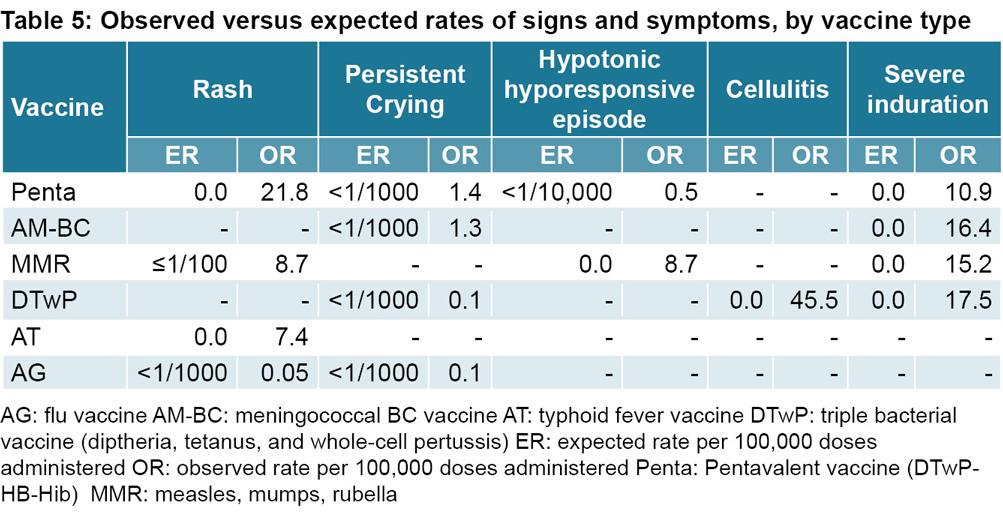
Fever, malaise, and irritability had lower rates than expected for all vaccines, while rash, persistent crying, EHH, cellulitis and severe induration were reported at values higher than expected for vaccines (Table 5).
DISCUSSION AEFI recording and analysis is an important step in post-marketing vaccine surveillance.[22]
The AEFI rate in our research is similar to those reported in other studies in Cuba. Galindo reported a rate of 106 events per 100,000 DA in Pinar del Río Province and 115 in Sancti Spíritus Province.[14] González obtained annual rates of 119–604 per 100,000 DA in the Isle of Youth Special Municipality,[23] and Mantecón identified 150 events per 100,000 DA in Camagüey Province.[24]
The rates in our study were higher than those found by Guo in a systematic meta-analysis that included 33 studies conducted in China and other countries, based on an international comparison of AEFI reporting rates divided by pediatric age group.[25] Our rates were also higher than those reported by other investigations carried out at different times in populations that use passive surveillance, by populations that perform their data analysis according to doses administered (not distributed), and who have vaccine schedules similar to those in Cuba.[26–31]
The high AEFI rates in Pinar del Río could be attributed to Cuba’s surveillance system, which identifies and reports all events that occur within the vaccinated community, which leaves little margin for underreporting. This makes the Cuban vaccination surveillance system highly sensitive.
However, since high rates are not always the result of high sensitivity in surveillance systems, it is important to consider both relevance of the reported cases and data quality in addition to the number of notifications. These values could be influenced by average rates of certain signs and symptoms that occur within the community which could be considered AEFI if they appear after vaccination.
A higher frequency of events was recorded in children under one year of age. Other investigations carried out in Cuba[10,14,23] and in other countries[30–33] describe similar results, although other research has found higher AEFI rates in other pediatric age groups.[26,27]
The first year of life is a period of rapid body transformation when the immune system is also rapidly maturing.[34] During this period, alterations to expected growth and development patterns caused by underlying congenital diseases can occur, acquired diseases can be more serious, and reactions to drugs can be more diverse. Children also receive the highest number of vaccine doses during their first year, so it is entirely possible that many medical incidents could occur following a routine vaccination, even if such incidents were not caused by the vaccine.
The differences observed in AEFI rates and patterns between Cuba and other countries could be explained by differing population compositions, by the fact that some countries rely on different vaccination schedules, and because each country’s vaccines have different origins and rely on different production technologies. In Cuba, for example, most of the immunobiologicals used in the Cuban population are produced domestically, while other countries often purchase vaccines from international pharmaceutical firms. In Brazil, to give another example, the group most affected by AEFI were children between the ages of one and four years old, and the national vaccine schedule includes a tetraviral vaccine (measles–mumps–rubella–varicella) administered during that period, as well as a vaccine for hepatitis A[26] that is not administered in Cuba. In Canada, the highest rates of AEFI are reported in children between the ages of one and two, and the immunization schedule includes both the tetraviral vaccine and a live attenuated influenza vaccine.[27]
In Pinar del Río, 82% of municipalities reported adverse events during the study period, a rate similar to that found in Camagüey Province in eastern Cuba (84.6%),[24] and higher than those reported in other countries.[26,35] In Cuba, AEFI surveillance and notification is the responsibility of physicians and nurses in family practice at the primary healthcare level.[14] Surveillance increases confidence in vaccine programs, completes the safety profile of vaccines during the post-marketing stage, guarantees that detection of problems related to vaccine use is accompanied by preventive and corrective actions, and favors communication with the professionals responsible for both designing and administering vaccines and with the families who receive them. Underreporting of AEFIs reveals weaknesses in the surveillance system and calls into question the results of investigations.
The vaccines combined with DTP were the most reactogenic, as seen in results of previous research in Cuba[10,14,22,24,36] and in other countries.[25,33,37,38] However, the Republic of Korea reports more AEFIs for the BCG vaccine,[29] Australia reports more for the seasonal influenza vaccine[33] and China reports higher rates for the measles vaccine.[32]
It is well established in the literature that vaccines combined with DTP are the most reactogenic, especially those that contain the whole-cell pertussis component.[4,6] The pentavalent and DTP vaccines used in Cuba are produced nationally, include whole cells and are considered the most reactogenic of all vaccines in the Cuban vaccine schedule. Internationally, other formulations use acellular DTP which is less reactogenic but more expensive and less effective.[14]
The highest AEFI rates were reported for the first dose of different vaccines, for those administered intramuscularly, those administered in the anterolateral quadrant of the thigh, and those administered in polyclinics. These results coincide with those reported in national Cuban studies[24,36,39,40] and by other countries.[32,41–43]
As outlined by the standards published in the Expanded Program on Immunizations[44] the route of administration of immunobiologicals is specific to each immunobiologic compound, and each has recommendations for optimal techniques designed to reduce adverse events resulting from errors in administration.[45–47] The higher rates observed in the intramuscular route of administration could be due to the fact that it is used for the DTP and pentavalent vaccines—which carry the highest rates of AEFIs reported in this study—or because recommended optimal techniques for administration of these particular compounds were not followed. These guidelines indicate the anatomical region in which each vaccine should be injected to ensure that damage to tissue, nerves, veins and arteries is minimal. The higher rates of AEFIs associated with vaccine administration to the anterolateral quadrant of the thigh could be due to the fact that it is the anatomical site that requires the greatest navigational expertise from vaccinators.
The greater number of AEFIs registered during polyclinic vaccinations could be due to the fact that polyclinics are the places that administer the highest number of vaccine doses in the Cuban program (11 of 18 total vaccine doses in the national childhood vaccination schedule), and community-based polyclinics allow for closer post-vaccination observation and thus often better management of AEFIs by health professionals.
Common and general signs and symptoms occurred more frequently, with fever the most often reported symptom. Some researchers report similar findings,[10,14,23,26] while other studies found a higher frequency of local events.[27,29,30–33] Moderate and mild intensity AEFIs were reported more frequently, which coincides with results of other national[10,14,23] and international studies,[30] with the exception of reports from Colombia (with 76% events classified as severe).[48] No AEFI in this study was classified as severe, consistent with some authors[24] but differing from others, both in Cuba and internationally.[14,23,26,35]
Differences in AEFI frequency and location may be due at least in part to the fact that some AEFIs result from physiological inflammatory responses intrinsic to the organism’s innate immune system; may be due to factors such as individual susceptibility, different types of vaccines, vaccine composition; or can be the result of program errors.[4,49,50] Clinical manifestations can be localized at the injection site or can be systemic. The higher prevalence found in our study for general AEFIs is explained by the high rate reported for the pentavalent vaccine, for which systemic events are more common than local ones.[50]
Our results coincide with the literature reporting higher frequencies of mild AEFIs.[4,5] As there were no severe AEFIs, we can conclude that the vaccines administered in the country are safe, and that risks to pediatric patients following administration of immunobiologic agents are extremely low.
Signs and symptoms were related to vaccines, immunization errors, or to a lesser extent, were coincidental, similar to behavior described in other investigations.[14,52] Establishing or ruling out causal relationships between appearance of signs and symptoms and vaccine administration is a complex process, especially in young children. It requires considering aspects of the episode, establishing a chronological relationship with exposure to the vaccine according to the underlying pathophysiology, and the possible effects of other causal agents or conditions.[52]
The low rate of events related to immunization errors speaks to the competence of Pinar del Río’s health professionals and the quality of processes related to correct administration procedures for vaccination, as these are preventable events. AEFIs related to the vaccines themselves cannot be avoided, as they depend on factors related to vaccine components or the innate susceptibilities of the vaccinated population.
In this study, some signs and symptoms occurred at higher rates than would have been expected. AEFI secondary to immunization are considered expected when there is substantiated or consistent information on what may occur, and otherwise unexpected, regardless of whether they are related to vaccine administration.[52]
The higher-than-expected rates we observed could be due to a study limitation, as the average rates of the signs and symptoms examined in the reference population are unknown. This made the proportion of AEFIs related to the vaccine impossible to separate entirely from the portion unrelated to vaccination. False positive cases (those not due to vaccines) could also have been reported, which is common in passive surveillance systems or because, as explained above, the system in question has little room for underreporting.
CONCLUSIONS The rates of AEFI in the population studied do not show relevant clinical-epidemiological differences with those reported in Cuba as a whole or in other countries, and the absence of serious events demonstrates the low risk presented by the childhood vaccines included in the Cuban National Vaccination Program.
López Ambrón L, Egües Torres LI, Pérez A, Galindo BM, Galindo MA, Resik S, et al. Experiencia cubana en inmunización, 1962–2016. Rev Panam Salud Pública [Internet]. 2018 [cited 2017 Nov 22];42(34):40–8. Available at: https://doi.org/10.26633/RPSP.2018.34. Spanish.
Rodríguez A, Zunino C, Speranza N, Fernández S, Varela A, Picón T, et al. Seguimiento de eventos supuestamente atribuibles a la vacunación e inmunización graves notificados al Ministerio de Salud Pública entre 2010 y 2014. Rev Méd Urug [Internet]. 2017 [cited 2018 Jun 6];33(1):47–58. Available at: http://www.rmu.org.uy/revista/2017v1/art6.pdf. Spanish.
Secretaría de Salud. Manual de Eventos Supuestamente Atribuibles a la Vacunación o Inmunización. 1st ed [Internet]. Mexico, D.F.: Editorial Soluciones Gráficas Lithomat; 2014 Jun [cited 2018 Mar 9]. p. 7–14. Available at: https://www.gob.mx/cms/uploads/attachment/file/287240/ESAVI_2014.pdf. Spanish.
Spanish Paediatric Association. Manual de vacunas en línea de la AEP [Internet]. Madrid: Spanish Paediatric Association; c1999–2019. Section 1, Chapter 5.2 Efectos adversos de las vacunas; [cited 2017 Dec 15]. Available at: https://vacunasaep.org/documentos/manual/cap-5. Spanish.
World Health Organization [Internet]. Geneva: World Health Organization; c2020. Iniciativa global sobre la seguridad de las vacunas. Eventos adversos posvacunales; [updated 2015 Apr 1; cited 2017 Dec 12]. Available at: http://www.who.int/vaccine_safety/initiative/detection/AEFI/es/. Spanish.
Ministry of Health (PE). Centro Nacional de Epidemiologia, Prevención y Control de Enfermedades. Vigilancia de ESAVI [Internet]. Lima: Ministry of Health (PE); 2013 [cited 2018 Jun 22]; [about 2 screens]. Available at: http://www.dge.gob.pe/portal/index.php?option=com_content&view=article&id=432&Itemid=109. Spanish.
Díaz Pinera AM, Cuevas Valdespino IE. Eventos adversos en la vacunación de menores de 2 años, Hospital Pediátrico de Centro Habana (2002-2007). Rev Cubana Hig Epidemiol [Internet]. 2014 [cited 2017 Nov 7];52(1):81–97. Available at: http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S1561-30032014000100008&lng=es&nrm=iso. Spanish.
Galindo BM. Diseño, implementación y evaluación de la vigilancia de eventos adversos a vacunas en Cuba. 1999-2010 [thesis] [Internet]. [Havana]: University of Medical Sciences of Havana; 2017 [cited 2017 Nov 22]. 135 p. Available at: http://tesis.sld.cu/index.php?P=FullRecord&ID=216. Spanish.
Cruz Martínez G, Verdasquera Corcho D, Corcho Quintero A, Delgado Díaz OL, Díaz Fuentes C, Carbó Riverón M. Eventos adversos de la vacuna cubana antimeningocóccica. Rev Cubana Med Gen Integr [Internet]. 2011 Apr–Jun [cited 2019 Jun 13];27(2):187–96. Available at: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252011000200007&nrm=iso. Spanish.
Center for State Control of Medicines and Medical Devices – CECMED (CU). Regulación No. 17 – 2008. Directrices para la investigación de los eventos adversos supuestamente atribuibles a la vacunación o inmunización (ESAVI) [Internet]. Havana: Ministry of Public Health (CU); 2008 [cited 2017 May 14]. 27 p. Available at: http://www.cecmed.cu/reglamentacion-vigilancia?page=1. Spanish.
Gidudu J, Kohl KS, Halperin S, Hammer SJ, Heath PT, Hennig R, et al. A local reaction at or near injection site: case definition and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine [Internet]. 2008 [cited 2018 Apr 10];26(52):6800–13. Available at: https://www.sciencedirect.com/science/article/pii/S0264410X08013868
Buettcher M, Heininger U, Braun M, Bonhoeffer J, Halperin S, Heijbel H, et al. Hypotonic-hyporesponsive episode (HHE) as an adverse event following immunization in early childhood: case definition and guidelines for data collection, analysis, and presentation. Vaccine [Internet]. 2007 Aug 1 [cited 2018 Apr 10];25(31):5875–81. Available at: https://www.sciencedirect.com/science/article/pii/S0264410X07005026?via%3Dihub
González Fiallo S, Bell Morales B, García Sanz D, Moreno Gell M. Eventos adversos supuesta mente atribuidos a la vacunación o inmunización. Isla de la Juventud, Cuba, enero/2013-octubre/2016. VacciMonitor [Internet]. 2017 [cited 2019 Jan 28];26(3):102–9. Available at: http://www.redalyc.org/articulo.oa?id=203454509005. Spanish.
Mantecón MC. Evaluación del sistema de vigilancia de eventos adversos a la vacunación en la provincia Camagüey, 2016 [thesis]. [Havana]: Dr Pedro Kourí Institute of Tropical Medicine; 2018. Spanish.
Guo B, Page A, Wang H, Taylor R, McIntyre P. Systematic review of reporting rates of adverse events following immunization: an international comparison of post-marketing surveillance programs with reference to China. Vaccine [Internet]. 2013 Jan 11 [cited 2019 Jan 3];31(4):603–17. Available at: http://dx.doi.org/10.1016/j.vaccine.2012.11.051
Caselli F, Santos CMA, Kalume AG, Deotti SM, da Silva AM, Moreira R, et al. Análise do Sistema de Informação da Vigilância de Eventos Adversos Pós-Vacinação no Brasil, 2014 a 2016. Rev Panam Salud Pública [Internet]. 2018 [cited 2018 Jun 21];42(12):1–12. Available at: https://doi.org/10.26633/RPSP.2018.12. Portuguese.
Law BJ, Laflèche J, Ahmadipour N, Anyoti H. Canadian Adverse Events Following Immunization SurveillanceSystem (CAEFISS): Annual report for vaccines administered in 2012. CCDR [Internet]. 2014 Dec 4 [cited 2018 Jun 29];40(3). Available at: https://doi.org/10.14745/ccdr.v40is3a02
Alicino C, Merlano C, Zappettini S, Schiaffino S, Della Luna G, Accardo C, et al. Routine surveillance of adverse events following immunization as an important tool to monitor vaccine safety. The two-years’ experience of the Liguria Region, Italy. Hum Vaccin Immunother [Internet]. 2015 Jan [cited 2018 Jun 29];11(1):91–4. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4514437/
Kim M-K, Lee YK, Kim TE, Kong I, Yang H-J, Suh ES. Surveillance and compensation claims for adverse events following immunization from 2011 to 2016 in the Republic of Korea. Clin Exp Vaccine Res [Internet]. 2017 Jul [cited 2018 Jun 29];6(2):146–55. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5540963/
Dey A, Wang H, Quinn H, Cook J, McCartney K. Annual report: surveillance of adverse events following immunization in Australia, 2015. Commun Dis Intell [Internet]. 2017 Sep [cited 2018 Dec 11];41(3):E264–78. Available at: http://www.health.gov.au/internet/main/publishing.nsf/Content/cdi4103-l
Deverell M, Phu A, Zurynski Y, Elliott E; APSU Surveillance Studies investigators. Australian Pediatric Surveillance Unit Annual Report, 2016. Commun Dis Intell [Internet]. 2017 Sep [cited 2018 Dec 11];41(3):E288–93. Available at: http://www.health.gov.au/internet/main/publishing.nsf/Content/cdi4103-l
González V, Gutiérrez S, Quian J. Eventos adversos supuestamente atribuibles a la vacunación e inmunización en hijos de madres infectadas con el virus de la inmunodeficiencia humana. Arch Pediatr Urug [Internet]. 2013 [cited 2019 Jan 15];84(1):4–9. Available at: http://www.scielo.edu.uy/scielo.php?script=sci_arttext&pid=S1688-12492013000100002&lng=es. Spanish.
Pérez JA. Evaluación del sistema de vigilancia de eventos adversos a la vacunación. La Lisa, 2015 [thesis]. [Havana]: University of Medical Sciences of Havana; 2017. Spanish.
González Montiel AR. Evaluación del Sistema de Farmacovigilancia utilizado en México, 2012 [thesis]. [Cuernavaca]: National Institute of Public Health (MX); 2012 [cited 2019 Jan 15]. 63 p. Available at: http://catalogoinsp.mx/files/tes/052574.pdf. Spanish.
Alfonso OL, Pérez E. Comportamiento del ensayo clínico de la vacuna pentavalente en la Policlínica Docente Área Norte de Placetas. Rev Acta Médica Centro [Internet]. 2010 [cited 2018 Dec 9];4(3). Available at: http://www.revactamedicacentro.sld.cu/index.php/amc/article/view/514/682. Spanish.
Zafack Guetsop J, De Serres G, Kiely M, Gariepy MC, Rouleau I, Anne-Marie K, et al. Risk of recurrence of adverse events following immunization: a systematic review. Pediatrics [Internet]. 2017 Sep [cited 2018 Dec 9];140(3):e20163707. Available at: http://pediatrics.aappublications.org/content/140/3/e20163707
Principios generales de inmunización. Cap.VIII. In: Normas y Procedimientos del Programa Ampliado de Inmunizaciones (PAI) de Honduras [Internet]. Tegucigalpa: Secretaria de Salud; 2011 Jul [cited 2017 Nov 22]. p. 24–5. Available at: http://www.bvs.hn/Honduras/PAI/ManualNormasyProcedimientos/MNPPAIH1-7.pdf. Spanish.
Merino M, Bravo J. Generalidades sobre vacunas: cosas prácticas. In: AEP. Curso de Actualización Pediatría 2018. Madrid: Lúa Ediciones 3.0; 2018. p. 67–76. Spanish.
Diggle L, Deeks J. Effect of needle length on incidence of local reactions to routine immunisation in infants aged 4 months: randomised controlled trial. BMJ [Internet]. 2000 Oct 14 [cited 2018 Mar 9];321(7266):931–3. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/11030682/. Spanish.
World Health Organization [Internet]. Geneva: World Health Organization; c2020. Vaccine safety basics e-learning course. Adverse events fallowing immunization; 2018 [cited 2018 Jun 20]. Available at: http://vaccine-safety-training.org/vaccine-reactions.html
THE AUTHORS Elba Cruz-Rodríguez (Corresponding author: elba@ipk.sld.cu; elbacr@infomed.sld.cu), physician with dual specialties in family medicine and epidemiology, and a master’s degree in epidemiology. Associate professor and adjunct researcher, Epidemiological Surveillance and Research Department, Pedro Kourí Tropical Medicine Institute (IPK), Havana, Cuba. https://orcid.org/0000-0002-9322-0875
Belkys María Galindo-Santana, physician with dual specialties in family medicine and epidemiology, a master’s degree in epidemiology and a doctorate in the medical sciences. Senior researcher and full professor, Epidemiological Surveillance and Research Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-8757-4036
Waldemar Baldoquín-Rodríguez, physician with dual specialties in family medicine and biostatistics. Assistant professor and associate researcher, Epidemiological Surveillance and Research Department, IPK, Havana, Cuba. https://orcid.org/0000-0001-9231-7109
Dayana Rodríguez-Velázquez, geographer, Epidemiological Surveillance and Research Department, IPK, Havana, Cuba. https://orcid.org/0000-0002-6473-5650Damarys Concepción-Díaz, laboratory technician specializing in computer sciences, Epidemiological Surveillance and Research Department, IPK, Havana, Cuba. https://orcid.org/0000-0003-2403-6801
Miriam Caridad Luis-Martínez, physician with dual specialties in family medicine and epidemiology, and a master’s degree in satisfactory longevity, Provincial Hygiene, Epidemiology and Microbiology Center, Pinar del Río, Cuba. https://orcid.org/0000-0001-7896-8837
Submitted: April 24, 2020 Approved: December 20, 2020 Disclosures: None
Cruz-Rodríguez E, Galindo-Santana BM, Baldoquín-Rodríguez W, Rodríguez-Velázquez D, Concepción-Díaz D, Luis-Martínez MC. Characterization of adverse events following childhood immunizations in Pinar del Río. MEDICC Rev. 2021 Jan;23(1):35–42. Available at:
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.